
Diagnostic Performance of Serum Biomarkers Fibroblast Growth Factor 21, Galectin-3 and Copeptin for Heart Failure with Preserved Ejection Fraction in a Sample of Patients with Type 2 Diabetes Mellitus

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Characteristics
2.2. Biomarkers
2.3. Echocardiographic Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Sample of Patients with Type 2 DM
3.2. Comparisons of Serum FGF21, Galectin-3, Copeptin and Echocardiographic Parameters in Patients with Type 2 Diabetes Mellitus Grouped by Heart Failure
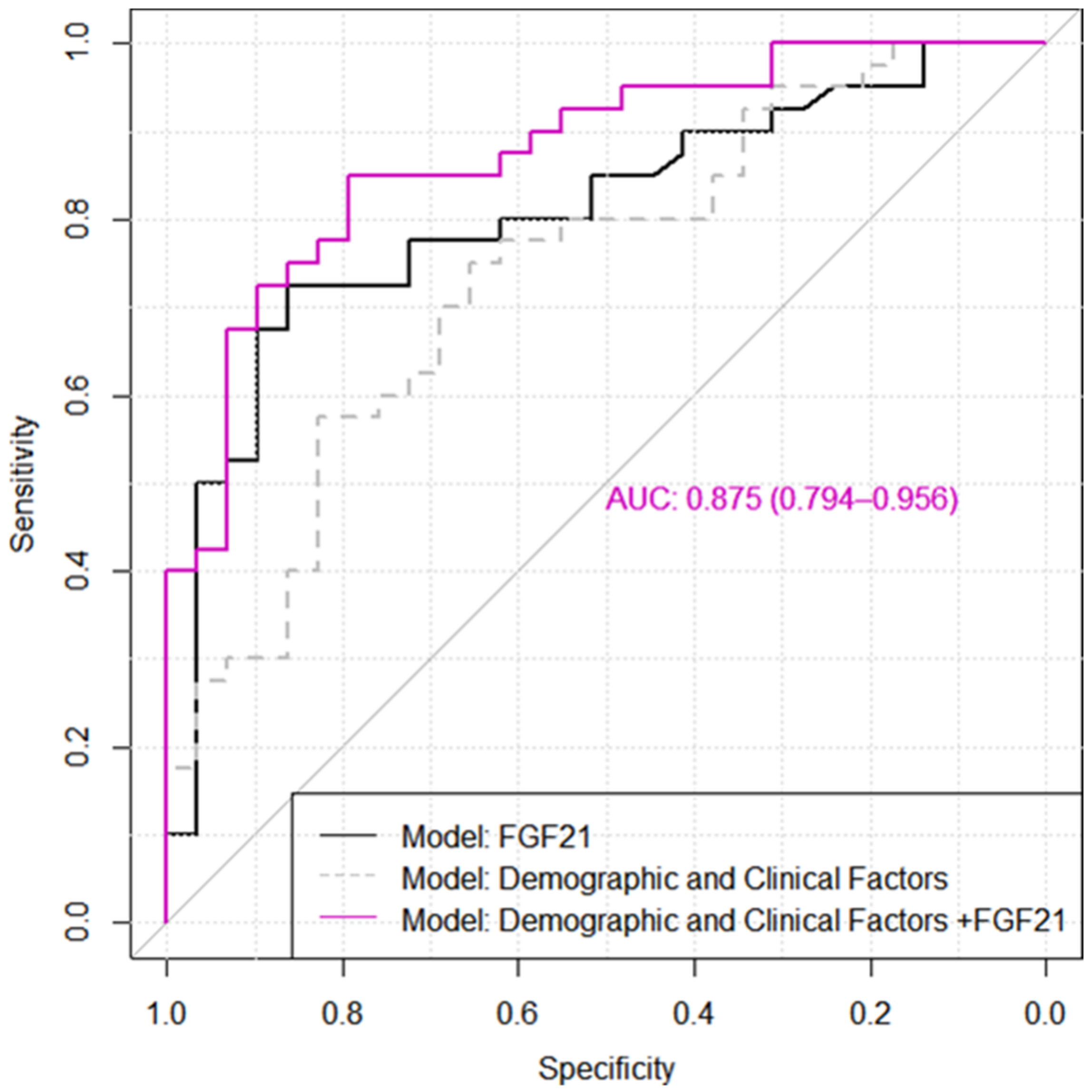
3.3. Evaluation of FGF21, Copeptin and Gal-3 as Markers of HFpEF in Patients with Type 2 DM
3.4. Correlations among FGF21, Galectin-3, and Copeptin with Clinical, Laboratory Data and Echocardiographic Variables in All Samples of Patients with Type 2 DM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seshasai, S.R.S.; Kaptoge, S.S. Emerging Risk Factors Collaboration. Diabetes mellitus, fasting glucose, and risk of cause specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar]
- Yuvashree, M.; Pragasam, V. Diabetic Cardiomyopathy: A New Perspective of Mechanistic Approach. J. Diabetes Metab. 2015, 6, 605. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Pieske, B.; Tschöpe, C.; de Boer, R.A.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F. How to diagnose heart failure with preserved ejection fraction: The HFA–PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 40, 3297–3317. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.L.; Chan, F.T.; Nabeebaccus, A.A.; Shah, A.M.; McDonagh, T.; Okonko, D.O. Drug treatment effects on outcomes in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Heart 2018, 104, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.H.; Huang, P.H.; Hsu, C.Y. Circulating Fibroblast Growth Factor 21 is Associated with Diastolic Dysfunction in Heart Failure Patients with Preserved Ejection Fraction. Sci. Rep. 2016, 6, 33953. [Google Scholar] [CrossRef] [PubMed]
- Palomer, C.X.; Delgado, J.P.; Vazquez-Carrera, M. Emerging Actors in Diabetic Cardiomyopathy: Heartbreaker Biomarkers or Therapeutic Targets? Trends Pharmacol. Sci. 2018, 39, 452–467. [Google Scholar] [CrossRef]
- Anjan, V.Y.; Loftus, T.M.; Burke, M.A.; Akhter, N.; Fonarow, G.C.; Gheorghiade, M.; Shah, S.J. Prevalence, clinical phenotype, and outcomes associated with normal B-type natriuretic peptide levels in heart failure with preserved ejection fraction. Am. J. Cardiol. 2012, 110, 870–876. [Google Scholar] [CrossRef] [Green Version]
- Borlaug, B.A.; Nishimura, R.A.; Sorajja, P.; Lam, C.S.; Redfield, M.M. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ. Heart Fail. 2010, 3, 588–595. [Google Scholar] [CrossRef] [Green Version]
