
Perioperative GABA Blood Concentrations in Infants with Cyanotic and Non-Cyanotic Congenital Heart Diseases

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Monitoring Parameters
2.2. Perioperative Near Infrared Spectroscopy (NIRS)
2.3. Anesthetic Technique
2.4. Cardiopulmonary by-Pass Management
2.5. GABA Measurement
2.6. Neurological Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Perioperative Parameters
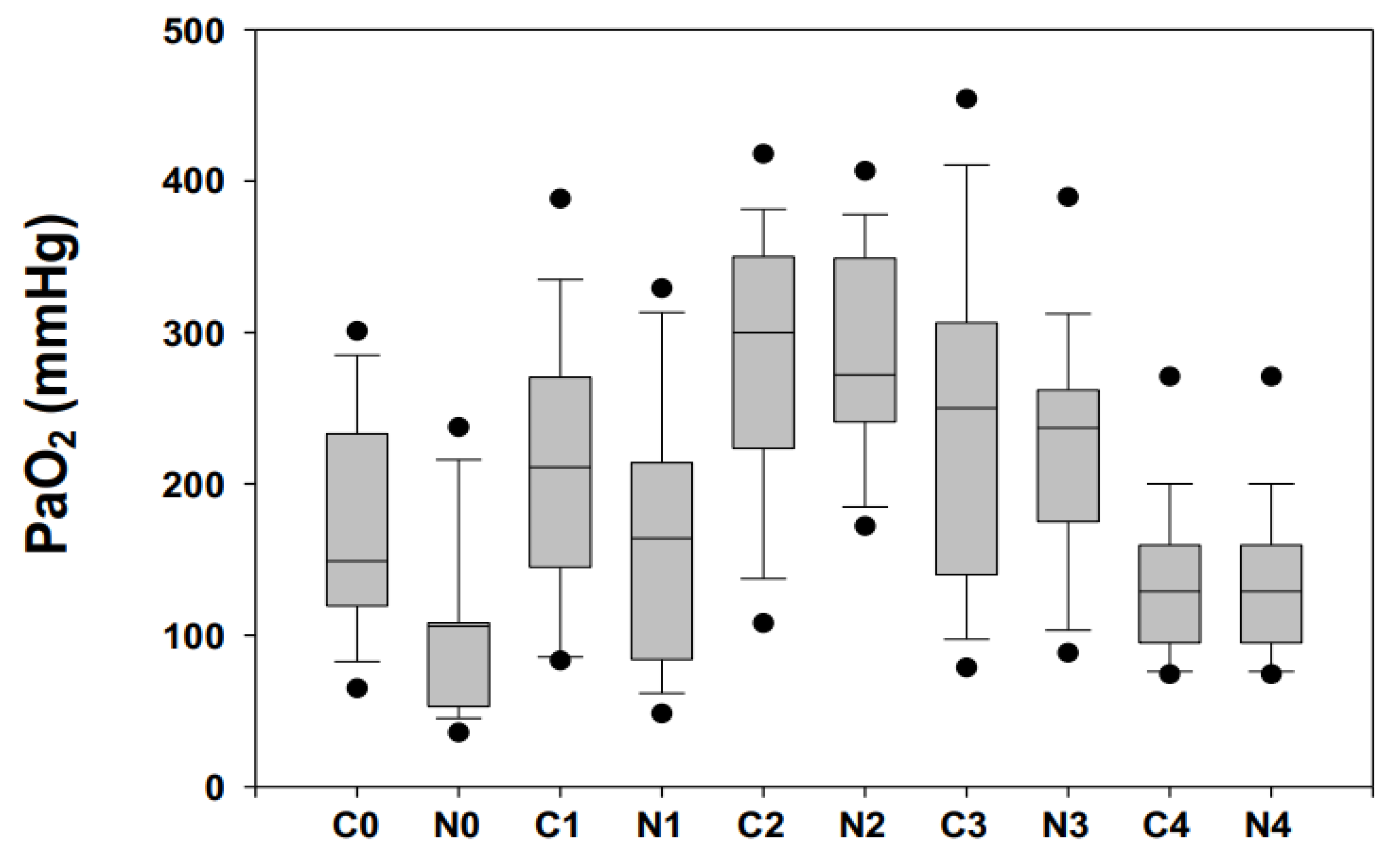
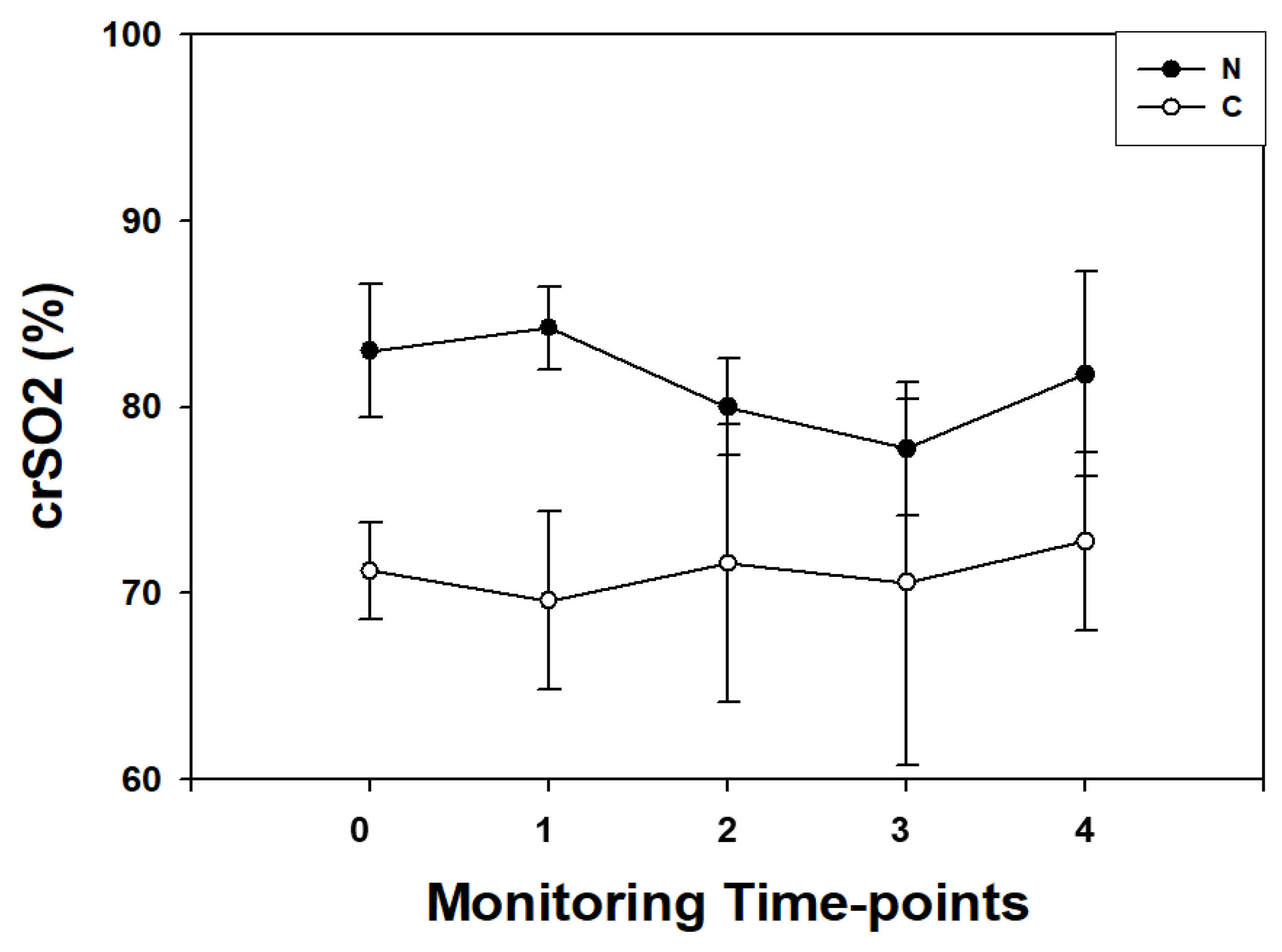
3.2. Near-Infrared Spectroscopy Recordings
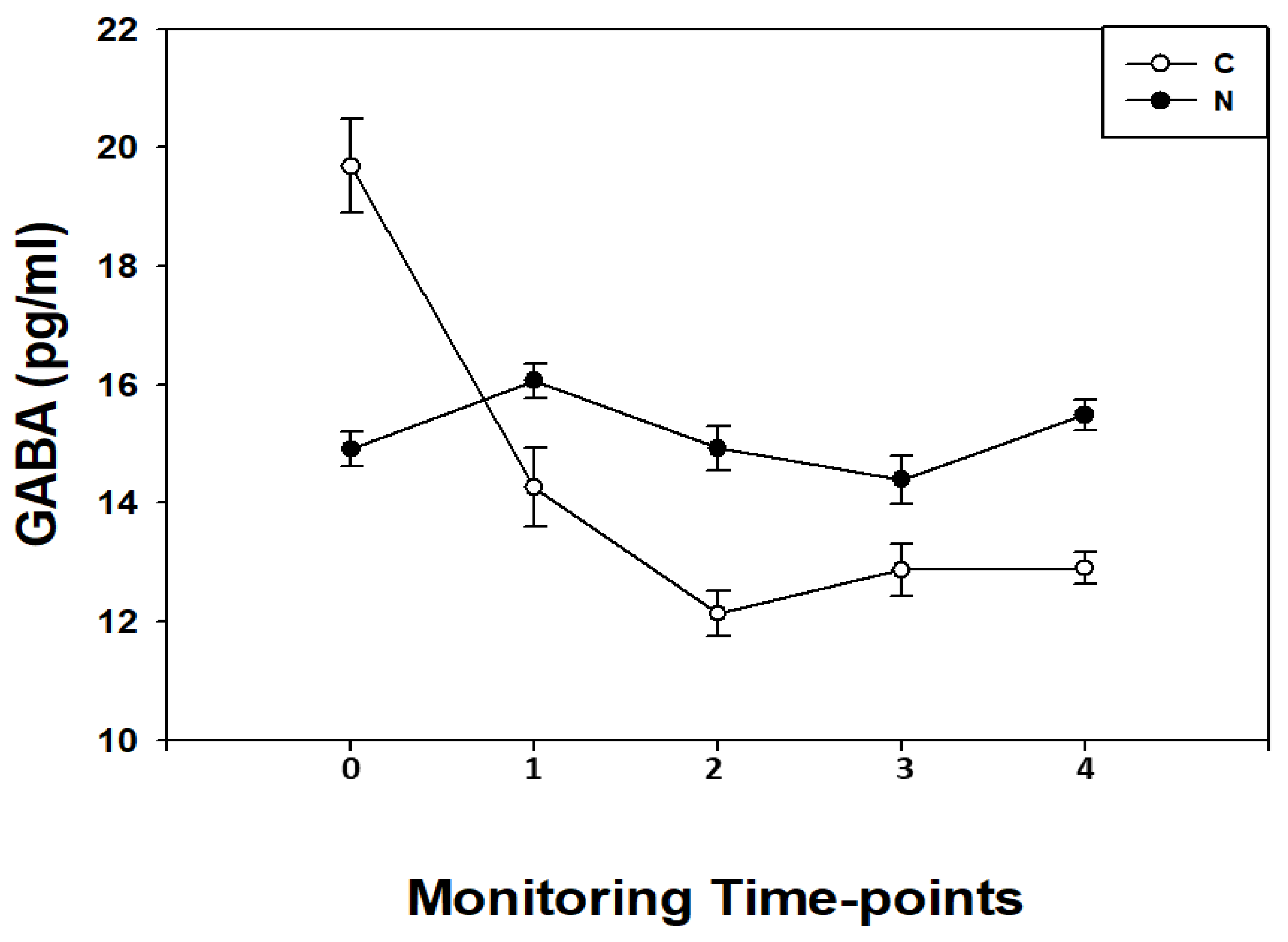
3.3. GABA Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BP | blood pressure |
| BW | body weight |
| C | cyanotic cardiac heart disease |
| CHD | cardiac heart disease |
| CPB | cardiopulmonary bypass |
| crSO2 | cerebral regional oxygen saturation |
| EB | base excess |
| GABA | Ɣ amino-aminobutyric acid |
| HB | hemoglobin concentration |
| HCO3 | bicarbonate |
| HI | hypoxia-ischemia injury |
| Ht | hematocrit rate percentage |
| LA | left atrium |
| RA | right atrium |
| MUF | modified ultrafiltration |
| N | non-cyanotic cardiac heart disease |
| 0 | before the surgical procedure |
| 1 | during the surgical procedure after sternotomy before CPB |
| 2 | at the end of CPB |
| 3 | at the end of the surgical procedure |
| 4 | 24-h after the surgical procedure |
| NIRS | near-infrared spectroscopy |
| PaCO2 | carbon dioxide partial pressures |
| PaO2 | oxygen partial pressures |
| RA | right atrium |
| SaO2 | oxygen saturation |
References
- Hsia, T.Y.; Gruber, P.J. Factors influencing neurologic outcome after neonatal cardiopulmonary bypass: What we can and cannot control. Ann. Thorac. Surg. 2006, 81, 2381–2388. [Google Scholar] [CrossRef]
