
Short-Term CPAP Improves Biventricular Function in Patients with Moderate-Severe OSA and Cardiometabolic Comorbidities

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sleep Study
2.2. Echocardiography
2.3. Doppler Analysis
2.4. Global LV Longitudinal Strain Imaging
2.5. Ambulatory Blood Pressure Monitoring (ABPM)
2.6. CPAP Therapy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.-L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers 2015, 1, 15015. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.A.; Veasey, S.C.; Morgan, B.J.; O’Donnell, C.P. Pathophysiology of sleep apnea. Physiol. Rev. 2010, 90, 47–112. [Google Scholar] [CrossRef] [PubMed]
- Lavie, L. Obstructive sleep apnoea syndrome—An oxidative stress disorder. Sleep Med. Rev. 2003, 7, 35–51. [Google Scholar] [CrossRef]
- Smith, R.P.; Veale, D.; Pépin, J.L.; Lévy, P.A. Obstructive sleep apnoea and the autonomic nervous system. Sleep Med. Rev. 1998, 2, 69–92. [Google Scholar] [CrossRef]
- Pépin, J.-L.; Tamisier, R.; Barone-Rochette, G.; Launois, S.H.; Lévy, P.; Baguet, J.-P. Comparison of continuous positive airway pressure and valsartan in hypertensive patients with sleep apnea. Am. J. Respir. Crit. Care Med. 2010, 182, 954–960. [Google Scholar] [CrossRef]
- Brooks, D.; Horner, R.L.; Kozar, L.F.; Render-Teixeira, C.L.; Phillipson, E.A. Obstructive sleep apnea as a cause of systemic hypertension. evidence from a canine model. J. Clin. Investig. 1997, 99, 106–109. [Google Scholar] [CrossRef]
- Parker, J.D.; Brooks, D.; Kozar, L.F.; Render-Teixeira, C.L.; Horner, R.L.; Douglas Bradley, T.; Phillipson, E.A. Acute and chronic effects of airway obstruction on canine left ventricular performance. Am. J. Respir. Crit. Care Med. 1999, 160, 1888–1896. [Google Scholar] [CrossRef]
- Sascău, R.; Zota, I.M.; Stătescu, C.; Boișteanu, D.; Roca, M.; Maștaleru, A.; Leon Constantin, M.M.; Vasilcu, T.F.; Gavril, R.S.; Mitu, F. Review of echocardiographic findings in patients with obstructive sleep apnea. Can. Respir. J. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, S.; Dahlslett, T.; Grenne, B.; Sjøli, B.; Smiseth, O.; Edvardsen, T.; Brunvand, H. Global longitudinal strain is a more reproducible measure of left ventricular function than ejection fraction regardless of echocardiographic training. Cardiovasc. Ultrasound 2019, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Altekin, R.E.; Yanıkoğlu, A.; Karakaş, M.S.; Ozel, D.; Yıldırım, A.B.; Kabukçu, M. Evaluation of Subclinical left ventricular systolic dysfunction in patients with obstructive sleep apnea by automated function imaging method; an observational study. Anadolu Kardiyol. Derg. AKD Anatol. J. Cardiol. 