- Meijers, W.C.; Hoekstra, T.; Jaarsma, T.; van Veldhuisen, D.J. Patients with heart failure with preserved ejection fraction and low levels of natriuretic peptides. Neth. Heart J. 2016, 24, 287–295. [Google Scholar] [CrossRef] [Green Version]
- Hage, C.; Lund, L.H.; Donal, E. Copeptin in patients with heart failure and preserved ejection fraction: A report from the prospective KaRen-study. Open Heart 2015, 2, e000260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugliese, G.P.; Iacobini, C.I. Galectin-3 in diabetic patients. Clin. Chem. Lab. Med. 2014, 52, 1413. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yang, L.; Xu, X.; Tang, F.; Yi, P.; Qiu, B.; Hao, Y. A review of fibroblast growth factor 21 in diabetic cardiomyopathy. Heart Fail. Rev. 2019, 24, 1005–1017. [Google Scholar] [CrossRef] [PubMed]
- Shao, M.; Yu, L.; Zhang, F.; Lu, X.; Li, X.; Cheng, P.; Lin, X.; He, L. Additive protection by LDR and FGF21 treatment against diabetic nephropathy in type 2 diabetes model. Am. J. Physiol. Endocrinol. Metab. 2015, 309, E45–E54. [Google Scholar] [CrossRef] [Green Version]
- Yafei, S.; Elsewy, F.; Youssef, E.; Ayman, M.; El-Shafei, M. Fibroblast growth factor 21 association with subclinical atherosclerosis and arterial stiffness in type 2 diabetes. Diabetes Metab. Syndr. 2019, 13, 882–888. [Google Scholar] [CrossRef]
- Zhang, W.; Chu, S.; Ding, W.; Wang, F. Serum Level of Fibroblast Growth Factor 21 Is Independently Associated with Acute Myocardial Infarction. PLoS ONE 2015, 10, e0129791. [Google Scholar] [CrossRef] [Green Version]
- Jia, G.; Hill, M.A.; Sowers, J.R. Diabetic Cardiomyopathy. An Update of Mechanisms Contributing to This Clinical Entity. Circ. Res. 2018, 122, 624–638. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Struck, J.; Alonso, C.; Bergmann, A. Assay for the measurement of copeptin, a stable peptide derived from the precursor of vasopressin. Clin. Chem. 2006, 52, 112. [Google Scholar] [CrossRef] [Green Version]
- Enhörning, S.; Bo Hedblad, B.; Nilsson, P.M.; Engstrom, G. Copeptin is an independent predictor of diabetic heart disease and death. Am. Heart J. 2015, 169, 549–556. [Google Scholar] [CrossRef]
- Enhörning, S.; Wang, T.J.; Nilsson, P.M.; Almgren, P.; Hedblad, B.; Berglund, G. Plasma copeptin and the risk of diabetes mellitus. Circulation 2010, 121, 2102–2108. [Google Scholar] [CrossRef] [Green Version]
