
Forecasting COVID-19 Severity by Intelligent Optical Fingerprinting of Blood Samples

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
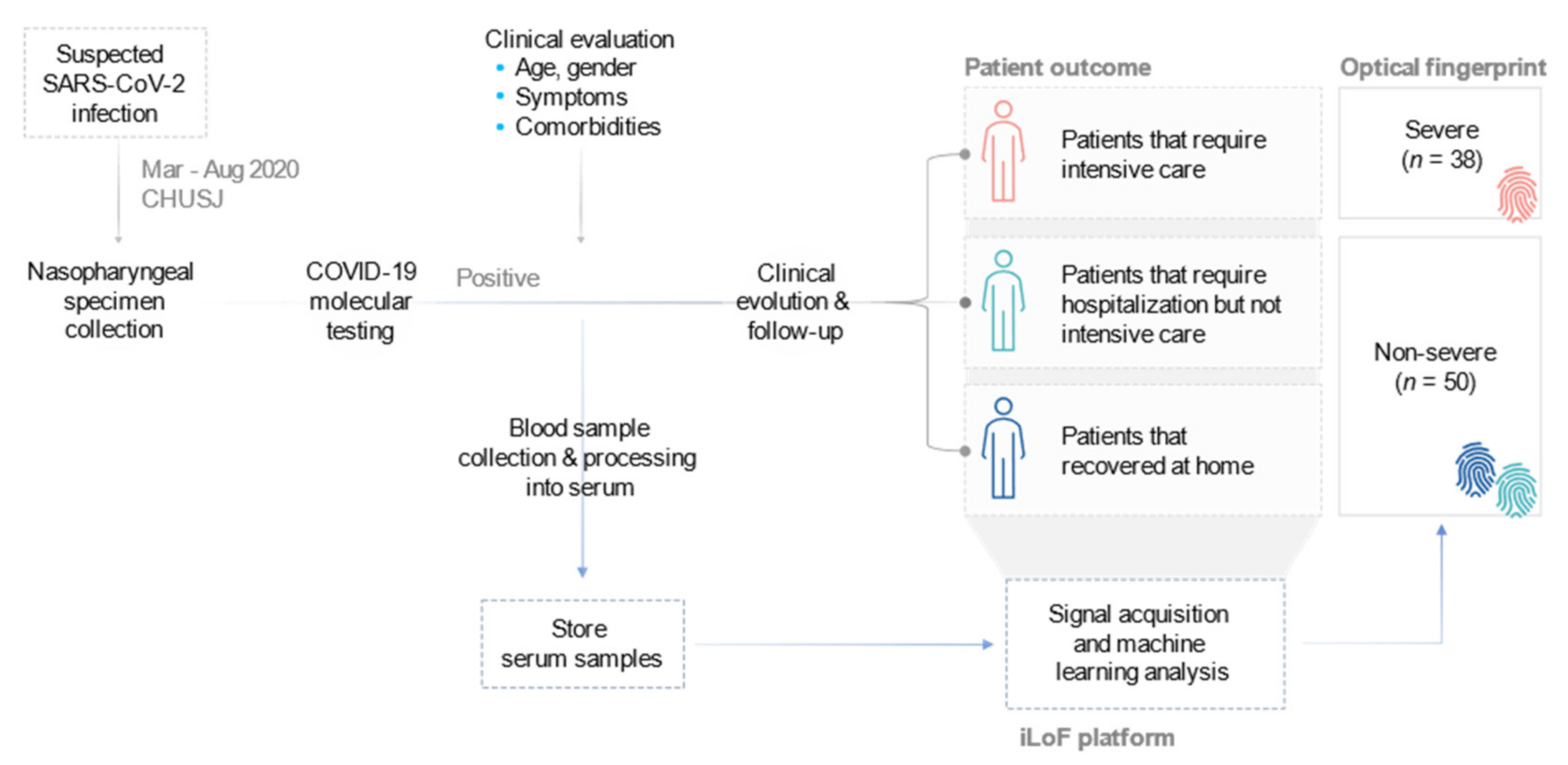
2.1. Description of the Prospective Study
2.2. Sample Collection and Preparation
2.3. Probe Fabrication
2.4. Data Acquisition
2.5. Signal Processing
2.6. Feature Definition
2.7. Model Development
2.8. Statistical Analysis
3. Results
3.1. Study Design and Cohort Characteristics
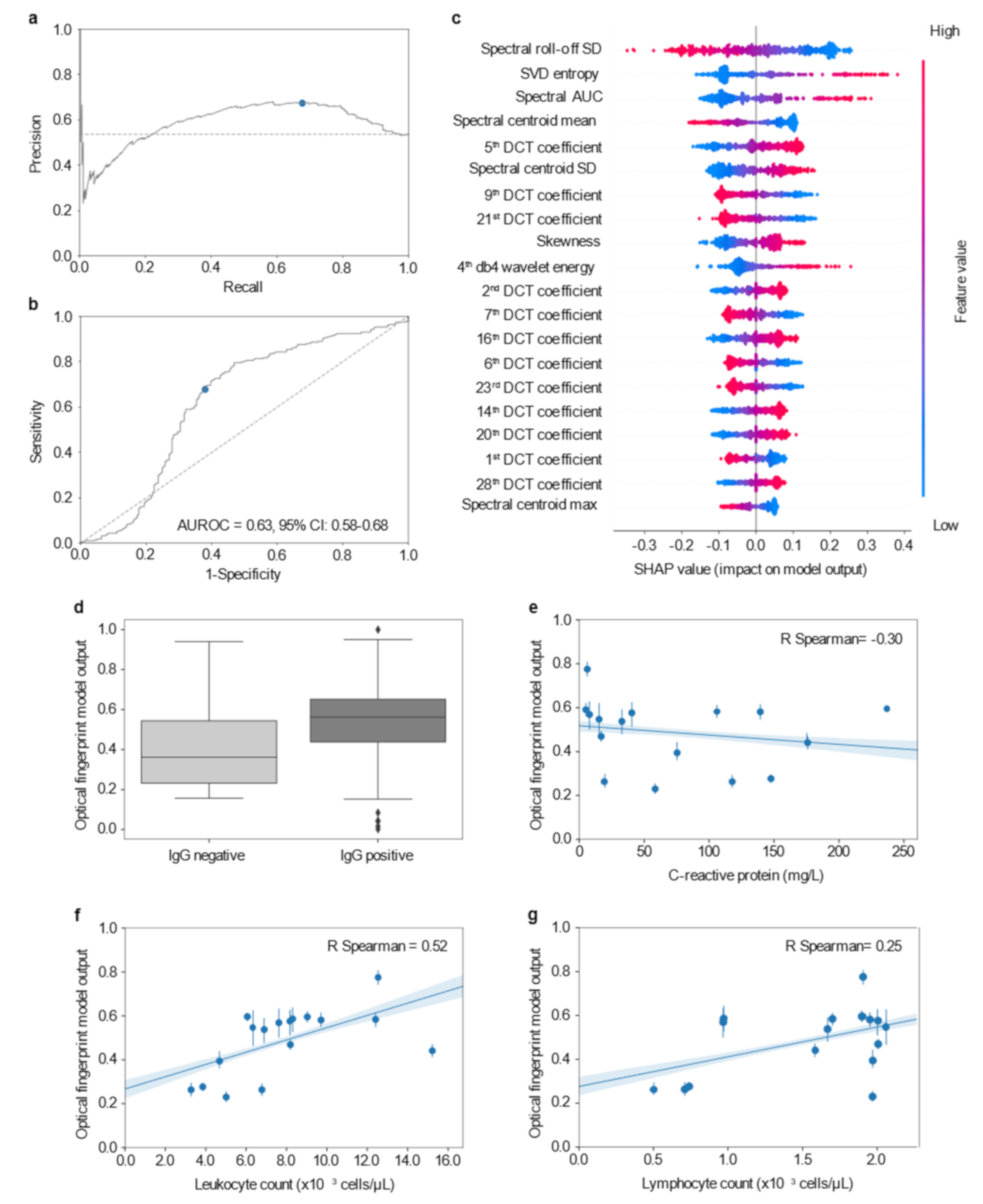
3.2. Optical Fingerprinting of COVID-19 Serum Samples Provides Unique Information for Severity Prediction
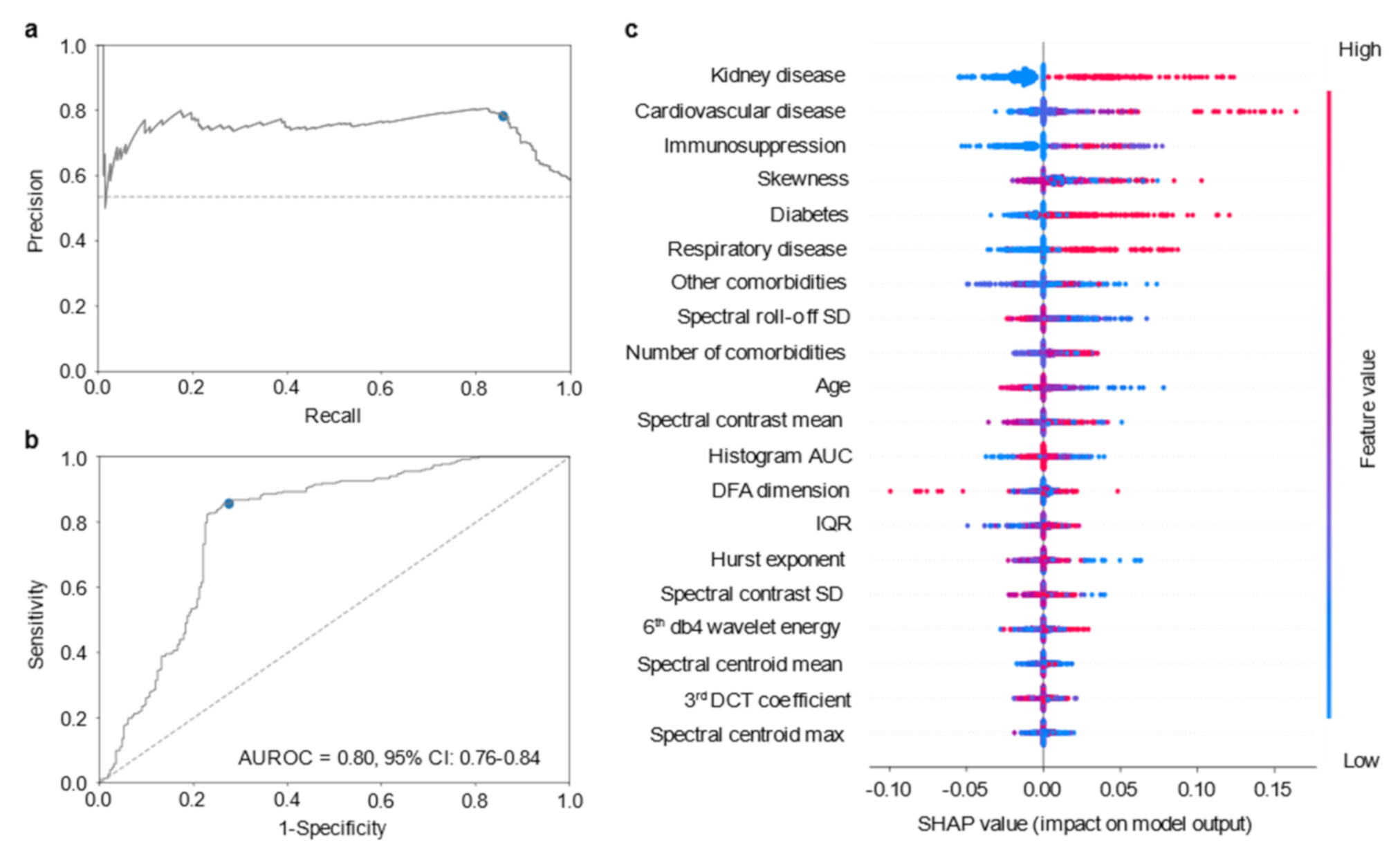
3.3. Stacking Ensemble Model Based on Optical Fingerprinting, Comorbidities and Age Information
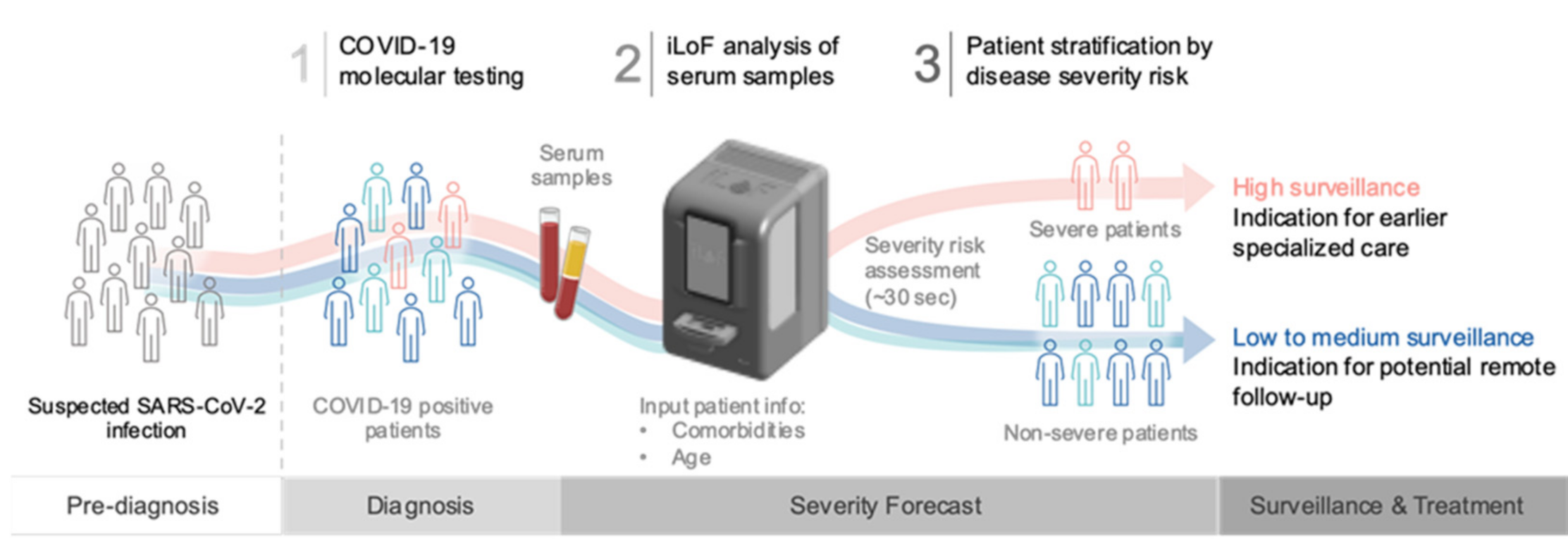
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting characteristics, comorbidities and outcomes among 5700 patients hospitalized With COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: Summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO clinical characterisation protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Furlow, B. COVACTA trial raises questions about tocilizumab’s benefit in COVID-19. Lancet Rheumatol. 2020, 2, e592. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the treatment of Covid-19—final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19—preliminary report. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef]