2012, 12, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Varghese, M.J.; Sharma, G.; Shukla, G.; Seth, S.; Mishra, S.; Gupta, A.; Bahl, V.K. Longitudinal ventricular systolic dysfunction in patients with very severe obstructive sleep apnea: A case control study using speckle tracking imaging. Indian Heart J. 2017, 69, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Vural, M.G.; Çetin, S.; Keser, N.; Firat, H.; Akdemir, R.; Gunduz, H. Left ventricular torsion in patients with obstructive sleep apnoea before and after continuous positive airway pressure therapy: Assessment by two-dimensional speckle tracking echocardiography. Acta. Cardiol. 2017, 72, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Kourouklis, S.P.; Vagiakis, E.; Paraskevaidis, I.A.; Farmakis, D.; Kostikas, K.; Parissis, J.T.; Katsivas, A.; Kremastinos, D.T.; Anastasiou-Nana, M.; Filippatos, G. Effective Sleep apnoea treatment improves cardiac function in patients with chronic heart failure. Int. J. Cardiol. 2013, 168, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Akar Bayram, N.; Ciftci, B.; Durmaz, T.; Keles, T.; Yeter, E.; Akcay, M.; Bozkurt, E. Effects of continuous positive airway pressure therapy on left ventricular function assessed by tissue doppler imaging in patients with obstructive sleep apnoea syndrome. Eur. J. Echocardiogr. 2009, 10, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Colish, J.; Walker, J.R.; Elmayergi, N.; Almutairi, S.; Alharbi, F.; Lytwyn, M.; Francis, A.; Bohonis, S.; Zeglinski, M.; Kirkpatrick, I.D.C.; et al. Obstructive sleep apnea. Chest 2012, 141, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Au, S.; Lau, C.; Chen, K.; Cheong, A.; Tong, Y.; Chan, L. Hemodynamic Effects of noninvasive positive-pressure ventilation assessed using transthoracic echocardiography. J. Cardiovasc. Echogr. 2018, 28, 114. [Google Scholar] [CrossRef]
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of adult obstructive sleep apnea with positive airway pressure: An american academy of sleep medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2019, 15, 301–334. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Shim, C.Y.; Cho, Y.-J.; Park, S.; Lee, C.J.; Park, J.H.; Cho, H.J.; Ha, J.-W.; Hong, G.-R. Continuous Positive airway pressure therapy restores cardiac mechanical function in patients with severe obstructive sleep apnea: A randomized, sham-controlled study. J. Am. Soc. Echocardiogr. 2019, 32, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. The EACVI Textbook of Echocardiography; Oxford University Press: Oxford, UK, 2017; ISBN 978-0-19-103889-1. [Google Scholar]