- Triedman, J.K.; Newburger, J.W. Trends in congenital heart disease, the next decade. Circulation 2016, 133, 2716–2733. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G.; Buja, L.M. Congenital heart disease: Pathology, natural history, and interventions. In Cardiovascular Pathology, 4th ed.; Buja, L.M., Butany, J., Eds.; Academic Press/Elsevier: Waltham, MA, USA, 2016; pp. 611–647. [Google Scholar]
- Gazzolo, D.; Abella, R.; Marinoni, E.; Di Iorio, R.; Li Volti, G.; Galvano, F.; Pongiglione, G.; Frigiola, A.; Bertino, E.; Florio, P. Circulating biochemical markers of brain damage in infants complicated by ischemia reperfusion injury. Cardiovasc. Hematol. Agents. Med. Chem. 2009, 7, 108–126. [Google Scholar] [CrossRef]
- Abella, R.; Varrica, A.; Satriano, A.; Tettamanti, G.; Pellisero, G.; Gavilanes, A.D.; Zimmermann, L.J.; Hans, J.V.; Strozzi, M.C.; Pluchinotta, F.R.; et al. Biochemical markers for brain injury monitoring in children with or without congenital heart diseases. CNS Neurol. Disord. Drug. Targets 2015, 14, 12–23. [Google Scholar] [CrossRef]
- Kirklin, J.W.; Barratt-Boyes, B.G. Cardiac Surgery: Morphology, Diagnostic Criteria, Natural History, Techniques, Results and Indication; Churchill Livingston Inc.: New York, NY, USA, 1993; p. 77. [Google Scholar]
- Bersani, I.; Ferrari, F.; Lugli, L.; Ivani, G.; Conio, A.; Moataza, B.; Aboulgar, H.; Mufeed, H.; Iskander, I.; Kornacka, M.; et al. Monitoring the effectiveness of hypothermia in perinatal asphyxia infants by urinary S100B levels. Clin. Chem. Lab. Med. 2019, 57, 1017–1025. [Google Scholar] [CrossRef]