- Enhörning, S.; Bankir, L.; Bouby, N.; Struck, J.; Hedblad, B.; Persson, M.; Morgenthaler, N.G. Copeptin, a marker of vasopressin, in abdominal obesity, diabetes and microalbuminuria: The prospective Malmö Diet and Cancer Study cardiovascular cohort. Int. J. Obes. 2013, 37, 598–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mant, J.; Doust, J.; Roalfe, A.; Barton, P.; Cowie, M.R.; Glasziou, P.; Mant, D. Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care. Health Technol. Assess. 2009, 13, 1–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A simple, evidence-based approach to help guide diagnosis of heart failure with preserved ejection fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Kane, G.C.; Reddy, Y.N.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure with Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation 2017, 135, 825–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, R.T.; Jhund, P.S.; Castagno, D.; Hawkins, N.M.; Petrie, M.C.; McMurray, J.J. What have we learned about patients with heart failure and preserved ejection fraction from DIG-PEF, CHARM-preserved, and I-PRESERVE? J. Am. Coll. Cardiol. 2012, 60, 2349–2356. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.M.; Claggett, B.; Sweitzer, N.K.; Shah, S.J.; Anand, I.S.; O’Meara, E.; Desai, A.S.; Heitner, J.F.; Li, G.; Fang, J.; et al. Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: Findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure Aldosterone Antagonist (TOPCAT) Trial. Circ. Heart Fail. 2014, 5, 740–751. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Chhor, M.; Rayner, B.; McGrath, K. Diagnostics and prognostic potential of current biomarkers in heart failure with preserved ejection fraction: A systematic review and meta-analysis. medRxiv 2020, 4, 18. [Google Scholar] [CrossRef]
- Lee, Y.; Lim, S.; Hong, E.S.; Kim, J.H.; Moon, M.K.; Chun, E.J. Serum FGF21 concentration is associated with hypertriglyceridemia, hyperinsulinemia and pericardial fat accumulation, independently of obesity, but not with current coronary artery status. Clin. Endocrinol. 2014, 80, 57–64. [Google Scholar] [CrossRef]
- Zhang, R.; Cai, X.; Du, Y.; Liu, L.; Han, X.; Liu, W.; Gong, S.; Zhou, X.; Wang, X. Association of serum fibroblast growth factor 21 and urinary glucose excretion in hospitalized patients with type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107750. [Google Scholar] [CrossRef]
- Kharitonenkov, A.; Shiyanova, T.L.; Koester, A.; Ford, A.M.; Micanovic, R.; Galbreath, E.J.; Sandusky, G.E.; Hammond, L.J.; Moyers, J.S. FGF21 as a novel metabolic regulator. J. Clin. Investig. 2005, 115, 1627–1635. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Wu, G.; Fang, Q.; Zhang, M.; Hui, X.; Sheng, B.; Wu, L.; Bao, Y.; Li, P.; Xu, A. Fibroblast growth factor 21 increases insulin sensitivity through specific expansion of subcutaneous fat. Nat. Commun. 2018, 9, 272. [Google Scholar] [CrossRef] [Green Version]
- Han, M.M.; Wang, W.F.; Liu, M.Y.; Li, D.S.; Zhou, B.; Yu, Y.H. FGF21 protects H9c2 cardiomyoblasts against hydrogen peroxide-induced oxidative stress injury. Yao Xue Xue Bao 2014, 49, 470–475. [Google Scholar]
