
Coronary Calcium Scoring with First Generation Dual-Source Photon-Counting CT—First Evidence from Phantom and In-Vivo Scans


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Phantom Study
2.2.1. Anthropomorphic Phantom
2.2.2. Phantom Scan Acquisition
2.2.3. Scan Reconstruction
2.2.4. Reference
2.3. Patient Scans
2.4. Coronary Artery Calcium Scoring
2.5. Statistical Analysis
3. Results
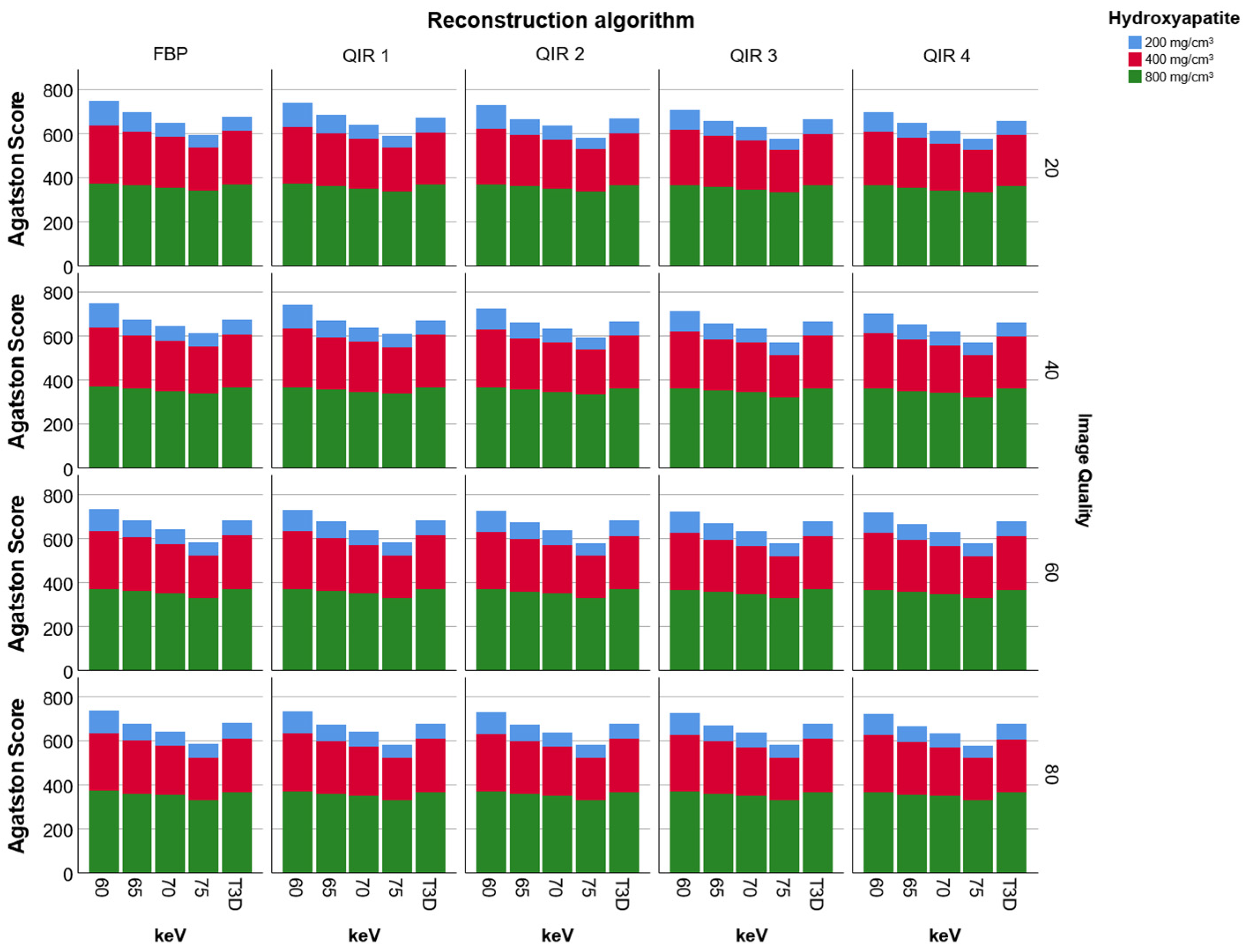
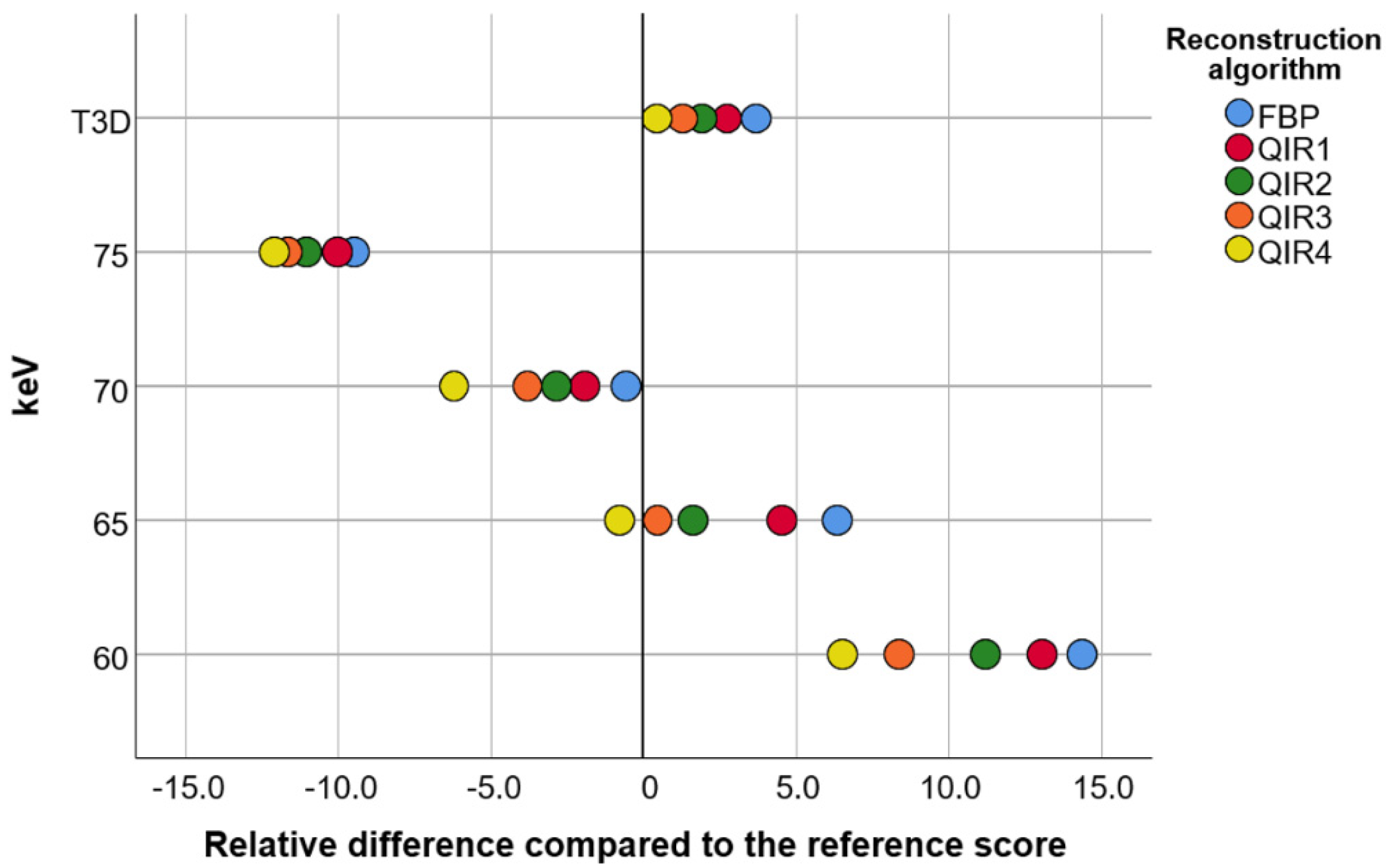
3.1. Phantom Study
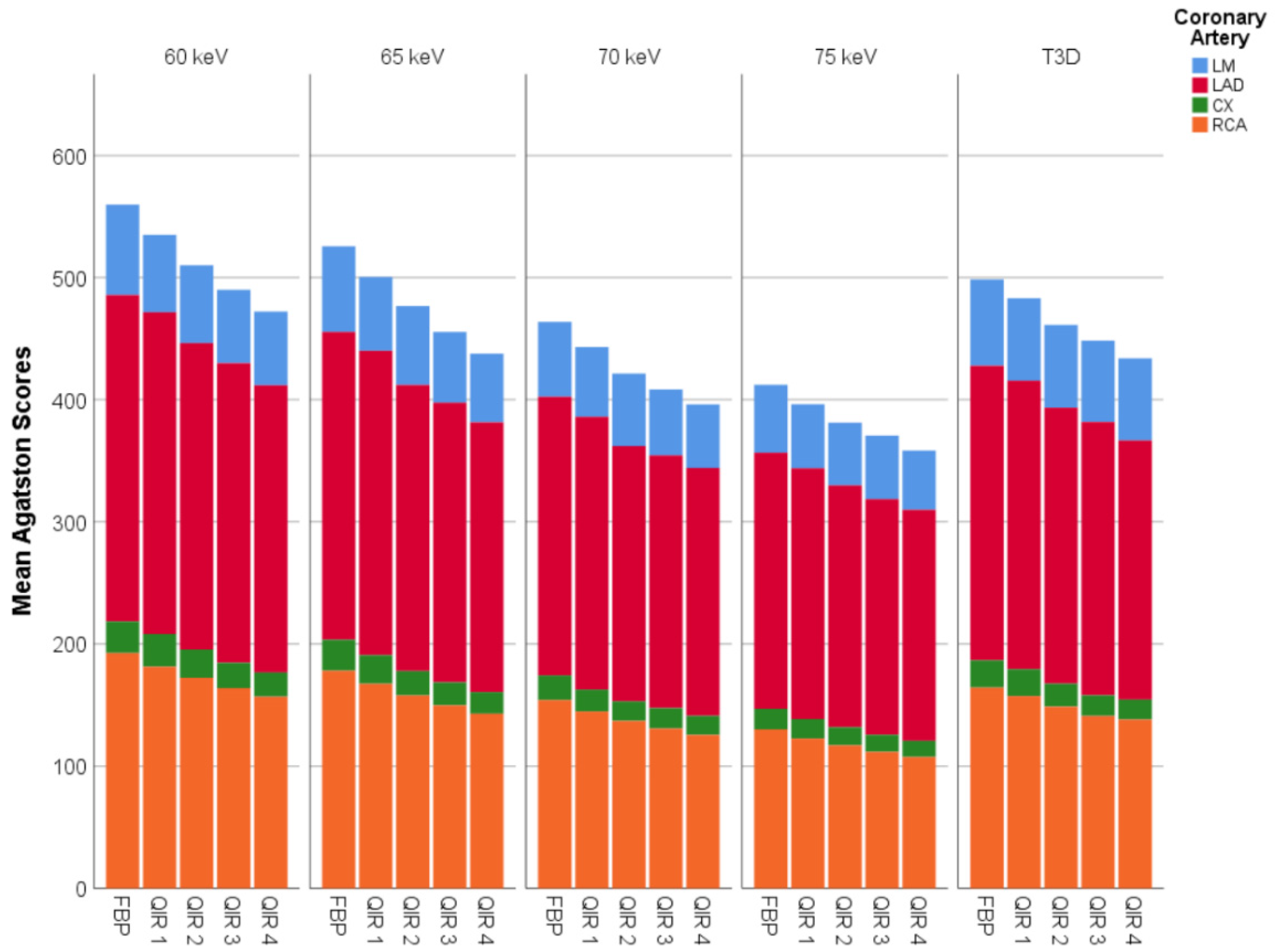
3.2. Patient Study
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Grandhi, G.R.; Mirbolouk, M.; Dardari, Z.A.; Al-Mallah, M.H.; Rumberger, J.A.; Shaw, L.J.; Blankstein, R.; Miedema, M.D.; Berman, D.S.; Budoff, M.J.; et al. Interplay of Coronary Artery Calcium and Risk Factors for Predicting CVD/CHD Mortality: The CAC Consortium. JACC Cardiovasc. Imaging 2020, 13, 1175–1186. [Google Scholar] [CrossRef]
- Writing, G.; Slim, A.M.; Fentanes, E.; Cheezum, M.K.; Parsons, I.T.; Maroules, C.; Chen, B.; Abbara, S.; Branch, K.; Nagpal, P.; et al. The role of cardiovascular CT in occupational health assessment for coronary heart disease: An expert consensus document from the Society of Cardiovascular Computed Tomography (SCCT). J. Cardiovasc. Comput. Tomogr. 2021. [Google Scholar] [CrossRef]
- Vancheri, F.; Longo, G.; Vancheri, S.; Danial, J.S.H.; Henein, M.Y. Coronary Artery Microcalcification: Imaging and Clinical Implications. Diagnostics 2019, 9, 125. [Google Scholar] [CrossRef] [Green Version]