- Wisnowski, J.L.; Wu, T.W.; Reitman, A.J.; McLean, C.; Friedlich, P.; Vanderbilt, D.; Ho, E.; Nelson, M.; Panigraphy, A.; Blum, S. The effects of therapeutic hypothermia on cerebral metabolism in neonates with hypoxic-ischemic encephalopathy: An in vivo 1H-MR spectroscopy study. J. Cereb. Blood. Flow. Metabol. 2016, 36, 1075–1086. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.P.; McQuillen, P.S.; Hamrick, S.; Xu, D.; Glidden, D.V.; Charlton, N.; Karl, T.; Azakie, A.; Ferriero, D.M.; Barkovich, A.J.; et al. Abnormal brain development in newborns with congenital heart disease. N. Engl. J. Med. 2007, 357, 1928–1938. [Google Scholar] [CrossRef] [Green Version]
- Bersani, I.; Pluchinotta, F.; Dotta, A.; Savarese, I.; Campi, F.; Auriti, C.; Chuklantseva, N.; Piersigilli, F.; Gazzolo, F.; Varrica, A.; et al. Early predictors of perinatal brain damage: The role of neurobiomarkers. Clin. Chem. Lab. Med. 2020, 58, 471–486. [Google Scholar] [CrossRef] [Green Version]
- Bonham, A.C. Neurotransmitters in the CNS control of breathing. Respiration. Physiology 1995, 101, 219–230. [Google Scholar]
- Harbison, A.L.; Votava-Smith, J.K.; del Castillo, S.; Kumar, S.R.; Lee, V.; Schmithorst, V.; Lai, H.A.; O’Neil, S.; Bluml, S.; Paquette, L.; et al. Clinical Factors associated with cerebral metabolism in term neonates with congenital heart disease. J. Pediatr. 2017, 183, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, K.; Hatta, S.; Haga, M.; Ohshika, H. Effects of bilobalide on gamma-aminobutyric acid levels and glutamic acid decarboxylase in mouse brain. Eur. J. Pharmacol. 1999, 367, 165–173. [Google Scholar] [CrossRef]
- Varrica, A.; Satriano, A.; Frigiola, A.; Giamberti, A.; Tettamanti, G.; Anastasia, L.; Conforti, E.; Gavilanes, D.W.; Zimmermann, L.J.; Vles, H.J.S.; et al. Circulating S100B and adiponectin in children who underwent open heart surgery and cardiopulmonary bypass. BioMed Res. Int. 2015, 2015, 402–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumer, J.L. Clinical Pharmacology of midazolam in infants and children. Clin. Pharmacokinet. 