
Evaluation of Complete Pathological Regression after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients with BRCA1 Founder Mutation Aided Bayesian A/B Testing Approach

 , , and
, , and
Abstract
:1. Introduction
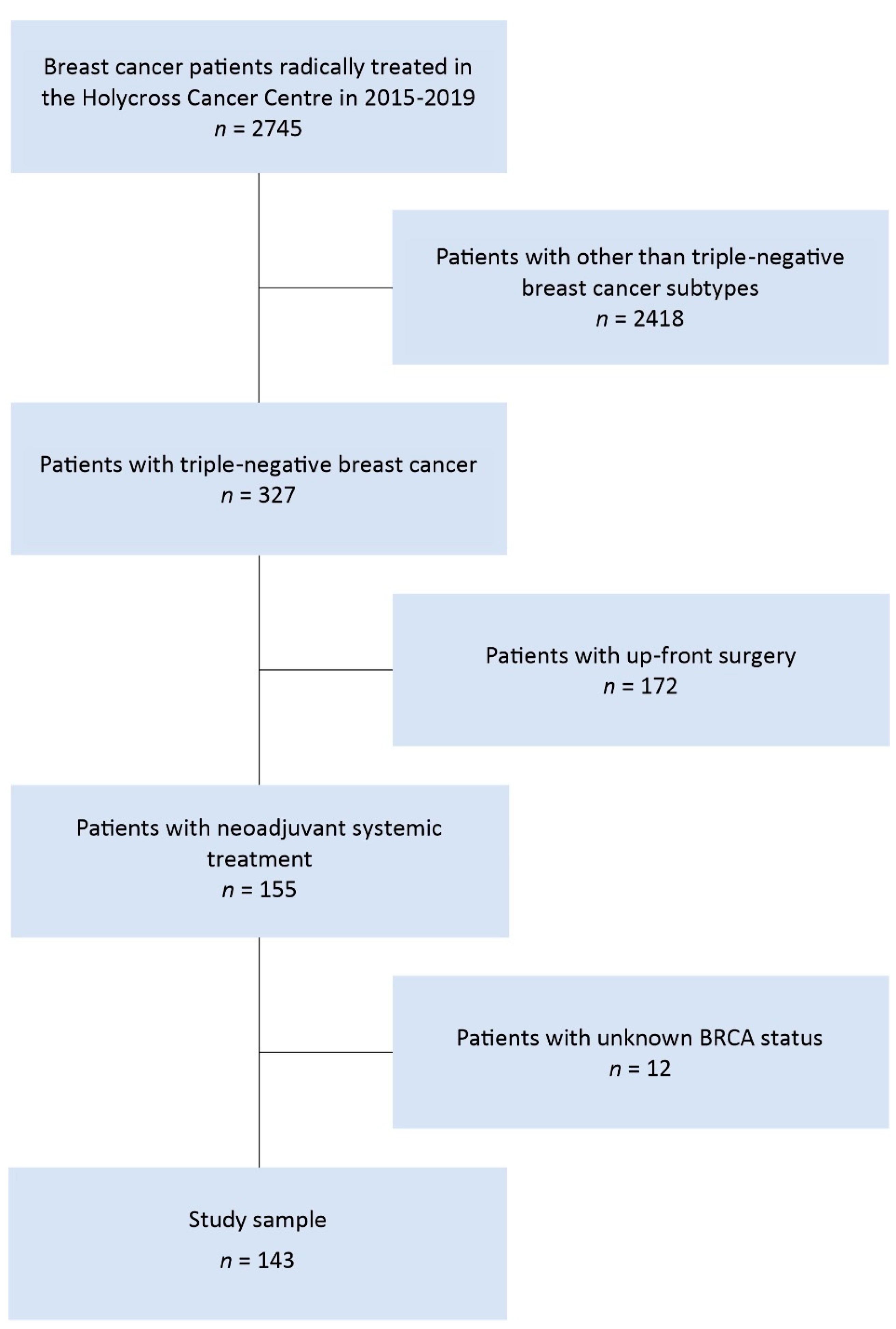
2. Materials and Methods
2.1. Verification of Data
2.2. Pathologic Complete Regression Status Determination
2.3. BRCA Status Determination
2.3.1. DNA Isolation
2.3.2. High-Resolution Melting (HRM)-Polymerase Chain Reaction (PCR) and Sanger Sequencing
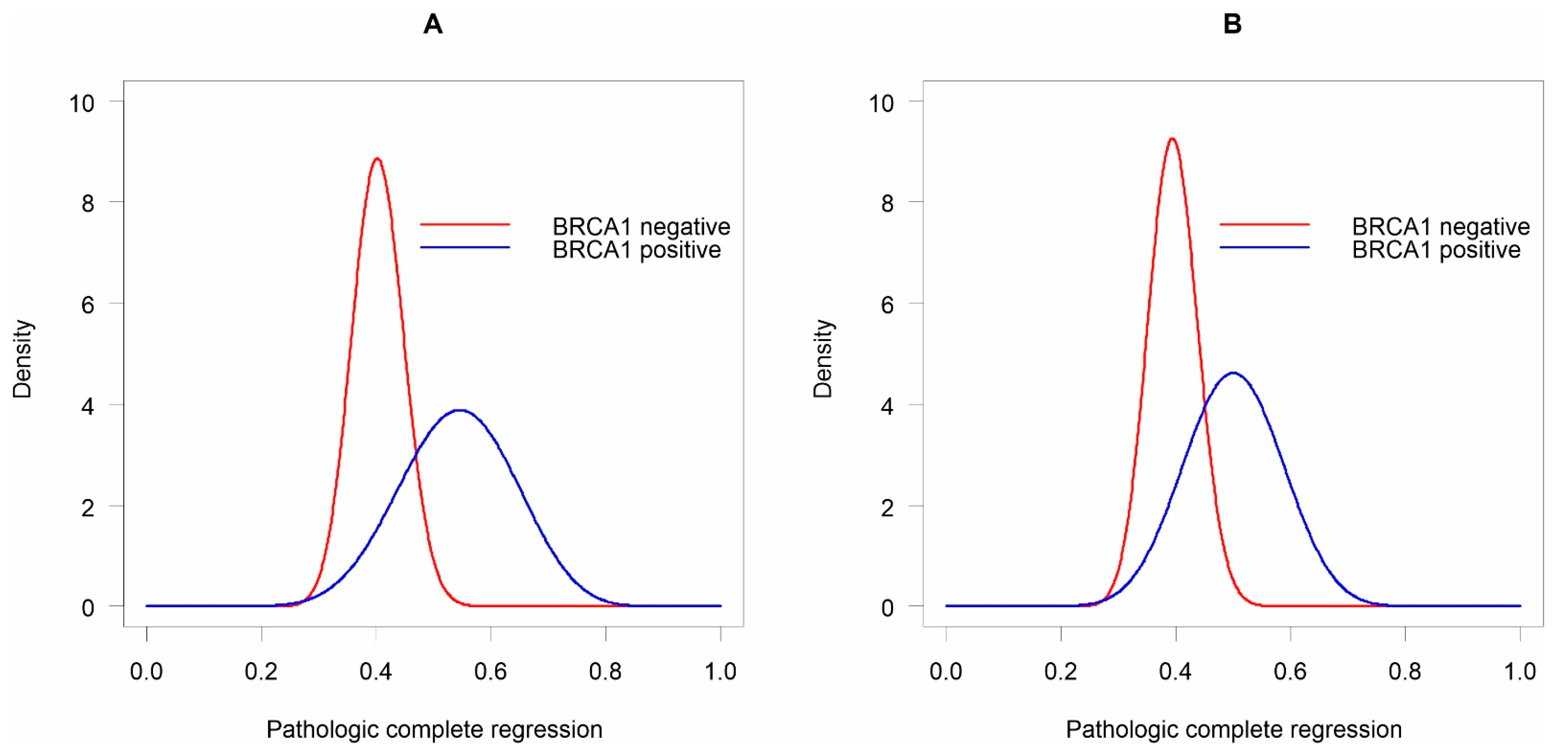
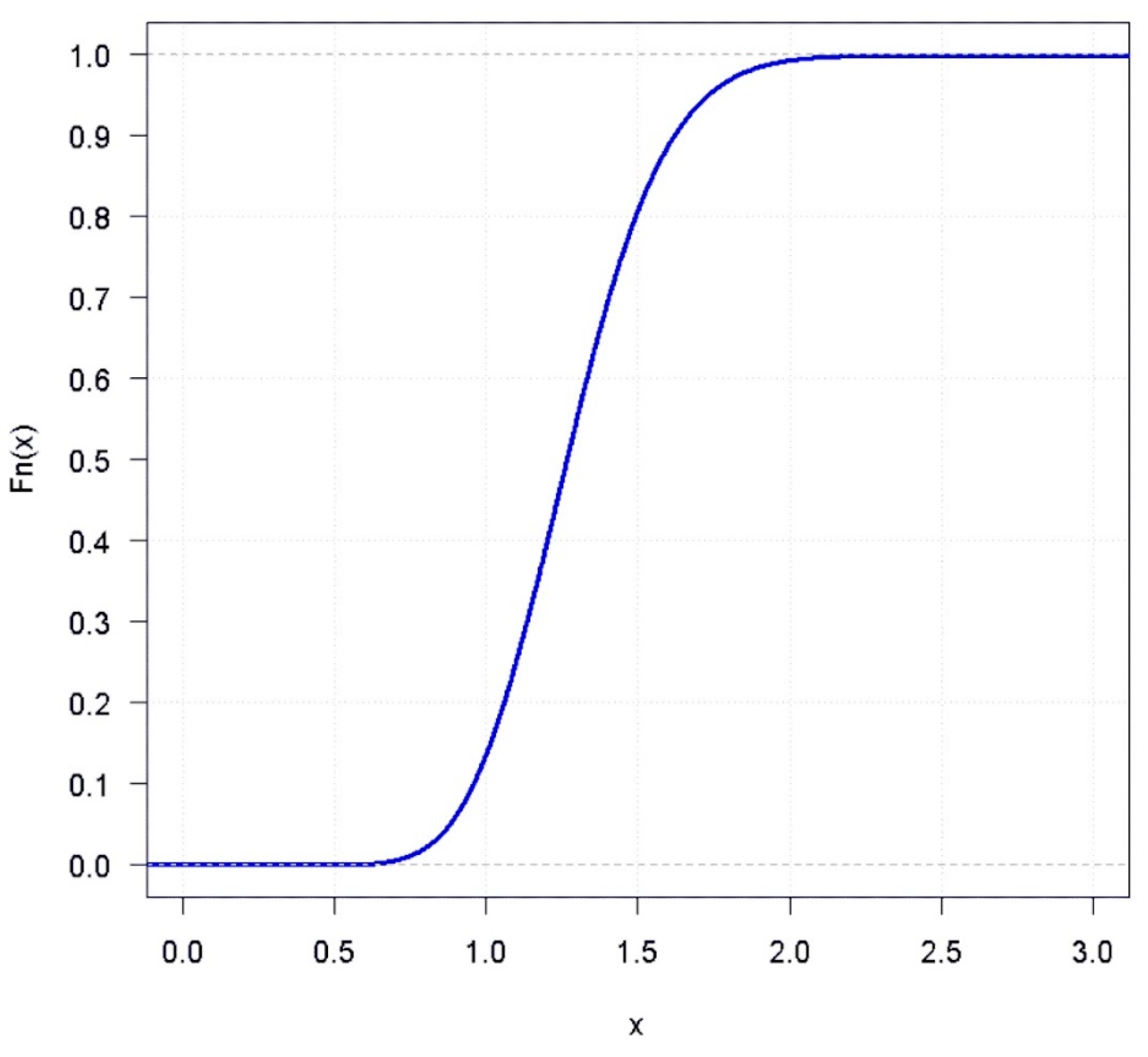
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012: Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef]
- Khosravi-Shahi, P.; Cabezón-Gutiérrez, L.; Aparicio Salcedo, M.I. State of art of advanced triple negative breast cancer. Breast J. 2019, 25, 967–970. [Google Scholar] [CrossRef]
- Chaudhary, L.N.; Hope Wilkinson, K.; Kong, A. Triple-Negative Breast Cancer: Who Should Receive Neoadjuvant Chemotherapy? Surg. Oncol. Clin. 2018, 27, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The Triple Negative Paradox: Primary Tumor Chemosensitivity of Breast Cancer Subtypes. Clin. Cancer Res. 2007, 13, 2329–2334. [Google Scholar] [CrossRef] [Green Version]
- Bear, H.D.; Anderson, S.; Smith, R.E.; Geyer, C.E.; Mamounas, E.P.; Fisher, B.; Brown, A.M.; Robidoux, A.; Margolese, R.; Kahlenberg, M.S.; et al. Sequential Preoperative or Postoperative Docetaxel Added to Preoperative Doxorubicin plus Cyclophosphamide for Operable Breast Cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 2006, 24, 2019–2027. [Google Scholar] [CrossRef]
- Rastogi, P.; Anderson, S.J.; Bear, H.D.; Geyer, C.E.; Kahlenberg, M.S.; Robidoux, A.; Margolese, R.G.; Hoehn, J.L.; Vogel, V.G.; Dakhil, S.R.; et al. Preoperative Chemotherapy: Updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J. Clin. Oncol. 