- Engleman, H.M.; Wild, M.R. Improving CPAP Use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med. Rev. 2003, 7, 81–99. [Google Scholar] [CrossRef]
- Haruki, N.; Takeuchi, M.; Kanazawa, Y.; Tsubota, N.; Shintome, R.; Nakai, H.; Lang, R.M.; Otsuji, Y. Continuous Positive airway pressure ameliorates sleep-induced subclinical left ventricular systolic dysfunction: Demonstration by two-dimensional speckle-tracking echocardiography. Eur. J. Echocardiogr. 2010, 11, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Wachter, R.; Lüthje, L.; Klemmstein, D.; Lüers, C.; Stahrenberg, R.; Edelmann, F.; Holzendorf, V.; Hasenfuß, G.; Andreas, S.; Pieske, B. Impact of obstructive sleep apnoea on diastolic function. Eur. Respir. J. 2013, 41, 376–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dursunoglu, D.; Dursunoglu, N.; Evrengül, H.; Ozkurt, S.; Kuru, O.; Kiliç, M.; Fisekci, F. Impact of obstructive sleep apnoea on left ventricular mass and global Function. Eur. Respir. J. 2005, 26, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Altekin, R.E.; Karakas, M.S.; Yanikoglu, A.; Ozel, D.; Ozbudak, O.; Demir, I.; Deger, N. Determination of right ventricular dysfunction using the speckle tracking echocardiography method in patients with obstructive sleep apnea. Cardiol. J. 2012, 19, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Vitarelli, A.; D’Orazio, S.; Caranci, F.; Capotosto, L.; Rucos, R.; Iannucci, G.; Continanza, G.; Dettori, O.; De Cicco, V.; Vitarelli, M.; et al. Left ventricular torsion abnormalities in patients with obstructive sleep apnea syndrome: An early sign of subclinical dysfunction. Int. J. Cardiol. 2013, 165, 512–518. [Google Scholar] [CrossRef]
- Oliveira, W.; Poyares, D.; Cintra, F.; Vieira, M.L.C.; Fischer, C.H.; Moises, V.; Tufik, S.; Carvalho, A.; Campos, O. Impact of Continuous positive airway pressure treatment on right ventricle performance in patients with obstructive sleep apnoea, assessed by three-dimensional echocardiography. Sleep Med. 2012, 13, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Akbar, M.; Woods, T.; Szabo, A.; Franco, R. Impact of CPAP for OSA on right heart function as measured by TAPSE and RV contraction velocity by color doppler ECHO. Chest 2011, 140, 822A. [Google Scholar] [CrossRef] [Green Version]
- Holtstrand Hjälm, H.; Fu, M.; Hansson, P.-O.; Zhong, Y.; Caidahl, K.; Mandalenakis, Z.; Morales, D.; Ergatoudes, C.; Rosengren, A.; Grote, L.; et al. Association between left atrial Enlargement and obstructive sleep apnea in a general population of 71-year-old men. J. Sleep Res. 2018, 27, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Wright, L.; Negishi, T.; Negishi, K.; Liu, J.; Marwick, T.H. Research to practice. JACC Cardiovasc. Imaging 2018, 11, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.