- Mäkelä, J.; Tselykh, T.V.; Maiorana, F.; Eriksson, O.; Do, H.T.; Mudò, G.; Korhonen, L.T.; Belluardo, N.; Lindholm, D. Fibroblast growth factor-21 enhances mitochondrial functions and increases the activity of PGC-1α in human dopaminergic neurons via Sirtuin-1. Springerplus 2014, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Van Kimmenade, R.R.; Januzzi, J.L.; Ellinor, P.T.; Sharma, U.C.; Bakker, J.A. Utility of amino-terminal pro-brain natriuretic peptide, galectin-3, and apelin for the evaluation of patients with acute heart failure. J. Am. Coll. Cardiol. 2006, 48, 1217–1224. [Google Scholar] [CrossRef] [Green Version]
- Trippel, T.D.; Mende, M.; Düngen, H.D.; Hashemi, D.; Petutschnigg, J.; Nolte, K.; Herrmann-Lingen, C. The diagnostic and prognostic value of galectin-3 in patients at risk for heart failure with preserved ejection fraction: Results from the DIAST-CHF study. ESC Heart Fail. 2021, 8, 829–841. [Google Scholar] [CrossRef] [PubMed]
- De Boer, R.A.; Lok, D.J.; Jaarsma, T.; van der Meer, P.; Voors, A.A.; Hillege, H.L.; van Veldhuisen, D.J. Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction. Ann. Med. 2011, 43, 60–68. [Google Scholar] [CrossRef]
- Cui, Y.; Qi, X.; Huang, A.; Li, J.; Hou, W.; Liu, K. Differential and Predictive Value of Galectin-3 and Soluble Suppression of Tumorigenicity-2 (sST2) in Heart Failure with Preserved Ejection Fraction. Med. Sci. Monit. 2018, 24, 5139–5146. [Google Scholar] [CrossRef] [PubMed]
- Yin, Q.S.; Shi, B.; Dong, L.; Bi, L. Comparative study of galectin-3 and B-type natriuretic peptide as biomarkers for the diagnosis of heart failure. J. Geriatr. Cardiol. 2014, 11, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Gurel, O.; Yilmaz, H. Galectin-3 as a new biomarker of diastolic dysfunction in hemodialysis patients. Herz 2015, 40, 788–794. [Google Scholar] [CrossRef]
- Hussain, S.; Habib, A.; Hussain, M.S.; Najmi, A.K. Potential biomarkers for early detection of diabetic kidney disease. Diabetes Res. Clin. Pract. 2020, 161, 1–9. [Google Scholar] [CrossRef]
- Jin, Q.H.; Lou, Y.F.; Li, T.L.; Chen, H.H.; Liu, Q.; He, X.J. Serum galectin-3: A risk factor for vascular complications in type 2 diabetes mellitus. Chin. Med. J. 2013, 126, 2109–2115. [Google Scholar]
- Edelmann, F.; Holzendorf, V.; Wachter, R.; Nolte, K.; Schmidt, A.G.; Kraigher-Krainer, E.; Duvinage, A.; Unkelbach, I.; Düngen, H.D.; Tschöpe, C. Galectin-3 in patients with heart failure with preserved ejection fraction: Results from the Aldo-DHF trial. Eur. J. Heart Fail. 2015, 17, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Pecherina, T.; Kutikhin, A.; Kashtalap, V.; Karetnikova, V.; Gruzdeva, O.; Hryachkova, O.; Barbarash, O. Serum and Echocardiographic Markers May Synergistically Predict Adverse Cardiac Remodeling after ST-Segment Elevation Myocardial Infarction in Patients with Preserved Ejection Fraction. Diagnostics 2020, 10, 301. [Google Scholar] [CrossRef] [PubMed]