2008, 26, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, W.; Verma, V.; Hatch, S.; Klimberg, V.S.; Butler, E.B.; Teh, B.S. Response rates and pathologic complete response by breast cancer molecular subtype following neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2018, 170, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Darb-Esfahani, S.; Loibl, S.; Müller, B.M.; Roller, M.; Denkert, C.; Komor, M.; Schlüns, K.; Blohmer, J.U.; Budczies, J.; Gerber, B.; et al. Identification of Biology-Based Breast Cancer Types with Distinct Predictive and Prognostic Features: Role of Steroid Hormone and HER2 Receptor Expression in Patients Treated with Neoadjuvant Anthracycline/Taxane-Based Chemotherapy. Breast Cancer Res. 2009, 11, R69. [Google Scholar] [CrossRef] [Green Version]
- Citron, M.L.; Berry, D.A.; Cirrincione, C.; Hudis, C.; Winer, E.P.; Gradishar, W.J.; Davidson, N.E.; Martino, S.; Livingston, R.; Ingle, J.N.; et al. Randomized Trial of Dose-Dense versus Conventionally Scheduled and Sequential versus Concurrent Combination Chemotherapy as Postoperative Adjuvant Treatment of Node-Positive Primary Breast Cancer: First Report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J. Clin. Oncol. 2003, 21, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Gluz, O.; Nitz, U.A.; Harbeck, N.; Ting, E.; Kates, R.; Herr, A.; Lindemann, W.; Jackisch, C.; Berdel, W.E.; Kirchner, H.; et al. Triple-Negative High-Risk Breast Cancer Derives Particular Benefit from Dose Intensification of Adjuvant Chemotherapy: Results of WSG AM-01 Trial. Ann. Oncol. 2008, 19, 861–870. [Google Scholar] [CrossRef]
- Lebert, J.M.; Lester, R.; Powell, E.; Seal, M.; McCarthy, J. Advances in the systemic treatment of triple-negative breast cancer. Curr. Oncol. 2018, 25 (Suppl. 1), S142–S150. [Google Scholar] [CrossRef] [Green Version]
- Mazouni, C.; Kau, S.-W.; Frye, D.; Andre, F.; Kuerer, H.M.; Buchholz, T.A.; Symmans, W.F.; Anderson, K.; Hess, K.R.; Gonzalez-Angulo, A.M.; et al. Inclusion of Taxanes, Particularly Weekly Paclitaxel, in Preoperative Chemotherapy Improves Pathologic Complete Response Rate in Estrogen Receptor-Positive Breast Cancers. Ann. Oncol. 2007, 18, 874–880. [Google Scholar] [CrossRef]