1998, 35, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Gazzolo, D.; Vinesi, P.; Geloso, M.C.; Marcelletti, C.; Iorio, F.S.; Cipriani, A.; Marianeschi, S.M.; Michetti, F. S100 blood concentrations in children subjected to cardiopulmonary by-pass. Clin. Chem. 1998, 44, 1058–1060. [Google Scholar] [CrossRef] [Green Version]
- Gaynor, J.W. The effect of modified ultrafiltration on the postoperative course in patients with congenital heart disease. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2003, 6, 128–139. [Google Scholar] [CrossRef]
- Fuks, J.M.; Arrighi, R.B.; Weidner, J.M.; Kumar Mendu, S.; Jin, Z.; Wallin, R.P.; Rethi, B.; Birnir, B.; Barragan, A. GABAergic signaling is linked to a hypermigratory phenotype in dendritic cells infected by Toxoplasma gondii. PLoS Pathog. 2012, 8, e1003051. [Google Scholar] [CrossRef] [Green Version]
- Tina, L.G.; Frigiola, A.; Abella, R.; Artale, B.; Puleo, G.; Musmarra, S.D.C.; Tagliabue, P.; Li Volti, G.; Florio, P.; Gazzolo, D. Near Infrared Spectroscopy in healthy preterm and term newborns: Correlation with gestational age and standard monitoring parameters. Curr. Neurovasc. Res. 2009, 6, 148–154. [Google Scholar] [CrossRef]
- Lim, J.M.; Kingdom, T.; Saini, B.; Chau, V.; Post, M.; Blaser, S.; Macgowan, C.; Miler, S.; Seed, M. Cerebral oxygen delivery is reduced in newborns with congenital heart disease. J. Thorac. Cardiovasc. Surg. 2016, 152, 1095–1103. [Google Scholar] [CrossRef] [Green Version]
- Seco, M.; Edelman, J.J.; Wilson, M.K.; Bannon, P.G.; Vallely, M.P. Serum biomarkers of neurologic injury in cardiacoperations. Ann. Thorac. Surg. 2012, 94, 1026–1033. [Google Scholar] [CrossRef]