- De Marco, C.; Claggett, B.L.; de Denus, S.; Zile, M.R.; Huynh, T.; Desai, A.S.; Sirois, M.G.; Solomon, S.D.; Pitt, B. Impact of diabetes on serum biomarkers in heart failure with preserved ejection fraction: Insights from the TOPCAT trial. ESC Heart Fail. 2021, 8, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Schill, F.; Timpka, S.; Nilsson, P.M.; Melander, O.; Enhörning, S. Copeptin as a predictive marker of incident heart failure. ESC Heart Fail. 2021, 8, 3180–3188. [Google Scholar] [CrossRef]
- Noor, T.; Hanif, F.; Kiran, Z.; Rehman, R.; Khan, M.T.; Haque, Z.; Nankani, K. Relation of Copeptin with Diabetic and Renal Function Markers Among Patients with Diabetes Mellitus Progressing Towards Diabetic Nephropathy. Arch. Med. Res. 2020, 51, 548–555. [Google Scholar] [CrossRef]
- Xu, L.; Liu, X.; Wu, S.; Gai, L. The clinical application value of the plasma copeptin level in the assessment of heart failure with reduced left ventricular ejection fraction a cross-sectional study. Medicine 2018, 97, e12610. [Google Scholar] [CrossRef]
- Stoiser, B.; Mörtl, D.; Hülsmann, M.; Berger, R.; Struck, J.; Morgenthaler, N.G.; Bergmann, A.; Pacher, R. Copeptin, a fragment of the vasopressin precursor, as a novel predictor of outcome in heart failure. Eur. J. Clin. Investig. 2006, 36, 771–778. [Google Scholar] [CrossRef]
- Maisel, A.; Xue, Y.; Shah, K.; Mueller, C.; Nowak, R.; Peacock, W.F.; Ponikowski, P.; Mockel, M.; Hogan, C. Increased 90-day mortality in patients with acute heart failure with elevated copeptin: Secondary results from the Biomarkers in Acute Heart Failure (BACH) study. Circ. Heart Fail. 2011, 4, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Pazin-Filho, A.; Kottgen, A.; Bertoni, A.G.; Russell, S.D.; Selvin, E.; Rosamond, W.D.; Coresh, J. HbA1c as a risk factor for heart failure in persons with diabetes: The Atherosclerosis Risk in Communities (ARIC) study. Diabetologia 2008, 51, 2197–2204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, W.; Katzmarzyk, P.T.; Horswell, R.; Wang, Y.; Johnson, J.; Hu, G. HbA1c and heart failure risk among diabetic patients. J. Clin. Endocrinol. Metab. 2014, 99, E263–E267. [Google Scholar] [CrossRef] [Green Version]
- Lind, M.; Olsson, M.; Rosengren, A.; Svensson, A.M.; Bounias, I.; Gudbjörnsdottir, S. The relationship between glycaemic control and heart failure in 83,021 patients with type 2 diabetes. Diabetologia 2012, 55, 2946–2953. [Google Scholar] [CrossRef] [Green Version]