- Hayes, D.F.; Thor, A.D.; Dressler, L.G.; Weaver, D.; Edgerton, S.; Cowan, D.; Broadwater, G.; Goldstein, L.J.; Martino, S.; Ingle, J.N.; et al. HER2 and Response to Paclitaxel in Node-Positive Breast Cancer. N. Engl. J. Med. 2007, 357, 1496–1506. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.D.; Bauer, J.A.; Schafer, J.M.; Pendleton, C.S.; Tang, L.; Johnson, K.C.; Chen, X.; Balko, J.M.; Gómez, H.; Arteaga, C.L.; et al. PIK3CA Mutations in Androgen Receptor-Positive Triple Negative Breast Cancer Confer Sensitivity to the Combination of PI3K and Androgen Receptor Inhibitors. Breast Cancer Res. 2014, 16, 406. [Google Scholar] [CrossRef] [Green Version]
- Sikov, W.M.; Berry, D.A.; Perou, C.M.; Singh, B.; Cirrincione, C.T.; Tolaney, S.M.; Kuzma, C.S.; Pluard, T.J.; Somlo, G.; Port, E.R.; et al. Impact of the Addition of Carboplatin and/or Bevacizumab to Neoadjuvant Once-per-Week Paclitaxel Followed by Dose-Dense Doxorubicin and Cyclophosphamide on Pathologic Complete Response Rates in Stage II to III Triple-Negative Breast Cancer: CALGB 40603 (Alliance). J. Clin. Oncol. 2015, 33, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Sikov, W.; Berry, D.A.; Perou, C.M.; Singh, B.; Cirrincione, C.T.; Tolaney, S.M.; Somlo, G.; Port, E.R.; Qamar, R.; Sturtz, K.; et al. Abstract S2-05: Event-Free and Overall Survival Following Neoadjuvant Weekly Paclitaxel and Dose-Dense AC/-Carboplatin and/or Bevacizumab in Triple-Negative Breast Cancer: Outcomes from CALGB 40603 (Alliance). Cancer Res. 2016. [Google Scholar] [CrossRef]
- Bianchini, G.; Balko, J.M.; Mayer, I.A.; Sanders, M.E.; Gianni, L. Triple-negative breast cancer: Challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 2016, 13, 674–690. [Google Scholar] [CrossRef]
- Maksimenko, J.; Irmejs, A.; Nakazawa-Miklasevica, M.; Melbarde-Gorkusa, I.; Trofimovics, G.; Gardovskis, J.; Miklasevics, E. Prognostic Role of BRCA1 Mutation in Patients with Triple-Negative Breast Cancer. Oncol. Lett. 2014, 7, 278–284. [Google Scholar] [CrossRef] [Green Version]