-W.; Shu, X.-H.; Liu, Y.-L.; Shen, H.; Li, W.-J.; Gong, X.; Chen, H.-Y.; Zhao, W.-P.; Pan, C.-Z.; Li, S.-Q. A novel method for sensitive determination of subclinical left-ventricular systolic dysfunction in subjects with obstructive sleep apnea. Respir. Care 2016, 61, 366–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Azevedo, J.C.M.; de Carvalho, E.R.M.; Feijó, L.A.; de Oliveira, F.P.; de Menezes, S.L.S.; Murad, H. Efeitos Da Pressão Positiva Contínua Nas Vias Aéreas Na Insuficiência Cardíaca Crônica. Arq. Bras. Cardiol. 2010, 95, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakhama, L.; Herbegue, B.; Abouda, M.; Antit, S.; Slama, I.; Boussabah, E.; Thameur, M.; Masmoudi, M.; Abdelaali, N.; Charfi, M.R.; et al. Impact of obstructive sleep apnea on the right ventricle. Tunis. Med. 2016, 94, 612–615. [Google Scholar] [PubMed]
- Dursunoglu, N.; Dursunoglu, D.; Özkurt, S.; Gür, S.; Özalp, G.; Evyapan, F. Effects of CPAP on right ventricular myocardial performance index in obstructive sleep apnea patients without hypertension. Respir. Res. 2006, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Liu, P.P.; Fitzgerald, F.S.; Allidina, Y.K.; Douglas Bradley, T. Effects of continuous positive airway pressure on cardiac volumes in patients with ischemic and dilated cardiomyopathy. Am. J. Respir. Crit. Care Med. 2000, 161, 128–134. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Baseline Value |
|---|---|
| Age (years) | 57.98 ± 9.17 |
| Sex (m/f) | 40/17 |
| Weight (kg) | 101.21 ± 17.63 |
| BMI (kg/m2) | 34.37 ± 5.99 |
| Waist circumference (cm) | 114.79 ± 11.43 |
| Systolic Blood Pressure (mmHg) | 137.21 ± 18.38 |
| Diastolic Blood Pressure (mmHg) | 86.47 ± 11.87 |
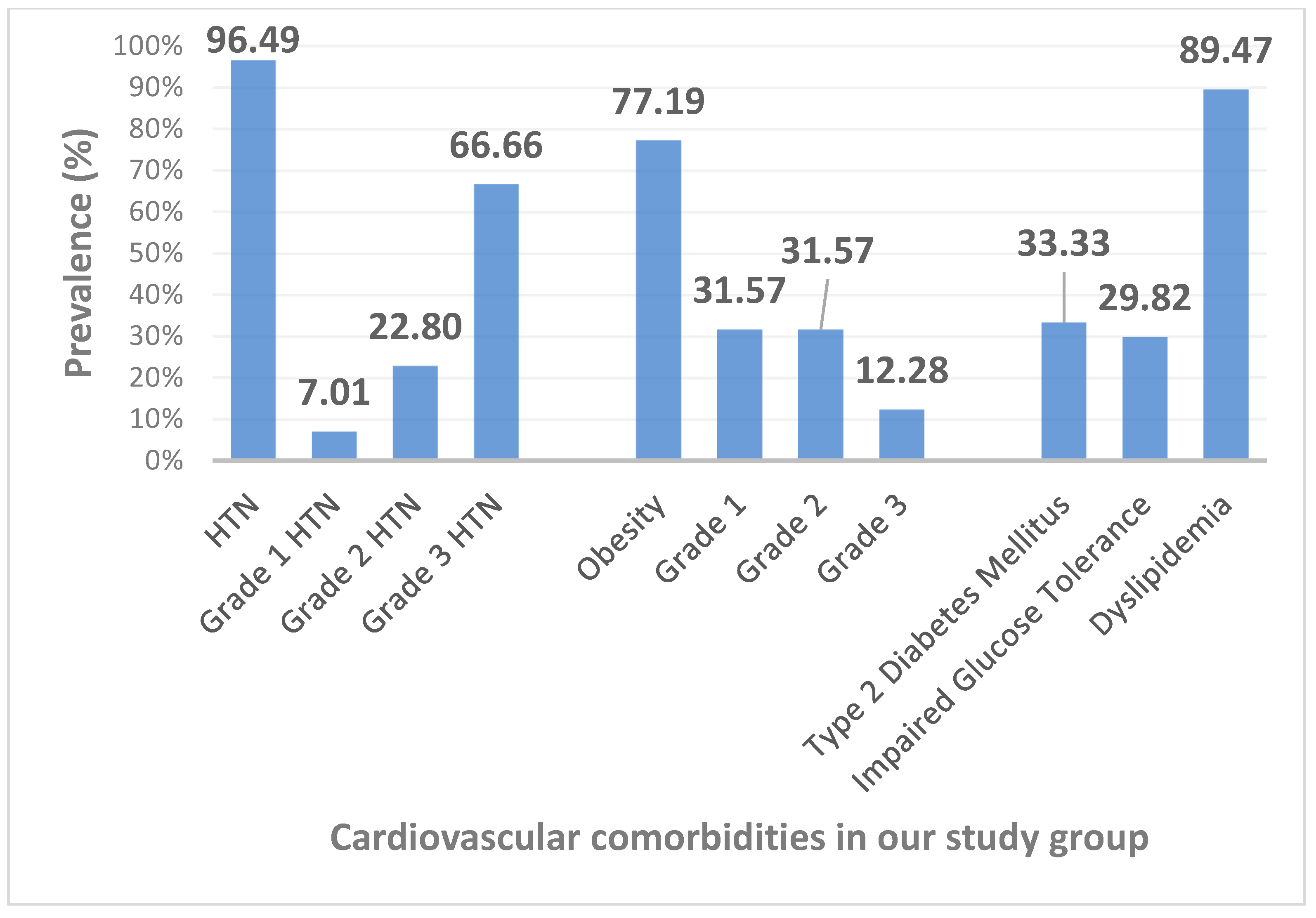
| Systemic Hypertension (n) | 55 |
| Grade 1 (n) | 4 |
| Grade 2 (n) | 13 |
| Grade 3 (n) | 38 |
| Obesity (n) | 44 |
| Grade 1 (n) | 18 |
| Grade 2 (n) | 18 |
| Grade 3 (n) | 7 |
| Diabetes Mellitus (n) | 19 |
| Impaired glucose tolerance (n) | 17 |
| Dyslipidemia (n) | 51 |
| AHI (events/h) | 42.3 ± 21.3 |
| Desaturation index (events/h) | 40.34 ± 20.86 |
| Minimum nocturnal O2Sa (%) | 71.58 ± 11.61 |
| Average nocturnal O2Sa (%) | 91.05 ± 3.72 |
| CPAP pressure (cmH20) | 11.31 ± 2.45 |
| Variable | Baseline Value All Patients (n = 57) | Moderate OSA Subgroup (n = 22) | Severe OSA Subgroup (n = 35) | p * |
|---|---|---|---|---|
| Septal wall thickness (mm) | 11.64 ± 1.76 | 11.51 ± 1.97 | 11.72 ± 1.64 | NS |
| LV posterior wall thickness (mm) | 11.86 ± 1.54 | 11.86 ±1.41 | 11.86 ± 1.64 | NS |