- Paiva, J.S.; Jorge, P.; Ribeiro, R.S.R.; Balmaña, M.; Campos, D.; Mereiter, S.; Jin, C.; Karlsson, N.G.; Sampaio, P.; Reis, C.A.; et al. iLoF: An intelligent lab on fiber approach for human cancer single-cell type identification. Sci. Rep. 2020, 10, 3171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, J.S.; Jorge, P.A.S.; Ribeiro, R.S.R.; Sampaio, P.; Rosa, C.C.; Cunha, J.P.S. Optical fiber-based sensing method for nanoparticle detection through supervised back-scattering analysis: A potential contributor for biomedicine. Int. J. Nanomed. 2019, 14, 2349–2369. [Google Scholar] [CrossRef] [Green Version]
- Xu, R. Light scattering: A review of particle characterization applications. Particuology 2015, 18, 11–21. [Google Scholar] [CrossRef]
- Ribeiro, R.S.R.; Queirós, R.; Soppera, O.; Guerreiro, A.; Jorge, P.A.S. Optical fiber tweezers fabricated by guided wave photo-polymerization. Photonics 2015, 2, 634–645. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, R.S.R.; Soppera, O.; Oliva, A.; Guerreiro, A.; Jorge, P. New trends on optical fiber tweezers. J. Lightwave Technol. 2015, 33, 3394–3405. [Google Scholar] [CrossRef]
- Paiva, J.S.; Ribeiro, R.S.R.; Cunha, J.P.S.; Rosa, C.C.; Jorge, P.A.S. Single particle differentiation through 2D optical fiber trapping and back-scattered signal statistical analysis: An exploratory approach. Sensors 2018, 18, 710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, R.S.R.; Dahal, P.; Guerreiro, A.; Jorge, P.A.S.; Viegas, J. Fabrication of fresnel plates on optical fibres by FIB milling for optical trapping, manipulation and detection of single cells. Sci. Rep. 2017, 7, 4485. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.M.; Paiva, J.S.; Ribeiro, R.S.R.; Soppera, O.; Cunha, J.P.S.; Jorge, P.A.S. Fabrication of multimode-single mode polymer fiber tweezers for single cell trapping and identification with improved performance. Sensors 2018, 18, 2746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckardt, R.C. Nonlinear Optics, Basics|χ(2)–Harmonic Generation; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Marques de Sá, J.P. Pattern Recognition: Concepts, Methods and Applications; Springer: Berlin, Germany, 2001. [Google Scholar]
- Hosseinifard, B.; Moradi, M.H.; Rostami, R. Classifying depression patients and normal subjects using machine learning techniques and nonlinear features from EEG signal. Comput. Methods Programs Biomed. 2013, 109, 339–345. [Google Scholar] [CrossRef]
- Dubnov, S. Generalization of spectral flatness measure for non-gaussian linear processes. IEEE Signal Process. Lett. 2004, 11, 698–701. [Google Scholar] [CrossRef]
- Jiang, D.-N.; Lu, L.; Zhang, H.-J.; Tao, J.-H.; Cai, L.-H. Music type classification by spectral contrast feature. In Proceedings of the 2002 IEEE International Conference on Multimedia and Expo, Lausanne, Switzerland, 26–29 August 2002; pp. 113–116. [Google Scholar]
- Kesić, S.; Spasić, S.Z. Application of higuchi’s fractal dimension from basic to clinical neurophysiology: A review. Comput. Methods Programs Biomed. 2016, 133, 55–70. [Google Scholar] [CrossRef]
- Wolpert, D.H. Stacked generalization. Neural Netw. 1992, 5, 241–259. [Google Scholar] [CrossRef]
- Lundberg, S.; Lee, S.-I. Advances in Neural Information Processing Systems; Curran Associates, Inc.: Long Beach, CA, USA, 2017; pp. 4765–4774. [Google Scholar]