- Gazzolo, D.; Masetti, P.; Kornacka, M.; Abella, R.; Bruschettini, P.; Michetti, F. Phentolamine administration increases blood S100B protein levels in pediatric open-heart surgery patients. Acta Paediatr. 2003, 92, 1427–1432. [Google Scholar] [CrossRef]
- Petroff, O.A. GABA and glutamate in the human brain. Neuroscientist 2002, 8, 562–573. [Google Scholar] [CrossRef]
- Hall, K.A.A.; DeLane, S.E.; Anderson, G.M.; Lago, T.R.; Shor, R.; Wang, W.; Rasmusson, A.M.; Pineles, S.L. Plasma gamma-aminobutyric acid (GABA) levels and posttraumatic stress disorder symptoms in trauma-exposed women: A preliminary report. Psychopharmacology 2021, 238, 1541–1552. [Google Scholar] [CrossRef]
- Algra, S.O.; Jansen, N.J.; van der Tweel, I.; Schouten, A.N.; Groenendaal, F.; Toet, M.; van Oeveren, W.; van Haastert, I.C.; Schoof, P.H.; de Vries, L.S.; et al. Neurological injury after neonatal cardiac surgery: A randomized, controlled trial of 2 perfusion techiques. Circulation 2014, 129, 224–233. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.G.; Bottiglieri, T.; Snead, O.C. GABA, gamma-hydroxybutyric acid and neurological disease. Ann. Neurol. 2003, 54, 3–12. [Google Scholar] [CrossRef]
- Buckberg, G.D. Studies of hypoxemic/reoxygenation injury: I. Linkage between cardiac function and oxidant damage. J. Thorac. Cardiovasc. Surg. 1995, 110, 1164–1170. [Google Scholar] [CrossRef] [Green Version]
- Morita, K.; Ihnken, K.; Buckberg, G.D. Studies of hypoxemic/reoxygenation injury: With aortic clamping. XII. Delay of cardiac reoxygenation damage in the presence of cyanosis: A new concept of controlled cardiacreoxygenation. J. Thorac. Cardiovasc. Surg. 1995, 110, 1265–1273. [Google Scholar] [CrossRef] [Green Version]