- Erqou, S.; Lee, C.T.; Suffoletto, M.; Echouffo-Tcheugui, J.B.; de Boer, R.A.; van Melle, J.P.; Adler, A.I. Association between glycated haemoglobin and the risk of congestive heart failure in diabetes mellitus: Systematic review and meta-analysis. Eur. J. Heart Fail. 2013, 15, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Iribarren, C.; Karter, A.J.; Go, A.S.; Ferrara, A.; Liu, J.Y.; Sidney, S.; Selby, J.V. Glycemic Control and Heart Failure Among Adult Patients with Diabetes. Circulation 2001, 103, 2668–2673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, L.; Lam, K.S.L.; Xu, A. The therapeutic potential of FGF21 in metabolic diseases: From bench to clinic. Nat. Rev. Endocrinol. 2020, 16, 654–667. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All DM Samples (n = 69) | DM without HFpEF (n1 = 29) | DM with HFpEF (n2 = 40) | p-Value | |
|---|---|---|---|---|
| Age, years (a) | 64.65 ± 9.83 | 63.83 ± 7.70 | 65.25 ± 11.17 | 0.557 |
| Male (b) | 37 (53.62) | 18 (62.07) | 19 (47.50) | 0.231 |
| Body mass index, kg/m2 (a) | 32.43 ± 6.69 | 30.94 ± 7.25 | 33.50 ± 6.11 | 0.117 |
| Body Surface Area (a) | 1.99 ± 0.21 | 2.00 ± 0.24 | 1.99 ± 0.18 | 0.866 |
| SBP, mmHg (a) | 138.40 ± 19.68 | 136.60 ± 18.57 | 139.70 ± 20.59 | 0.519 |
| DBP, mmHg (a) | 79.67 ± 10.96 | 77.45 ± 10.20 | 81.28 ± 11.33 | 0.153 |
| Smoking (b) | 15 (21.74) | 8 (27.59) | 7 (17.50) | 0.316 |
| Medical history (b) | ||||
| Hypertension | 60 (86.96) | 27 (93.10) | 33 (82.50) | 0.285 |
| Atrial fibrillation | 9 (13.04) | 1 (3.45) | 8 (20.00) | 0.069 |
| Paroxysmal atrial fibrillation | 3 (4.35) | 0 (0.00) | 3 (7.50) | 0.258 |
| Previous stroke | 2 (2.90) | 0 (0.00) | 2 (5.00) | 0.506 |
| Previous MI | 32 (46.38) | 10 (34.48) | 22 (55.00) | 0.092 |
| COPD | 3 (5.80) | 1 (3.45) | 3 (7.69) | 0.631 |
| PAD | 5 (7.25) | 5 (17.86) | 0 (0.0) | 0.009 |
| Medication (b) | 0.765 | |||
| Insulin | 30 (43.48) | 12 (41.38) | 18 (45.00) | |
| Oral antidiabetic drugs (b) | 39 (56.52) | 17 (58.62) | 22 (55.00) | |
| Laboratory data (a) | ||||
| HbA1C, % | 7.65 [7.20, 9.25] | 7.42 [6.90, 7.69] | 8.84 [7.30, 9.96] | 0.008 * |
| Fasting blood glucose, mg/dL | 187.50 ± 74.12 | 171.50 ± 58.59 | 199.10 ± 82.38 | 0.128 |
| Total cholesterol, mg/dL | 166.60 ± 46.16 | 156.60 ± 41.67 | 173.80 ± 48.37 | 0.127 |
| LDL cholesterol, mg/dL | 93.66 ± 38.42 | 88.13 ± 38.97 | 97.66 ± 38.01 | 0.313 |
| HDL cholesterol, mg/dL | 38.74 ± 9.19 | 37.32 ± 8.44 | 39.77 ± 9.68 | 0.277 |
| Triglycerides, mg/dL | 155.20 [112.40, 204.00] | 156.40 [124.00, 181.10] | 150.50 [107.20, 224.00] | 0.918 |
| eGFR, mL/min/1.73 m2 by CKD-EPI | 73.69 ± 24.49 | 78.07 ± 21.70 | 70.53 ± 26.14 | 0.209 |
| Hemoglobin, g/dL | 13.38 ± 1.71 | 13.73 ± 1.76 | 13.13 ± 1.65 | 0.152 |
| Uric acid mg/dL | 6.36 ± 1.88 | 5.92 ± 1.06 | 6.68 ± 2.26 | 0.070 |