- Duda, R.O.; Hart, P.E.; Stork, D.G. Pattern Classification, 2nd ed.; Wiley-Interscience Publication: Hoboken, NJ, USA, 2001. [Google Scholar]
- Clopper, C.J.; Pearson, E.S. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika 1934, 26, 404–413. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating char-acteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef] [PubMed]
- Lassau, N.; Ammari, S.; Chouzenoux, E.; Gortais, H.; Herent, P.; Devilder, M.; Soliman, S.; Meyrignac, O.; Talabard, M.-P.; Lamarque, J.-P.; et al. Integrating deep learning CT-scan model, biological and clinical variables to predict severity of COVID-19 patients. Nat. Commun. 2021, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sill, J.; Takacs, G.; Mackey, L.; Lin, D. Feature-weighted linear stacking. arXiv 2009, arXiv:abs/0911.0460, Preprint. [Google Scholar]
- Feng, Z.; Yu, Q.; Yao, S.; Luo, L.; Zhou, W.; Mao, X.; Li, J.; Duan, J.; Yan, Z.; Yang, M.; et al. Early prediction of disease progression in COVID-19 pneumonia patients with chest CT and clinical characteristics. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Garibaldi, B.T.; Fiksel, J.; Muschelli, J.; Robinson, M.L.; Rouhizadeh, M.; Perin, J.; Schumock, G.; Nagy, P.; Gray, J.H.; Malapati, H.; et al. Patient trajectories among persons hospitalized for COVID-19. Ann. Intern. Med. 2021, 174, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and validation of a clinical risk score to predict the occurrence of critical illness in hospitalized patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically applicable AI system for accurate diagnosis, quantitative measurements and prognosis of COVID-19 pneumonia using computed tomography. Cell 2020, 181, 1423–1433.e11. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of COVID-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]
- Foy, B.H.; Carlson, J.C.T.; Reinertsen, E.; Valls, R.P.I.; Lopez, R.P.; Palanques-Tost, E.; Mow, C.; Westover, M.B.; Aguirre, A.D.; Higgins, J.M. Association of red blood cell distribution width with mortality risk in hospitalized adults with SARS-CoV-2 infection. JAMA Netw. Open 2020, 3, e2022058. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; González-Rivera, M.; Almansa, R.; Micheloud, D.; Tedim, A.P.; Domínguez-Gil, M.; Resino, S.; Martín-Fernández, M.; Murua, P.R.; Pérez-García, F.; et al. Viral RNA load in plasma is associated with critical illness and a dysregulated host response in COVID-19. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Scozzi, D.; Cano, M.; Ma, L.; Zhou, D.; Zhu, J.H.; O’Halloran, J.A.; Goss, C.W.; Rauseo, A.M.; Liu, Z.; Sahu, S.K.; et al. Circulating mitochondrial DNA is an early indicator of severe illness and mortality from COVID-19. JCI Insight 2021, 6, 143299. [Google Scholar] [CrossRef] [PubMed]
- O’Dell, D.; Schein, P.; Erickson, D. Simultaneous characterization of nanoparticle size and particle-surface interactions with three-dimensional nanophotonic force microscopy. Phys. Rev. Appl. 2016, 6, 034010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, M.; Nir, G.; Vivante, A.; Young, I.T.; Garini, Y. Dynamic analysis of a diffusing particle in a trapping potential. Phys. Rev. E 2013, 87, 022716. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Severe Group (n = 38) | Non-Severe Group (n = 50) | p Value | ||
