
Detection of Microcalcifications in Spiral Breast Computed Tomography with Photon-Counting Detector Is Feasible: A Specimen Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Imaging Technique
2.3. Image Reconstruction of SBCT and DBT
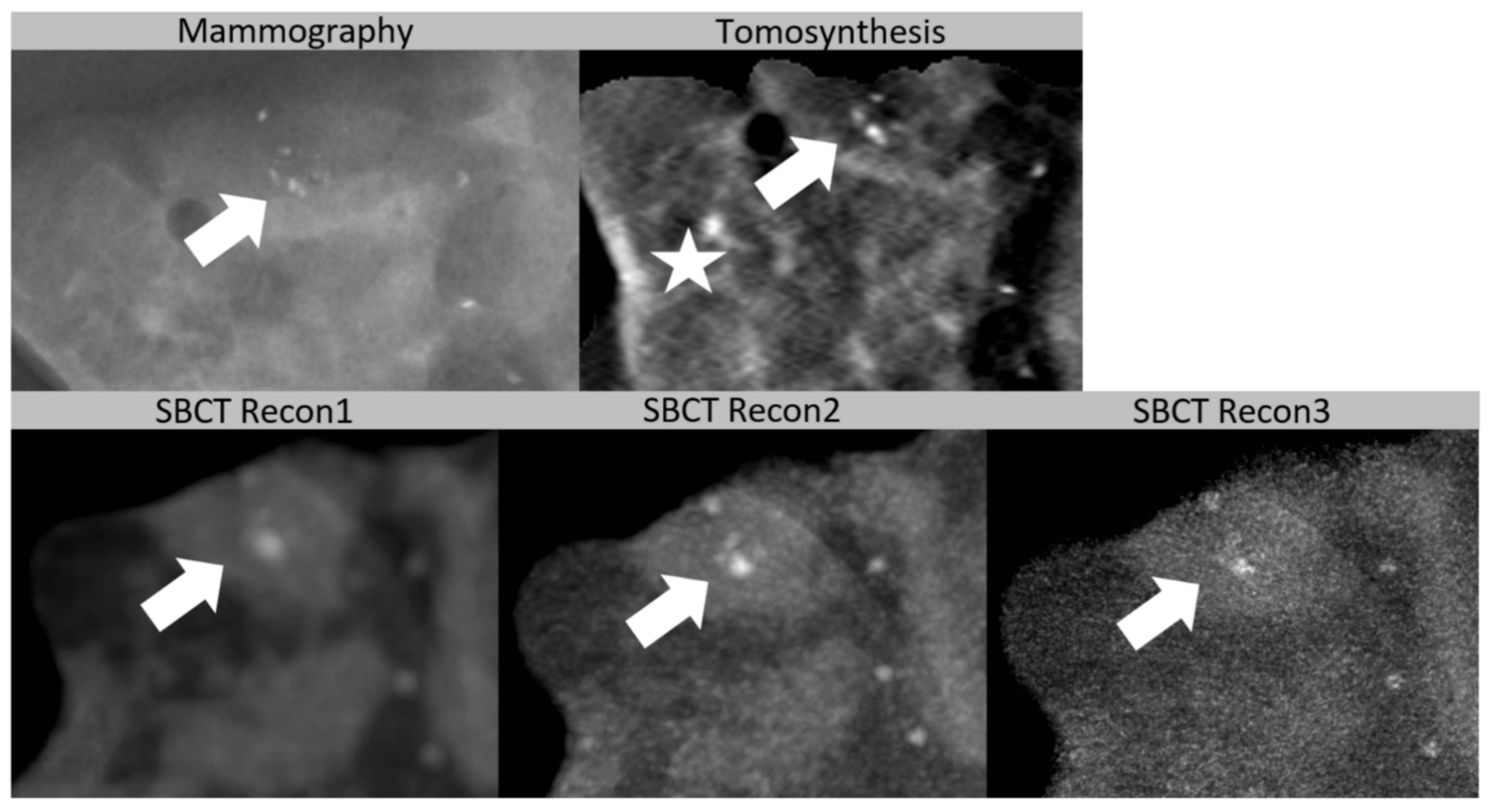
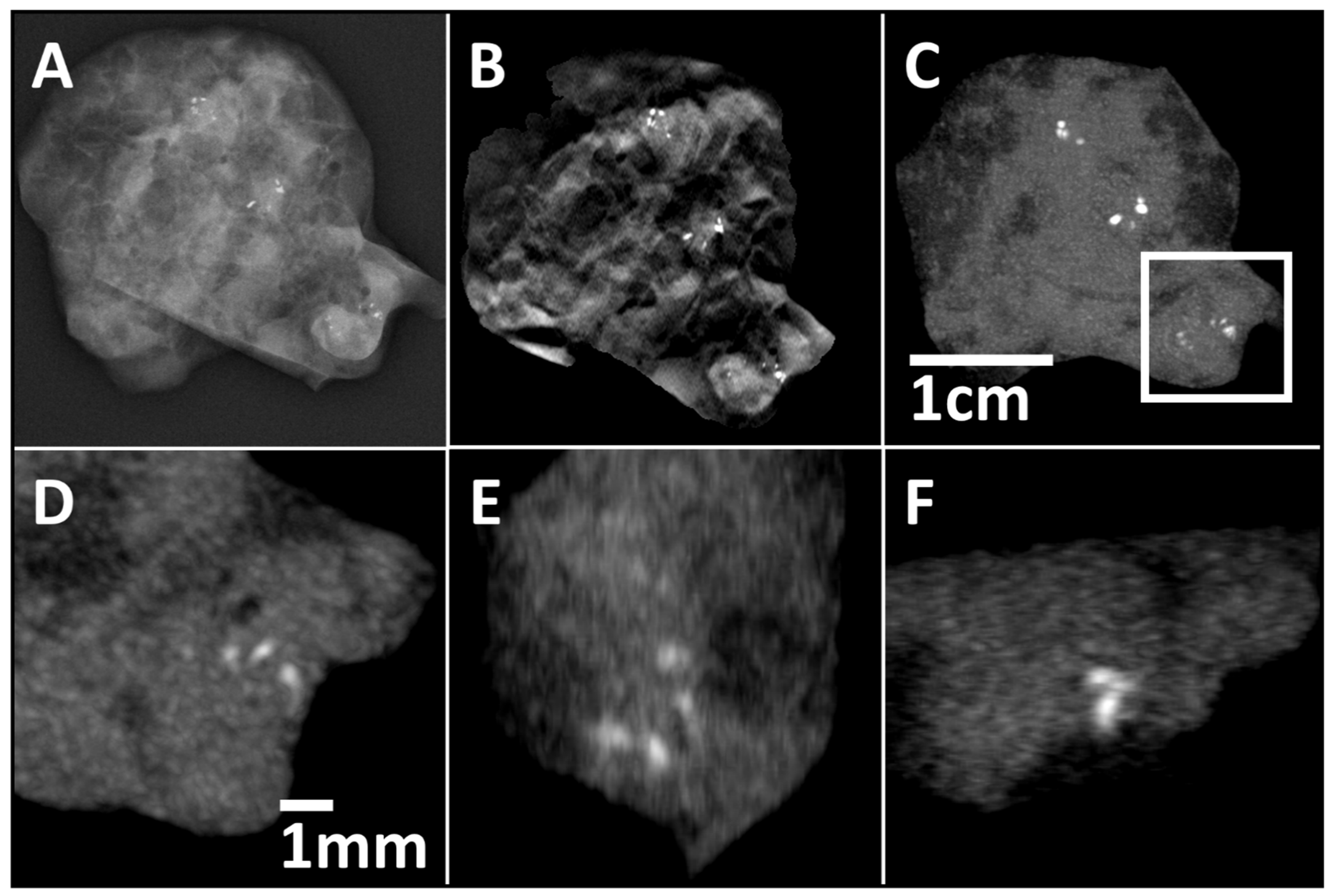
- Recon1: voxel size of (0.15 mm)3, smooth kernel, 2 × 2 detector binning, reconstruction time of 8 min.
- Recon2: voxel size of (0.05 mm)3, smooth kernel, 1 × 1 detector binning, reconstruction time of 15 min.
- Recon3: voxel size of (0.05 mm)3, sharp kernel, 1 × 1 detector binning, reconstruction time of 15 min.