| Coronary angiography #, (b) | 0.031 * | |||
| Absent | 4 (5.80) | 4 (16.00) | 0 (0.00) | |
| Monovessel CAD | 15 (21.74) | 4 (16.00) | 11 (32.35) | |
| Multivessel CAD | 40 (57.97) | 17 (68.00) | 23 (67.65) |
| All DM Samples (n = 69) | DM without HFpEF (n1 = 29) | DM with HFpEF (n2 = 40) | p-Value | |
|---|---|---|---|---|
| FGF21, pg/mL (a) | 221.72 ± 2.01 | 146.79 ± 1.76 | 298.98 ± 1.90 | <0.001 *,(d) |
| Gal-3, ng/mL (b) | 11.91 ± 1.52 | 11.66 ± 1.71 | 12.10 ± 1.36 | 0.239 |
| Copeptin, pg/mL (a) | 321.04 ± 2.55 | 348.35 ± 2.84 | 302.59 ± 2.36 | 0.541 (d) |
| LV ejection fraction, % (b) | 54 [51, 59] | 57 [54, 61] | 53 [50, 55] | 0.001 * |
| LV EDV, ml (c) | 108 [90, 126] | 103 [89, 112] | 116 [94.25, 138.20] | 0.061 |
| LV ESV, ml (b) | 50.4 ± 20.6 | 43.4 ± 17.2 | 55.5 ± 21.6 | 0.014 * |
| LVDd, mm (b) | 49.8 ± 5.1 | 50.3 ± 4.6 | 49.5 ± 5.5 | 0.539 |
| LVSd, mm (b) | 29.0 ± 6.4 | 28.3 ± 6.2 | 29.6 ± 6.6 | 0.425 |
| IVST, mm (b) | 12.3 ± 1.7 | 12.2 ± 1.7 | 12.3 ± 1.6 | 0.886 |
| PWT, mm (b) | 12.0 ± 1.6 | 11.8 ± 1.8 | 12.1 ± 1.5 | 0.355 |
| LA volume index, mL/m2 (c) | 30.0 [25.6, 35.0] | 27.3 [24.0, 29.8] | 32.31 [28.1, 41.3] | 0.001 * |
| LA surface, cm2 (b) | 22.9 ± 6.8 | 19.3 ± 4.3 | 25.5 ± 7.2 | <0.001 * |
| E wave velocity, m/s (b) | 0.8 ± 0.3 | 0.7 ± 0.2 | 0.9 ± 0.3 | 0.002 * |
| A wave velocity, m/s (b) | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.9 ± 0.2 | 0.111 |
| Mitral E/A ratio (b) | 0.9 ± 0.3 | 0.9 ± 0.4 | 0.9 ± 0.3 | 0.722 |
| TDE, msec (b) | 217.8 ± 39.9 | 230.8 ± 33.5 | 208.4 ± 41.9 | 0.020 * |
| Septal e’ velocity, cm/s (b) | 7.2 ± 1.4 | 7.9 ± 1.3 | 6.7 ± 1.2 | <0.001 * |
| Lateral e’ velocity, cm/s (b) | 8.6 ± 1.9 | 9.8 ± 1.5 | 7.7 ± 1.6 | <0.001 * |
| E/e’ mean ratio (b) | 10.7 ± 3.9 | 8.2 ± 2.5 | 12.37 ± 3.9 | <0.001 * |
| Relative wall thickness (b) | 0.48 ± 0.1 | 0.46 ± 0.06 | 0.49 ± 0.08 | 0.058 |
| TR velocity, m/s (b) | 2.4 ± 0.6 | 2.06 ± 0.42 | 2.69 ± 0.61 | <0.001 * |
| PASP, mmHg (b) | 30.6 ± 15.6 | 21.7 ± 7.9 | 37.1 ± 16.6 | <0.001 * |
| Variables | Univariable Model | p-Value | Multivariable Model | p-Value |
|---|---|---|---|---|
| Crude OR [95% CI] | Adjusted OR [95% CI] | |||
| FGF21 (pg/mL) | 5.16 [2.19, 15.47] | 0.001 * | 8.80 [2.95, 36.30] | 0.001 * |
| Age (years) | 1.16 [0.71, 1.90] | 0.551 | 2.52 [1.12; 6.68] | 0.039 * |
| Gender (a) | 0.55 [0.20, 1.45] | 0.233 | 0.67 [0.16, 2.72] | 0.574 |
| BMI (kg/m2) | 1.50 [0.91, 2.55] | 0.118 | 0.69 [0.31, 1.44] | 0.340 |
| DBP (mmHG) | 1.45 [0.88, 2.50] | 0.157 | 1.20 [0.64, 2.38] | 0.573 |
| HbA1c (%) | 1.99 [1.14, 3.93] | 0.0267 * | 2.27 [1.19, 5.13] | 0.025 * |
| Previous MI | 2.32 [0.88, 6.40] | 0.094 | 3.81 [0.99, 17.19] | 0.061 |
| Variables | Log FGF21 | Log Copeptin | Gal-3 |
|---|---|---|---|