|---|---|---|---|---|---|
| Patients | Missing Data | Patients | Missing Data | ||
| Age (y), median (IQR) | 71 (61–77) | 64 (46–83) | 0.2870 | ||
| Gender (Male) | 28 (73.7%) | 22 (44.0%) | 0.0087 | ||
| Comorbidities, N (%) | 1 (2.6%) | 5 (10.0%) | |||
| Kidney disease | 10 (27.0%) | 3 (6.7%) | 0.0157 | ||
| Cardiovascular disease | 29 (78.4%) | 20 (44.4%) | 0.0030 | ||
| Immunosuppressed | 11 (29.7%) | 5 (11.1%) | 0.0496 | ||
| Diabetes | 18 (48.6%) | 9 (20.0%) | 0.0091 | ||
| Respiratory disease | 9 (24.3%) | 4 (8.9%) | 0.0724 | ||
| Obesity | 7 (18.9%) | 2 (4.4%) | 0.0714 | ||
| Others | 19 (51.4%) | 24 (53.3%) | >0.9999 | ||
| Comorbidities per patient, N (%) | 0.0051 | ||||
| 0 | 3 (7.9%) | 13 (26.0%) | |||
| 1 or 2 | 9 (23.7%) | 15 (30.0%) | |||
| 3 or 4 | 11 (28.9% | 13 (26.0%) | |||
| ≥5 | 14 (36.8%) | 4 (8.0%) | |||
| C-reactive peptide (mg/L), median (IQR) | 117.0 (46.1–190.6) | 21.1 (6.5–69.8) | <0.0001 | ||
| Leukocyte count (×103 cells/uL), median (IQR) | 7.6 (6.0–10.9) | 5.6 (4.5–8.3) | 0.0112 | ||
| Lymphocyte count (×103 cells/uL), median (IQR) | 1.1 (0.6–1.7) | 1.4 (0.8–1.8) | 1 (2.0%) | 0.1645 | |
| IgG (Positive), N (%) | 28 (75.7%) | 1 (2.6%) | 19 (38.0%) | 0.0006 | |
| Model | AUC | Accuracy | Sensitivity | Specificity | Precision |
|---|---|---|---|---|---|
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Optical fingerprint, comorbidities, age | 0.80 | 79.6% | 85.7% | 72.6% | 78.3% |