| LV end-diastolic diameter (mm) | 54.45 ± 7.31 | 54.01 ± 6.55 | 54.73 ± 7.83 | NS |
| LV EF (%) | 56.69 ± 6.81 | 57.74 ± 5.80 | 56.03 ± 7.37 | NS |
| MAPSE (mm) | 15.8 ± 3.50 | 15.47 ± 2.88 | 16 ± 3.87 | NS |
| RV diameter (mm) | 34 ± 3.97 | 33.58 ± 4.11 | 34.26 ± 3.92 | NS |
| RV wall thickness (mm) | 5.59 ± 1.25 | 5.44 ± 1.34 | 5.66 ± 1.19 | NS |
| TAPSE (mm) | 26.23 ± 5.60 | 26.18 ± 6.02 | 26.27 ± 5.42 | NS |
| LA volume (ml) | 75.22 ± 23.19 | 84.86 ± 29.79 | 69.28 ± 15.60 | 0.01 |
| RA volume (ml) | 56.23 ± 16.41 | 59.45 ± 18.74 | 54.77 ± 14.87 | NS |
| Transmitral E wave (cm/s) | 73.32 ± 20.50 | 71.26 ± 20.92 | 74.62 ± 20.43 | NS |
| Transmitral A wave (cm/s) | 74.88 ± 22.98 | 69.07 ± 26.10 | 78.68 ± 19.66 | NS |
| Transmitral E/A ratio | 1.04 ± 0.47 | 1.16 ± 0.61 | 0.97 ± 0.32 | NS |
| Deceleration time (ms) | 204.81 ± 64.09 | 220.90 ± 76.52 | 200 ± 69.23 | NS |
| Isovolumetric relaxation time (ms) | 117.54 ± 21.15 | 115.27 ± 25.19 | 115.42 ± 21.30 | NS |
| Medial mitral e’ (cm/s) | 7.87 ± 2.15 | 7.97 ± 1.73 | 7.77 ± 2.38 | NS |
| Lateral mitral e’ (cm/s) | 10.96 ± 3.33 | 10.71 ± 3.06 | 10.97 ± 3.60 | NS |
| Medial mitral S’ (cm/s) | 8.60 ± 1.71 | 8.17 ± 1.75 | 8.73 ± 1.76 | NS |
| Lateral mitral S’ (cm/s) | 9.29 ± 2.17 | 9.41 ± 2.43 | 9.09 ± 2.14 | NS |
| E/average e’ | 7.97 ± 2.42 | 7.92 ± 3.26 | 8.33 ± 2.60 | NS |
| RV S’ (cm/s) | 13.47 ± 3.11 | 13.28 ± 3.59 | 13.96 ± 3.26 | NS |
| PASP (mmHg) | 21.97 ± 12.29 | 23.38 ± 13.32 | 21.12 ± 11.76 | NS |
| LV-GLS (%) | −16.07 ± 3.81 | −16.92 ± 3.70 | −15.54 ± 3.93 | NS |
| All Patients (n = 57) | CPAP Use < 240 Min/Night (n = 24) | CPAP Use ≥ 240 Min/Night (n = 24) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Baseline | After 8 Weeks CPAP | p * | Baseline | After 8 Weeks CPAP | p ” | Baseline | After 8 Weeks CPAP | p # |
| Weight (kg) | 101.21 | 99.07 | 0.000002 | 109.16 | 106.31 | 0.0003 | 95.77 | 94.14 | 0.01 |
| BMI (kg/m2) | 34.36 | 33.83 | 0.01 | 36.56 | 35.88 | NS | 33.37 | 32.80 | 0.04 |
| Waist circumference (cm) | 114.78 | 111.97 | 0.000001 | 119.79 | 115.77 | 0.00006 | 111.62 | 109.20 | 0.002 |
| SBP/24 h | 130.45 | 130.89 | NS | 129.25 | 130.20 | NS | 130.00 | 130.70 | NS |
| DBP/24 h | 75.66 | 74.87 | NS | 76.62 | 75.04 | NS | 74.16 | 74.29 | NS |
| Septal wall thickness (mm) | 11.64 | 11.41 | NS | 11.52 | 11.4 | NS | 11.75 | 11.33 | NS |
| LV posterior wall thickness (mm) | 11.86 | 11.65 | NS | 11.57 | 11.49 | NS | 11.87 | 11.53 | NS |
| LV end-diastolic diameter (mm) | 54.45 | 53.27 | NS | 54.06 | 52.17 | NS | 54.97 | 53.75 | NS |
| LV EF (%) | 56.69 | 56.49 | NS | 53.78 | 53.97 | NS | 59.42 | 58.37 | NS |
| MAPSE (mm) | 15.8 | 16.7 | NS | 15.6 | 15.85 | NS | 15.98 | 17.06 | NS |