- Del Nido, P.J.; Mickle, D.A.; Wilson, G.J.; Harding, R.D.; Romaschin, A.D. Evidence of myocardial free radical injury during elective repair of tetralogy of Fallot. Circulation 1987, 76, 174–179. [Google Scholar]
- Schurr, A. Lactate, glucose and energy metabolism in the ischemic brain. Int. J. Mol. Med. 2002, 10, 131–136. [Google Scholar] [CrossRef]
- Arrica, M.; Bissonnette, B. Therapeutic hypothermia. Semin. Cardiothorac. Vasc. Anesth. 2007, 11, 6–15. [Google Scholar] [CrossRef]
- Caputo, M.; Mokhtari, A.; Miceli, A.; Ghorbel, M.T.; Angelini, G.D.; Parry, A.; Suleiman, S.M. Controlled reoxygenation during cardiopulmonary bypass decreases markers of organ damage, inflammation, and oxidative stress in single-ventricle patients undergoing pediatric heart surgery. J. Thorac. Cardiovasc. Surg. 2014, 148, 792–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, P.; Masaoka, H.; Kuroiwa, T.; Wagner, H.; Fenton, I.; Klatzo, I. Influence of blood–brain barrier opening to proteins on development of post-ischaemic brain injury. Neurol. Res. 1986, 8, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Serpero, L.D.; Bianchi, V.; Pluchinotta, F.; Conforti, E.; Baryshnikova, E.; Guaschino, R.; Cassinari, M.; Trifoglio, O.; Calevo, M.G.; Gazzolo, D. S100B maternal blood levels are gestational age- and gender-dependent in healthy pregnancies. Clin. Chem. Lab. Med. 2017, 55, 1770–1776. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | C (n = 33) | N (n = 35) |
|---|---|---|
| Age (months) | 23 ± 11 | 30 ± 8 * |
| Weight (Kg) | 12 ± 1 | 16 ± 3 * |
| Gender (F/M) | 11/23 | 12/22 |
| Laboratory parameters | ||
| Hemoglobin (g/dL) | 13.5 ± 1.4 | 12.9 ± 2.0 |
| Hematocrit (%) | 39.9 ± 3.9 | 38.5 ± 4.9 |
| Platelet count (103/mmc) | 329 ± 107 | 335 ± 99 |
| Creatinine (mg/dL) | 0.5 ± 0.3 | 0.5 ± 0.2 |
| Urea (mg/dL) | 39 ± 11 | 37 ± 12 |