| (0.76–0.84) | (75.8–83.0) | (81.0-89.6) | (66.4–78.2) | (73.2–82.8) | |
| Optical fingerprint | 0.63 **** | 65.1% | 67.8% | 62.0% | 67.3% |
| (0.58–0.68) | (60.8–69.2) | (61.9–73.3) | (55.5–68.2) | (61.4–72.8) | |
| Comorbidities, age | 0.74 ** | 65.3% | 100.0% | 25.3% | 60.7% |
| (0.70–0.78) | (61.0-69.4) | (98.9–100.0) | (11.4–31.4) | (56.0–65.2) | |
| All clinical data(Comorbidities, age, laboratory parameters) | 0.75 * | 76.5% | 78.0% | 74.7% | 78.0% |
| (0.68–0.76) | (72.5–80.1) | (72.6–82.8) | (68.2–80.1) | (72.6–82.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faria, S.P.; Carpinteiro, C.; Pinto, V.; Rodrigues, S.M.; Alves, J.; Marques, F.; Lourenço, M.; Santos, P.H.; Ramos, A.; Cardoso, M.J.; et al. Forecasting COVID-19 Severity by Intelligent Optical Fingerprinting of Blood Samples. Diagnostics 2021, 11, 1309. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081309
Faria SP, Carpinteiro C, Pinto V, Rodrigues SM, Alves J, Marques F, Lourenço M, Santos PH, Ramos A, Cardoso MJ, et al. Forecasting COVID-19 Severity by Intelligent Optical Fingerprinting of Blood Samples. Diagnostics. 2021; 11(8):1309. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081309
Chicago/Turabian StyleFaria, Simão P., Cristiana Carpinteiro, Vanessa Pinto, Sandra M. Rodrigues, José Alves, Filipe Marques, Marta Lourenço, Paulo H. Santos, Angélica Ramos, Maria J. Cardoso, and et al. 2021. "Forecasting COVID-19 Severity by Intelligent Optical Fingerprinting of Blood Samples" Diagnostics 11, no. 8: 1309. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081309