2.4. Reference Standard
2.5. Image Analysis
2.6. Statistical Analysis
3. Results
3.1. Reference Standard
3.2. Detection of Microcalcifications
3.3. Classification as Cluster
3.4. Classification as Diffuse Microcalcification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- D’Orsi, C.J.; Sickles, E.A.; Mendelson, E.B.; Morris, E.B.; Creech, W.E.; Butler, P.F.; Wiegmann, P.G.; Chatfield, M.B.; Meyer, L.W.; Wilcox, P.A. Breast Imaging Reporting and Data System; ACR BI-RADS® Atlas; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Tot, T.; Gere, M.; Hofmeyer, S.; Bauer, A.; Pellas, U. The clinical value of detecting microcalcifications on a mammogram. Semin. Cancer Biol. 2019, 14, 1044-579X. [Google Scholar] [CrossRef]
- Weigel, S.; Decker, T.; Korsching, E.; Hungermann, D.; Böcker, W.; Heindel, W. Calcifications in Digital Mammographic Screening: Improvement of Early Detection of Invasive Breast Cancers? Radiology 2010, 255, 738–745. [Google Scholar] [CrossRef] [PubMed]
- D’Orsi, C.J. Early detection of breast cancer: Mammography. Breast Cancer Res. Treat. 1991, 18, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Mandelson, M.T.; Oestreicher, N.; Porter, P.L.; White, D.; Finder, C.A.; Taplin, S.H.; White, E. Breast density as a predictor of mammographic detection: Comparison of interval- and screen-detected cancers. J. Natl. Cancer Inst. 2000, 92, 1081–1087. [Google Scholar] [CrossRef]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: An analysis of 27,825 patient evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.U.; Chang, J.M.; Bae, M.S.; Lee, S.H.; Cho, N.; Seo, M.; Kim, W.H.; Moon, W.K. Comparative evaluation of average glandular dose and breast cancer detection between single-view digital breast tomosynthesis (DBT) plus single-view digital mammography (DM) and two-view DM: Correlation with breast thickness and density. Eur. Radiol. 2015, 25, 1–8. [Google Scholar] [CrossRef]
- Vedantham, S.; Karellas, A.; Vijayaraghavan, G.R.; Kopans, D.B. Digital breast tomosynthesis: State of the art. Radiology 2015, 277, 663–684. [Google Scholar] [CrossRef] [Green Version]
- Andersson, I.; Ikeda, D.M.; Zackrisson, S.; Ruschin, M.; Svahn, T.; Timberg, P.; Tingberg, A. Breast tomosynthesis and digital mammography: A comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur. Radiol. 2008, 18, 2817–2825. [Google Scholar] [CrossRef] [PubMed]
- Spangler, M.L.; Zuley, M.L.; Sumkin, J.H.; Abrams, G.; Ganott, M.A.; Hakim, C.; Perrin, R.; Chough, D.M.; Shah, R.; Gur, D. Detection and classification of calcifications on digital breast tomosynthesis and 2D digital mammography: A comparison. Am. J. Roentgenol. 2011, 196, 320–324. [Google Scholar] [CrossRef]
- Kopans, D.; Gavenonis, S.; Halpern, E.; Moore, R. Calcifications in the breast and digital breast tomosynthesis. Breast J. 2011, 17, 638–644. [Google Scholar] [CrossRef]
- Destounis, S.V.; Arieno, A.L.; Morgan, R.C. Preliminary clinical experience with digital breast tomosynthesis in the visualization of breast microcalcifications. J. Clin. Imaging Sci. 2013, 3, 65. [Google Scholar] [CrossRef] [PubMed]
- He, N.; Wu, Y.P.; Kong, Y.; Lv, N.; Huang, Z.M.; Li, S.; Wang, Y.; Geng, Z.J.; Wu, P.H.; Wie, W.D. The utility of breast cone-beam computed tomography, ultrasound, and digital mammography for detecting malignant breast tumors: A prospective study with 212 patients. Eur. J. Radiol. 2016, 85, 392–403. [Google Scholar] [CrossRef]