- Blaha, M.J.; Whelton, S.P.; Al Rifai, M.; Dardari, Z.; Shaw, L.J.; Al-Mallah, M.H.; Matsushita, K.; Rozanski, A.; Rumberger, J.A.; Berman, D.S.; et al. Comparing Risk Scores in the Prediction of Coronary and Cardiovascular Deaths: Coronary Artery Calcium Consortium. JACC Cardiovasc. Imaging 2021, 14, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Elias-Smale, S.E.; Proenca, R.V.; Koller, M.T.; Kavousi, M.; van Rooij, F.J.; Hunink, M.G.; Steyerberg, E.W.; Hofman, A.; Oudkerk, M.; Witteman, J.C. Coronary calcium score improves classification of coronary heart disease risk in the elderly: The Rotterdam study. J. Am. Coll. Cardiol. 2010, 56, 1407–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eberhard, M.; Hinzpeter, R.; Schonenberger, A.L.N.; Euler, A.; Kuzo, N.; Reeve, K.; Stahli, B.E.; Kasel, A.M.; Manka, R.; Tanner, F.C.; et al. Incremental Prognostic Value of Coronary Artery Calcium Score for Predicting All-Cause Mortality after Transcatheter Aortic Valve Replacement. Radiology 2021. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Sandfort, V.; Bluemke, D.A. CT calcium scoring. History, current status and outlook. Diagn. Interv. Imaging 2017, 98, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hecht, H.S.; Blaha, M.J.; Kazerooni, E.A.; Cury, R.C.; Budoff, M.; Leipsic, J.; Shaw, L. CAC-DRS: Coronary Artery Calcium Data and Reporting System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT). J. Cardiovasc. Comput. Tomogr. 2018, 12, 185–191. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Ulzheimer, S.; Halliburton, S.S.; Shanneik, K.; White, R.D.; Kalender, W.A. Coronary artery calcium: A multi-institutional, multimanufacturer international standard for quantification at cardiac CT. Radiology 2007, 243, 527–538. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Sartoretti, T.; Eberhard, M.; Nowak, T.; Gutjahr, R.; Jost, G.; Pietsch, H.; Schmidt, B.; Flohr, T.; Alkadhi, H.; Euler, A. Photon-Counting Multienergy Computed Tomography With Spectrally Optimized Contrast Media for Plaque Removal and Stenosis Assessment. Investig. Radiol. 2021, 56, 563–570. [Google Scholar] [CrossRef]
- Wetzl, M.; Wenkel, E.; Balbach, E.; Dethlefsen, E.; Hartmann, A.; Emons, J.; Kuhl, C.; Beckmann, M.W.; Uder, M.; Ohlmeyer, S. Detection of Microcalcifications in Spiral Breast Computed Tomography with Photon-Counting Detector Is Feasible: A Specimen Study. Diagnostics 2021, 11, 848. [Google Scholar] [CrossRef]
- Sandstedt, M.; Marsh, J., Jr.; Rajendran, K.; Gong, H.; Tao, S.; Persson, A.; Leng, S.; McCollough, C. Improved coronary calcification quantification using photon-counting-detector CT: An ex vivo study in cadaveric specimens. Eur. Radiol. 2021. [Google Scholar] [CrossRef]
- Eberhard, M.; Hinzpeter, R.; Polacin, M.; Morsbach, F.; Maisano, F.; Nietlispach, F.; Nguyen-Kim, T.D.L.; Tanner, F.C.; Alkadhi, H. Reproducibility of aortic valve calcification scoring with computed tomography—An interplatform analysis. J. Cardiovasc. Comput. Tomogr. 2019, 13, 92–98. [Google Scholar] [CrossRef]
- Hausleiter, J.; Meyer, T.; Hermann, F.; Hadamitzky, M.; Krebs, M.; Gerber, T.C.; McCollough, C.; Martinoff, S.; Kastrati, A.; Schomig, A.; et al. Estimated radiation dose associated with cardiac CT angiography. JAMA 2009, 301, 500–507. [Google Scholar] [CrossRef]