| Correlation Coefficient (95% CI) | Correlation Coefficient (95% CI) | Correlation Coefficient (95% CI) | |
| LV EF, % | −0.26 [−0.47, 0.02] (b) | 0.20 [−0.05, 0.42] (b) | −0.14 [−0.37, 0.11] (b) |
| LV EDV, ml | 0.32 [0.08, 0.52] (b),* | −0.30 [−0.50, −0.06] (b),* | 0.21 [−0.03, 0.43] (b) |
| LV ESV, ml | 0.39 [0.17, 0.57] (a),* | −0.31 [−0.51, −0.08] (a),* | 0.20 [−0.04, 0.42] (a) |
| LA volume index, mL/m2 | 0.29 [0.05, 0.49] (b),* | −0.09 [−0.33, 0.15] (b) | 0.25 [0.01, 0.47] (b),* |
| LA surface, cm2 | 0.26 [0.03, 0.47] (a),* | −0.05 [−0.29, 0.19] (a) | 0.12 [−0.12, 0.34] (a) |
| E wave velocity, m/s | 0.20 [−0.04, 0.41] (a) | 0.25 [0.02, 0.46] (a),* | 0.03 [−0.20, 0.27] (a) |
| A wave velocity, m/s | −0.01 [−0.26, 0.24] (a) | 0.11 [−0.14, 0.35] (a) | 0.01 [−0.23, 0.26] (a) |
| Mitral E/A ratio | 0.19 [−0.06, 0.42] (a) | 0.25 [0.00, 0.47] (a) | <0.01 [−0.25, 0.24] (a) |
| TDE, msec | −0.16 [−0.38, 0.08] (a) | −0.12 [−0.35, 0.12] (a) | <0.01 [−0.23, 0.24] (a) |
| Septal e’ velocity, cm/s | −0.19 [−0.41, 0.05] (a) | −0.03 [−0.27, 0.21] (a) | −0.07 [−0.30, 0.17] (a) |
| Lateral e’ velocity, cm/s | −0.21 [−0.42, 0.03] (a) | −0.01 [−0.25, 0.23] (a) | 0.03 [−0.21, 0.26] (a) |
| E/e’ mean ratio | 0.23 [−0.01, 0.44] (a) | 0.24 [0.00, 0.45] (a) | 0.06 [−0.18, 0.29] (a) |
| Relative wall thickness | 0.09 [−0.15, 0.32] (a) | 0.28 [0.04, 0.48] (a),* | 0.20 [−0.04, 0.41] (a) |
| TR velocity, m/s | 0.25 [0.02, 0.46] (a) | −0.17 [0.40, 0.06] (a) | 0.25 [0.02, 0.46] (a),* |
| PASP, mmHg | 0.26 [0.03, 0.47] (a),* | −0.16 [−0.38, 0.08] (a) | 0.27 [0.03, 0.48] (a),* |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ianoș, R.D.; Pop, C.; Iancu, M.; Rahaian, R.; Cozma, A.; Procopciuc, L.M. Diagnostic Performance of Serum Biomarkers Fibroblast Growth Factor 21, Galectin-3 and Copeptin for Heart Failure with Preserved Ejection Fraction in a Sample of Patients with Type 2 Diabetes Mellitus. Diagnostics 2021, 11, 1577. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091577
Ianoș RD, Pop C, Iancu M, Rahaian R, Cozma A, Procopciuc LM. Diagnostic Performance of Serum Biomarkers Fibroblast Growth Factor 21, Galectin-3 and Copeptin for Heart Failure with Preserved Ejection Fraction in a Sample of Patients with Type 2 Diabetes Mellitus. Diagnostics. 2021; 11(9):1577. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091577
Chicago/Turabian StyleIanoș, Raluca D., Călin Pop, Mihaela Iancu, Rodica Rahaian, Angela Cozma, and Lucia M. Procopciuc. 2021. "Diagnostic Performance of Serum Biomarkers Fibroblast Growth Factor 21, Galectin-3 and Copeptin for Heart Failure with Preserved Ejection Fraction in a Sample of Patients with Type 2 Diabetes Mellitus" Diagnostics 11, no. 9: 1577. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091577