| RV diameter (mm) | 33.83 | 32.97 | 0.01 | 34.39 | 33.31 | NS | 32.34 | 31.35 | 0.04 |
| RV wall thickness (mm) | 5.59 | 5.20 | 0.008 | 5.63 | 5.32 | NS | 5.46 | 4.96 | 0.02 |
| TAPSE (mm) | 26.23 | 27.92 | 0.03 | 26.68 | 27.67 | NS | 25.81 | 29.04 | 0.007 |
| LA volume (mL) | 75.22 | 76.43 | NS | 72.45 | 72.69 | NS | 76.47 | 79.36 | NS |
| RA volume (mL) | 56.23 | 56.95 | NS | 54.39 | 54.57 | NS | 56.77 | 57.91 | NS |
| Transmitral E wave (cm/s) | 73.32 | 81.69 | 0.0002 | 69.32 | 79.49 | 0.007 | 74.01 | 83.33 | 0.01 |
| Transmitral A wave (cm/s) | 74.88 | 74.84 | NS | 70.86 | 69.69 | NS | 77.6 | 81.44 | NS |
| Transmitral E/A ratio | 1.04 | 1.15 | 0.02 | 1.02 | 1.16 | 0.01 | 1.02 | 1.10 | NS |
| Deceleration time (ms) | 204.81 | 216.65 | NS | 203.16 | 215 | NS | 196.22 | 216.04 | NS |
| Isovolumetric relaxation time (ms) | 117.54 | 109.69 | 0.01 | 114.41 | 110.83 | NS | 118.22 | 108 | 0.02 |
| Medial mitral e’ (cm/s) | 7.87 | 7.95 | NS | 8.17 | 7.47 | NS | 7.82 | 8.05 | NS |
| Lateral mitral e’ (cm/s) | 10.96 | 11.16 | NS | 12 | 11.70 | NS | 10.09 | 10.56 | NS |
| Medial mitral S’ (cm/s) | 8.60 | 8.52 | NS | 9.50 | 9.61 | NS | 8.28 | 8.34 | NS |
| Lateral mitral S’ (cm/s) | 9.29 | 9.46 | NS | 8.45 | 8.45 | NS | 8.67 | 9.24 | NS |
| E/average e’ | 7.97 | 8.71 | NS | 7.32 | 8.47 | NS | 8.11 | 9.06 | NS |
| RV S’ (cm/s) | 13.47 | 14.34 | 0.01 | 13.35 | 14.66 | 0.01 | 13.32 | 14.29 | 0.02 |
| PASP (mmHg) | 21.97 | 21.14 | NS | 20.22 | 17.20 | NS | 24.34 | 26.22 | NS |
| LV-GLS (%) | −16.07 | −18.64 | 0.001 | −15.6 | −18.56 | NS | −15.15 | −18.1 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zota, I.M.; Sascău, R.A.; Stătescu, C.; Tinică, G.; Leon Constantin, M.M.; Roca, M.; Boișteanu, D.; Anghel, L.; Mitu, O.; Mitu, F. Short-Term CPAP Improves Biventricular Function in Patients with Moderate-Severe OSA and Cardiometabolic Comorbidities. Diagnostics 2021, 11, 889. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050889
Zota IM, Sascău RA, Stătescu C, Tinică G, Leon Constantin MM, Roca M, Boișteanu D, Anghel L, Mitu O, Mitu F. Short-Term CPAP Improves Biventricular Function in Patients with Moderate-Severe OSA and Cardiometabolic Comorbidities. Diagnostics. 2021; 11(5):889. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050889
Chicago/Turabian StyleZota, Ioana Mădălina, Radu Andy Sascău, Cristian Stătescu, Grigore Tinică, Maria Magdalena Leon Constantin, Mihai Roca, Daniela Boișteanu, Larisa Anghel, Ovidiu Mitu, and Florin Mitu. 2021. "Short-Term CPAP Improves Biventricular Function in Patients with Moderate-Severe OSA and Cardiometabolic Comorbidities" Diagnostics 11, no. 5: 889. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050889