| LDH (UI/L) | 565 ± 199 | 532 ± 206 |
| CK (UI/L) | 168 ± 112 | 173 ± 109 |
| Neurological examination before surgery | ||
| Normal/suspect/abnormal | 34/0/0 | 34/0/0 |
| Main interventions | ||
| CPB (min) | 88 ± 22 | 59 ± 25 * |
| Filtration (n/total) | 19/34 | 17/34 |
| Clamping (min) | 79 ± 25 * | 47 ± 29 * |
| Circulatory arrest (n/total) | 8/34 | 1/34 * |
| Cooling (°C) | 31 ± 3 | 27 ± 2 * |
| Parameters | T0 N | T0 C | T1 N | T1 C | T2 N | T2 C | T3 N | T3 C | T4 N | T4 C |
|---|---|---|---|---|---|---|---|---|---|---|
| Hb (g/dL) | 12.5 ± 2.1 | 12.2 ± 1.9 | 11.8 ± 2.3 | 12.1 ± 2.2 | 11.5 ± 2.9 | 11.7 ± 1.9 | 11.4 ± 1.8 | 11.3 ± 2.6 | 11.8 ± 1.8 | 11.6 ± 1.4 |
| Ht (%) | 35.7 ± 2.8 | 35.2 ± 2.2 | 34.1 ± 4.9 | 34.9 ± 3.7 | 32.9 ± 7.3 | 33.5 ± 3.1 | 32.8 ± 3.7 | 33.6 ± 2.2 | 34.7 ± 3.7 | 34.3 ± 4.1 |
| pH | 7.31 ± 0.10 | 7.34 ± 0.12 | 7.36 ± 0.11 | 7.35 ± 0.12 | 7.38 ± 0.09 | 7.36 ± 0.10 | 7.37 ± 0.11 | 7.36 ± 0.13 | 7.41 ± 0.08 | 7.40 ± 0.09 |
| PaCO2 (mmHg) | 35.4 ± 4.9 | 35.6 ± 5.3 | 35.4 ± 3.8 | 36.2 ± 4.5 | 34.7 ± 5.2 | 36.1 ± 3.1 | 36.8 ± 4.4 | 35.5 ± 3.4 | 36.3 ± 5.7 | 35.8 ± 6.0 |
| PaO2 (mmHg) | 205.3 ± 94 | 107 ± 18 * | 186 ± 72 | 150 ± 48 * | 266 ± 68 | 290 ± 67 | 185 ± 78 | 138 ± 63 * | 183 ± 55 | 138 ± 46 |
| H2CO3 | 23.1 ± 3.1 | 22.5 ± 2.3 | 21.8 ± 2.9 | 21.9 ± 4.6 | 21.5 ± 3.8 | 21.9 ± 4.0 | 22.7 ± 1.5 | 21.8 ± 2.3 | 22.4 ± 1.7 | 22.1 ± 1.5 |
| BE | 0.3 ± 2.4 | 0.2 ± 1.6 | −1.9 ± 3.3 | −1.5 ± 3.1 | −3.0 ± 2.3 | −2.3 ± 2.9 | −0.3 ± 0.9 | 0.8 ± 2.1 | 1.6 ± 1.7 | 1.5 ± 1.4 |
| SaO2 (mmHg) | 98.4 ± 2.6 | 82.4 ± 7.8 * | 97.8 ± 0.4 | 84.2 ± 8.7 * | 97.5 ± 1.9 | 96.0 ± 2.1 | 95.9 ± 1.6 | 94.8 ± 3.8 | 95.5 ± 4.6 | 93.1 ± 4.7 |
| HR (bpm) | 106 ± 10 | 111 ± 15 | 112 ± 13 | 111 ± 10 | 124 ± 12 | 118 ± 15 | 124 ± 14 | 134 ± 16 | 127 ± 18 | 123 ± 13 |