- Clifton, K.; Gutierrez-Barrera, A.; Ma, J.; Bassett, R.; Litton, J.; Kuerer, H.; Moulder, S.; Albarracin, C.; Hortobagyi, G.; Arun, B. Adjuvant versus Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients with BRCA Mutations. Breast Cancer Res. Treat. 2018, 170, 101–109. [Google Scholar] [CrossRef]
- Hahnen, E.; Lederer, B.; Hauke, J.; Loibl, S.; Kröber, S.; Schneeweiss, A.; Denkert, C.; Fasching, P.A.; Blohmer, J.U.; Jackisch, C.; et al. Germline Mutation Status, Pathological Complete Response, and Disease-Free Survival in Triple-Negative Breast Cancer: Secondary Analysis of the GeparSixto Randomized Clinical Trial. JAMA Oncol. 2017, 3, 1378–1385. [Google Scholar] [CrossRef]
- Symmans, W.F.; Wei, C.; Gould, R.; Yu, X.; Zhang, Y.; Liu, M.; Walls, A.; Bousamra, A.; Ramineni, M.; Sinn, B.; et al. Long-Term Prognostic Risk After Neoadjuvant Chemotherapy Associated With Residual Cancer Burden and Breast Cancer Subtype. J. Clin. Oncol. 2017, 35, 1049–1060. [Google Scholar] [CrossRef] [Green Version]
- Tutt, A.; Tovey, H.; Cheang, M.C.U.; Kernaghan, S.; Kilburn, L.; Gazinska, P.; Owen, J.; Abraham, J.; Barrett, S.; Barrett-Lee, P.; et al. Carboplatin in BRCA1/2-Mutated and Triple-Negative Breast Cancer BRCAness Subgroups: The TNT Trial. Nat. Med. 2018, 24, 628–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narod, S.A.; Huzarski, T.; Gronwald, J.; Byrski, T.; Marczyk, E.; Cybulski, C.; Szwiec, M.; Wisniowski, R.; Birkenfeld, B.; Kilar, E.; et al. Predictors of survival for breast cancer patients with a BRCA1 mutation. Breast Cancer Res. Treat. 2018, 168, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Byrski, T.; Gronwald, J.; Huzarski, T.; Grzybowska, E.; Budryk, M.; Stawicka, M.; Mierzwa, T.; Szwiec, M.; Wisniowski, R.; Siolek, M.; et al. Pathologic Complete Response Rates in Young Women with BRCA1-Positive Breast Cancers after Neoadjuvant Chemotherapy. J. Clin. Oncol. 2010, 28, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Poggio, F.; Bruzzone, M.; Ceppi, M.; Pondé, N.F.; La Valle, G.; Del Mastro, L.; de Azambuja, E.; Lambertini, M. Platinum-Based Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer: A Systematic Review and Meta-Analysis. Ann. Oncol. 2018, 29, 1497–1508. [Google Scholar] [CrossRef]