- Singh, G.; Al’Aref, S.J.; Lee, B.C.; Lee, J.K.; Tan, S.Y.; Lin, F.Y.; Chang, H.J.; Shaw, L.J.; Baskaran, L.; On Behalf Of The, C.; et al. End-to-End, Pixel-Wise Vessel-Specific Coronary and Aortic Calcium Detection and Scoring Using Deep Learning. Diagnostics 2021, 11, 215. [Google Scholar] [CrossRef] [PubMed]
- Tao, S.; Sheedy, E.; Bruesewitz, M.; Weber, N.; Williams, K.; Halaweish, A.; Schmidt, B.; Williamson, E.; McCollough, C.; Leng, S. Technical Note: kV-independent coronary calcium scoring: A phantom evaluation of score accuracy and potential radiation dose reduction. Med. Phys. 2021, 48, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Vingiani, V.; Abadia, A.F.; Schoepf, U.J.; Fischer, A.M.; Varga-Szemes, A.; Sahbaee, P.; Allmendinger, T.; Tesche, C.; Griffith, L.P.; Marano, R.; et al. Low-kV coronary artery calcium scoring with tin filtration using a kV-independent reconstruction algorithm. J. Cardiovasc. Comput. Tomogr. 2020, 14, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Tesche, C.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; Caruso, D.; Varga-Szemes, A.; Lesslie, V.W.; Ebersberger, U.; Canstein, C.; et al. Iterative beam-hardening correction with advanced modeled iterative reconstruction in low voltage CT coronary calcium scoring with tin filtration: Impact on coronary artery calcium quantification and image quality. J. Cardiovasc. Comput. Tomogr. 2017, 11, 354–359. [Google Scholar] [CrossRef]