- Lindfors, K.K.; Boone, J.M.; Nelson, T.R.; Yang, K.; Kwan, A.L.; Miller, D.F. Dedicated breast CT: Initial clinical experience. Radiology 2008, 246, 725–733. [Google Scholar] [CrossRef]
- Shah, J.P.; Mann, S.D.; McKinley, R.L.; Tornai, M.P. Implementation and CT sampling characterization of a third-generation SPECT-CT system for dedicated breast imaging. J. Med. Imaging 2017, 4, 033502. [Google Scholar] [CrossRef]
- Wienbeck, S.; Lotz, J.; Fischer, U. Review of clinical studies and first clinical experiences with a commercially available cone-beam breast CT in Europe. Clin. Imaging 2017, 42, 50–59. [Google Scholar] [CrossRef]
- Cho, H.M.; Ding, H.; Barber, W.C.; Iwanczyk, J.S.; Molloi, S. Microcalcification detectability using a bench-top prototype photon-counting breast CT based on a Si strip detector. Med. Phys. 2015, 42, 4401–4410. [Google Scholar] [CrossRef] [Green Version]
- Kalender, W.A.; Beister, M.; Boone, J.M.; Kolditz, D.; Vollmar, S.V.; Weigel, M.C. High-resolution spiral CT of the breast at very low dose: Concept and feasibility considerations. Eur. Radiol. 2012, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kalender, W.A.; Kolditz, D.; Steiding, C.; Ruth, V.; Lück, F.; Rößler, A.C.; Wenkel, E. Technical feasibility proof for high-resolution low-dose photon-counting CT of the breast. Eur. Radiol. 2017, 27, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Berger, N.; Marcon, M.; Saltybaeva, N.; Kalender, W.A.; Alkadhi, H.; Frauenfelder, T.; Boss, A. Dedicated Breast Computed Tomography with a Photon-Counting Detector: Initial Results of Clinical In Vivo Imaging. Investig. Radiol. 2019, 54, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Berger, N.; Marcon, M.; Frauenfelder, T.; Boss, A. Dedicated Spiral Breast Computed Tomography with a Single Photon-Counting Detector: Initial Results of the First 300 Women. Investig. Radiol. 2020, 55, 68–72. [Google Scholar] [CrossRef]
- Germann, M.; Shim, S.; Angst, F.; Saltybaeva, N.; Boss, A. Spiral breast computed tomography (CT): Signal-to-noise and dose optimization using 3D-printed phantoms. Eur. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Holland, R.; Hendriks, J.H. Microcalcifications associated with ductal carcinoma in situ: Mammographic-pathologic correlation. Semin. Diagn. Pathol. 1994, 11, 181–192. [Google Scholar]
- Newcombe, R.G. Two-Sided Confidence Intervals for the Single Proportion: Comparison of Seven Methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Rößler, A.C.; Kalender, W.; Kolditz, D.; Steiding, C.; Ruth, V.; Preuss, C.; Peter, S.C.; Brehm, B.; Hammon, M.; Schulz-Wendtland, R.; et al. Performance of Photon-Counting Breast Computed Tomography, Digital Mammography, and Digital Breast Tomosynthesis in Evaluating Breast Specimens. Acad. Radiol. 2017, 24, 184–190. [Google Scholar] [CrossRef]
- Shim, S.; Saltybaeva, N.; Berger, N.; Marcon, M.; Alkadhi, H.; Boss, A. Lesion Detectability and Radiation Dose in Spiral Breast CT With Photon-Counting Detector Technology: A Phantom Study. Investig. Radiol. 2020, 55, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.; Mariscotti, G.; Durando, M.; Stevanin, C.; Tagliafico, G.; Martino, L.; Bignotti, B.; Calabrese, M.; Houssami, N. Characterisation of microcalcification clusters on 2D digital mammography (FFDM) and digital breast tomosynthesis (DBT): Does DBT underestimate microcalcification clusters? Results of a multicentre study. Eur. Radiol. 2015, 25, 9–14. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, A.; Conover, D.L.; Zhang, Y.; Seifert, P.; Logan-Young, W.; Lin, C.F.; Sahler, L.; Ning, R. Cone-beam CT for breast imaging: Radiation dose, breast coverage, and image quality. Am. J. Roentgenol. 2010, 195, 496–509. [Google Scholar] [CrossRef]