- Silver, D.P.; Richardson, A.L.; Eklund, A.C.; Wang, Z.C.; Szallasi, Z.; Li, Q.; Juul, N.; Leong, C.-O.; Calogrias, D.; Buraimoh, A.; et al. Efficacy of Neoadjuvant Cisplatin in Triple-Negative Breast Cancer. J. Clin. Oncol. 2010, 28, 1145–1153. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Schneeweiss, A.; Loibl, S.; Salat, C.; Denkert, C.; Rezai, M.; Blohmer, J.U.; Jackisch, C.; Paepke, S.; Gerber, B.; et al. Neoadjuvant Carboplatin in Patients with Triple-Negative and HER2-Positive Early Breast Cancer (GeparSixto; GBG 66): A Randomised Phase 2 Trial. Lancet Oncol. 2014, 15, 747–756. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Möbus, V.; Tesch, H.; Hanusch, C.; Denkert, C.; Lübbe, K.; Huober, J.; Klare, P.; Kümmel, S.; Untch, M.; et al. Intense Dose-Dense Epirubicin, Paclitaxel, Cyclophosphamideversus Weekly Paclitaxel, Liposomal Doxorubicin (plus Carboplatin in Triple-Negative Breast Cancer) for Neoadjuvant Treatment of High-Risk Early Breast Cancer (GeparOcto-GBG 84): A Randomised Phase III Trial. Eur. J. Cancer 2019, 106, 181–192. [Google Scholar] [CrossRef] [PubMed]
- ESMO. Guidelines. Available online: https://www.esmo.org/guidelines (accessed on 7 April 2021).
- NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 8 April 2021).
- Kowalik, A.; Siołek, M.; Kopczyński, J.; Krawiec, K.; Kalisz, J.; Zięba, S.; Kozak-Klonowska, B.; Wypiórkiewicz, E.; Furmańczyk, J.; Nowak-Ozimek, E.; et al. BRCA1 Founder Mutations and beyond in the Polish Population: A Single-Institution BRCA1/2 next-Generation Sequencing Study. PLoS ONE 2018, 13, e0201086. [Google Scholar] [CrossRef] [PubMed]
- Incorvaia, L.; Fanale, D.; Bono, M.; Calò, V.; Fiorino, A.; Brando, C.; Corsini, L.R.; Cutaia, S.; Cancelliere, D.; Pivetti, A.; et al. BRCA1/2 Pathogenic Variants in Triple-Negative versus Luminal-like Breast Cancers: Genotype-Phenotype Correlation in a Cohort of 531 Patients. Ther. Adv. Med. Oncol. 2020, 12, 1–19. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Exon | Sequence-Specific Primers | Primer Sequences |