- Hinzpeter, R.; Weber, L.; Euler, A.; Kasel, A.M.; Tanner, F.C.; Alkadhi, H.; Eberhard, M. Aortic valve calcification scoring with computed tomography: Impact of iterative reconstruction techniques. Int. J. Cardiovasc. Imaging 2020, 36, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- den Harder, A.M.; Wolterink, J.M.; Willemink, M.J.; Schilham, A.M.R.; de Jong, P.A.; Budde, R.P.J.; Nathoe, H.M.; Isgum, I.; Leiner, T. Submillisievert coronary calcium quantification using model-based iterative reconstruction: A within-patient analysis. Eur. J. Radiol. 2016, 85, 2152–2159. [Google Scholar] [CrossRef] [PubMed]
- Szilveszter, B.; Elzomor, H.; Karolyi, M.; Kolossvary, M.; Raaijmakers, R.; Benke, K.; Celeng, C.; Bartykowszki, A.; Bagyura, Z.; Lux, A.; et al. The effect of iterative model reconstruction on coronary artery calcium quantification. Int. J. Cardiovasc. Imaging 2016, 32, 153–160. [Google Scholar] [CrossRef]
- Symons, R.; Sandfort, V.; Mallek, M.; Ulzheimer, S.; Pourmorteza, A. Coronary artery calcium scoring with photon-counting CT: First in vivo human experience. Int. J. Cardiovasc. Imaging 2019, 35, 733–739. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient and Scan Characteristics (n = 20) | |
|---|---|
| Females | n = 12 (60%) |
| Age (years) | 69 ± 12 |
| Height (cm) | 168 ± 12 |
| Weight (kg) | 76 ± 17 |
| Body mass index (kg/m2) | 27.0 ± 4.7 |
| Tube current time product (mAs) | 18 ± 6 |
| Volume CT dose index (mGy) | 3.3 ± 1.3 |
| Dose length product (mGy × cm) | 48 ± 19 |
| Effective dose * (mSv) | 0.67 ± 0.26 |