- Boone, J.M.; Nelson, T.R.; Lindfors, K.K.; Seibert, J.A. Dedicated breast CT: Radiation dose and image quality evaluation. Radiology 2001, 221, 657–667. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DBT | SBCT | p–Value (McNemar–Test) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Recon1 | Recon2 | Recon3 | DBT vs. Recon1 | DBT vs. Recon2 | DBT vs. Recon3 | Recon1 vs. Recon2 | Recon1 vs. Recon3 | Recon2 vs. Recon3 | ||
| reader1 | ||||||||||
| Sensitivity (95% CI) | 94.3% (89.1–97.2) | 88.5% (82.2–92.9) | 94.9% (89.9–97.6) | 92.4% (86.7–95.8) | 0.049 | 1.0 | 0.508 | 0.006 | 0.210 | 0.125 |
| Specificity (95% CI) | 84.7% (72.5–92.4) | 94.9% (84.9–98.7) | 91.5% (80.6–96.8) | 93.2% (82.7–97.8) | 0.070 | 0.388 | 0.227 | 0.688 | 1.0 | 1.0 |
| reader2 | ||||||||||
| Sensitivity (95% CI) | 93.0% (87.5–96.3) | 86.0% (79.3–90.8) | 92.4% (86.7–95.8) | 93.0% (87.5–96.3) | 0.027 | 1.0 | 1.0 | 0.041 | 0.027 | 1.0 |
| Specificity (95% CI) | 91.5% (80.6–96.8) | 94.9% (84.9–98.7) | 93.2% (82.7–97.8) | 91.5% (80.6–96.8) | 0.688 | 1.0 | 1.0 | 1.0 | 0.688 | 1.0 |
| DBT | SBCT | p-Value (McNemar Test) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Recon1 | Recon2 | Recon3 | DBT vs. Recon1 | DBT vs. Recon2 | DBT vs. Recon3 | Recon1 vs. Recon2 | Recon1 vs. Recon3 | Recon2 vs. Recon3 | ||
| Cluster | ||||||||||
| reader1 | 79.7% | 54.4% | 62.0% | 59.5% | <0.001 | 0.001 | <0.001 | 0.210 | 0.454 | 0.500 |
| reader2 | 77.2% | 62.0% | 75.9% | 75.9% | 0.017 | 1 | 1 | 0.013 | 0.019 | 1 |
| Diffuse Microcalcifications | ||||||||||
| reader1 | 88.9% | 81.0% | 92.1% | 88.9% | 0.052 | 0.289 | 1 | 0.001 | 0.021 | 0.125 |
| reader2 | 88.1% | 80.2% | 85.7% | 84.1% | 0.078 | 0.607 | 0.332 | 0.170 | 0.424 | 0.250 |
| Diffuse Microcalcifications (maximum diameter ≤ 0.5 mm) | ||||||||||
| reader1 | 86.3% | 76.5% | 90.2% | 86.3% | 0.052 | 0.289 | 1 | 0.001 | 0.021 | 0.125 |
| reader2 | 85.3% | 78.4% | 82.4% | 80.4% | 0.210 | 0.607 | 0.332 | 0.541 | 0.832 | 0.625 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wetzl, M.; Wenkel, E.; Balbach, E.; Dethlefsen, E.; Hartmann, A.; Emons, J.; Kuhl, C.; Beckmann, M.W.; Uder, M.; Ohlmeyer, S. Detection of Microcalcifications in Spiral Breast Computed Tomography with Photon-Counting Detector Is Feasible: A Specimen Study. Diagnostics 2021, 11, 848. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050848
Wetzl M, Wenkel E, Balbach E, Dethlefsen E, Hartmann A, Emons J, Kuhl C, Beckmann MW, Uder M, Ohlmeyer S. Detection of Microcalcifications in Spiral Breast Computed Tomography with Photon-Counting Detector Is Feasible: A Specimen Study. Diagnostics. 2021; 11(5):848. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050848
Chicago/Turabian StyleWetzl, Matthias, Evelyn Wenkel, Eva Balbach, Ebba Dethlefsen, Arndt Hartmann, Julius Emons, Christiane Kuhl, Matthias W. Beckmann, Michael Uder, and Sabine Ohlmeyer. 2021. "Detection of Microcalcifications in Spiral Breast Computed Tomography with Photon-Counting Detector Is Feasible: A Specimen Study" Diagnostics 11, no. 5: 848. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050848