|---|---|---|
| BRCA1 e20 | F | ATATGACGTGTCTGCTCCAC |
| R | GGGAATCCAAATTACACAGC | |
| BRCA1 e5 | F | CTCTTAAGGGCAGTTGTGAG |
| R | TTCCTACTGTGGTTGCTTCC | |
| BRCA1 e2 | F | GAAGTTGTCATTTTATAAACCTTT |
| R | TGTCTTTTCCCTAGTATGT | |
| BRCA1 e11 | F | CAGGGAGTTGGTCTGAGTGAC |
| R | GCTCCCCAAAAGCATAAAC |
| Characteristic | No BRCA1 Mutation (n = 119) | BRCA1 Mutation (n = 24) | p |
|---|---|---|---|
| Age (years), mean ± SD | 57.1 ± 12.5 | 47.0 ± 12.9 | <0.001 |
| Cancer side | >0.05 | ||
| Right | 62 (52.1) | 11 (45.8) | |
| Left | 57 (47.9) | 13 (54.2) | |
| Cancer type | >0.05 | ||
| NST | 105 (88.2) | 23 (95.8) | |
| Other # | 14 (11.8) | 1 (4.2) | |
| Ki-67, mean ± SD | 64.3 ± 25.8 | 77.3 ± 17.6 | <0.001 |
| Tumour size | >0.05 | ||
| T1 | 5 (4.2) | 3 (12.5) | |
| T2 | 62 (52.1) | 16 (66.7) | |
| T3 | 35 (29.4) | 5 (20.8) | |
| T4 | 17 (14.3) | no | |
| Nodal status | >0.05 | ||
| Nodes negative (cN−) | 72 (60.5) | 18 (75.0) | |
| Nodes positive (cN+) | 47 (39.5) | 6 (25.0) | |
| Clinical stage (CS) | <0.01 | ||
| I | 44 (37.0) | 17 (70.8) | |
| II | 56 (47.1) | 7 (29.2) | |
| III | 19 (16.0) | no | |
| Grading (G) | >0.05 | ||
| G1 | 4 (3.4) | no | |
| G2 | 56 (47.1) | 7 (29.2) | |
| G3 | 59 (49.6) | 17 (70.8) | |
| LVI | <0.05 | ||
| Yes | 30 (25.2) | 1 (4.2) | |
| No | 89 (74.8) | 23 (95.8) | |
| PNI | >0.05 | ||
| Yes | 4 (3.4) | no | |
| No | 115 (96.6) | 24 (100) | |
| CHTH | >0.05 | ||
| 4AC+12T | 101 (84.9) | 21 (87.5) | |
| AC/EC+ T+ Carboplatin | 9 (7.6) | 2 (8.3) | |
| Other † | 9 (7.6) | 1 (4.2) | |
| Type of surgery | <0.001 | ||
| BCT | 40 (33.6) | 1 (4.2) | |
| Radical mastectomy | 51 (42.9) | 1 (4.2) | |
| Simple mastectomy | 7 (5.9) | 3 (12.5) | |
| Skin sparing or nipple-sparing mastectomy | 21 (17.7) | 19 (79.2) | |
| pCR (ypT0 ypN0) | >0.05 | ||
| Yes | 48 (40.3) | 13 (54.2) | |
| No | 71 (59.7) | 11 (45.8) | |