| VMI/T3D | FBP/no QIR | QIR 1 | QIR 2 | QIR 3 | QIR 4 |
|---|---|---|---|---|---|
| 60 keV | 107 (48–1060) | 100 (44–1026) | 91 (40–999) | 86 (36–974) | 80 (33–952) |
| 65 keV | 105 (44–1024) | 98 (40–989) | 90 (36–957) | 82 (33–930) | 74 (30–896) |
| 70 keV | 86 (38–978) | 76 (35–939) | 65 (31–886) | 64 (27–877) | 59 (24–850) |
| 75 keV | 64 (29–895) | 59 (26–867) | 56 (23–839) | 53 (21–819) | 49 (20–803) |
| T3D | 101 (46–1035) | 95 (43–1013) | 86 (39–981) | 80 (37–959) | 76 (34–934) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eberhard, M.; Mergen, V.; Higashigaito, K.; Allmendinger, T.; Manka, R.; Flohr, T.; Schmidt, B.; Euler, A.; Alkadhi, H. Coronary Calcium Scoring with First Generation Dual-Source Photon-Counting CT—First Evidence from Phantom and In-Vivo Scans. Diagnostics 2021, 11, 1708. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091708
Eberhard M, Mergen V, Higashigaito K, Allmendinger T, Manka R, Flohr T, Schmidt B, Euler A, Alkadhi H. Coronary Calcium Scoring with First Generation Dual-Source Photon-Counting CT—First Evidence from Phantom and In-Vivo Scans. Diagnostics. 2021; 11(9):1708. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091708
Chicago/Turabian StyleEberhard, Matthias, Victor Mergen, Kai Higashigaito, Thomas Allmendinger, Robert Manka, Thomas Flohr, Bernhard Schmidt, Andre Euler, and Hatem Alkadhi. 2021. "Coronary Calcium Scoring with First Generation Dual-Source Photon-Counting CT—First Evidence from Phantom and In-Vivo Scans" Diagnostics 11, no. 9: 1708. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091708