| LA BP (mmHg) | 9.0 ± 3.7 | 7.9 ± 2.9 | 7.7 ± 3.0 | 7.4 ± 3.9 | 9.3 ± 3.5 | 8.9 ± 4.3 | 9.3 ± 5.1 | 8.6 ± 3.2 | 9.4 ± 4.1 | 9.3 ± 3.9 |
| RA BP (mmHg) | 9.4 ± 2.5 | 9.2 ± 1.8 | 8.8 ± 1.4 | 8.9 ± 1.6 | 8.8 ± 2.3 | 8.4 ± 2.8 | 8.9 ± 2.7 | 7.8 ± 2.2 | 10 ± 2.9 | 11 ± 2.3 |
| S BP (mmHg) | 89 ± 12 | 86 ± 13 | 87 ± 19 | 86 ± 15 | 87 ± 14 | 85 ± 12 | 88 ± 16 | 86 ± 13 | 97 ± 10 | 95 ± 15 |
| D BP (mmHg) | 43 ± 14 | 44 ± 9 | 54 ± 11 | 53 ± 13 | 55 ± 10 | 56 ± 9 | 50 ± 11 | 54 ± 14 | 58 ± 12 | 56 ± 10 |
| Glycaemia (mg/dL) | 103 ± 10 | 105 ± 8 | 117 ± 10 | 115 ± 14 | 129 ± 16 | 117 ± 10 | 110 ± 22 | 124 ± 13 | 118 ± 15 | 120 ± 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satriano, A.; Varrica, A.; Frigiola, A.; Graziosi, A.; Di Battista, C.; Primavera, A.P.; Centini, G.; Maconi, A.; Strozzi, C.; Gavilanes, A.D.W.; et al. Perioperative GABA Blood Concentrations in Infants with Cyanotic and Non-Cyanotic Congenital Heart Diseases. Diagnostics 2021, 11, 1149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071149
Satriano A, Varrica A, Frigiola A, Graziosi A, Di Battista C, Primavera AP, Centini G, Maconi A, Strozzi C, Gavilanes ADW, et al. Perioperative GABA Blood Concentrations in Infants with Cyanotic and Non-Cyanotic Congenital Heart Diseases. Diagnostics. 2021; 11(7):1149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071149
Chicago/Turabian StyleSatriano, Angela, Alessandro Varrica, Alessandro Frigiola, Alessandro Graziosi, Caterina Di Battista, Adele Patrizia Primavera, Giacomo Centini, Antonio Maconi, Chiara Strozzi, Antonio D. W. Gavilanes, and et al. 2021. "Perioperative GABA Blood Concentrations in Infants with Cyanotic and Non-Cyanotic Congenital Heart Diseases" Diagnostics 11, no. 7: 1149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071149