| Time 1 (days), mean ± SD | 167.3 ± 73.0 | 161.5 ± 19.0 | >0.05 |
| Time 2 (days), mean ± SD | 34.8 ± 18.0 | 33.0 ± 22.3 | >0.05 |
| Characteristic | OR (95% CI) |
|---|---|
| BRCA1 mutation status | |
| BRCA1 positive vs. BRCA1 negative | 1.75 (0.72, 4.3) |
| Age (years) | 0.97 (0.95, 1.00) |
| Cancer type | |
| NST vs. other # | 1.56 (0.52, 5.23) |
| Ki-67 | 1.01 (1.00, 1.03) |
| Tumour size | |
| T2 vs. T1 | 0.17 (0.01, 0.99) |
| T3 vs. T1 | 0.05 (0.01, 0.31) ** |
| T4 vs. T1 | 0.02 (0.01, 0.18) ** |
| Nodal status | |
| Node positive vs. node negative | 0.43 (0.21, 0.88) * |
| Staging | |
| Stage II vs. stage I | 0.32 (0.15, 0.67) ** |
| Stage III vs. stage I | 0.12 (0.03, 0.41) ** |
| Grading | |
| G2 vs. G1 | 0.85 (0.10, 7.47) |
| G3 vs. G1 | 0.65 (0.07, 5.67) |
| LVI | |
| Yes vs. No | 0.03 (0.01, 0.14) *** |
| CHTH | |
| 4AC + 12T vs. other † | 5.44 (1.73, 24.07) ** |
| Time 1 (days) | 1.00 (0.99, 1.00) |
| Time 2 (days) | 0.99 (0.97, 1.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kedzierawski, P.; Macek, P.; Ciepiela, I.; Kowalik, A.; Gozdz, S. Evaluation of Complete Pathological Regression after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients with BRCA1 Founder Mutation Aided Bayesian A/B Testing Approach. Diagnostics 2021, 11, 1144. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071144
Kedzierawski P, Macek P, Ciepiela I, Kowalik A, Gozdz S. Evaluation of Complete Pathological Regression after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients with BRCA1 Founder Mutation Aided Bayesian A/B Testing Approach. Diagnostics. 2021; 11(7):1144. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071144
Chicago/Turabian StyleKedzierawski, Piotr, Pawel Macek, Izabela Ciepiela, Artur Kowalik, and Stanislaw Gozdz. 2021. "Evaluation of Complete Pathological Regression after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients with BRCA1 Founder Mutation Aided Bayesian A/B Testing Approach" Diagnostics 11, no. 7: 1144. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071144