
Prediction of Bacteremia Based on 12-Year Medical Data Using a Machine Learning Approach: Effect of Medical Data by Extraction Time

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
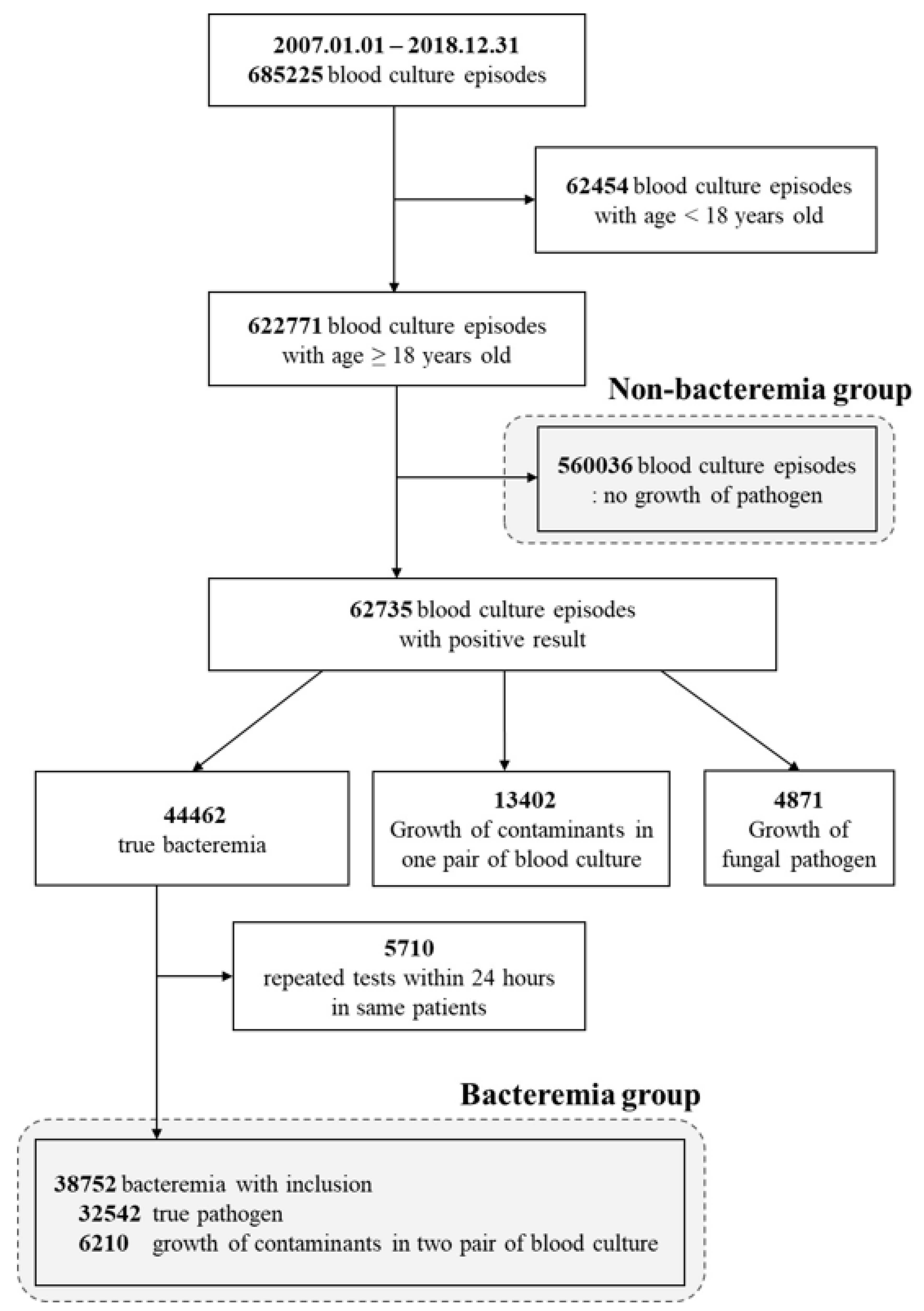
2.1. Study Population
2.2. Data Extraction
2.3. Definition of Bacteremia
2.4. Clinical Variables
2.5. Subgroup Analysis
2.6. Machine Learning Technique and Statistical Analysis
2.7. Ethics Approval and Consent to Participate
3. Results
3.1. Comprehensive Analysis
3.2. Influence Ranking of Clinical Variables
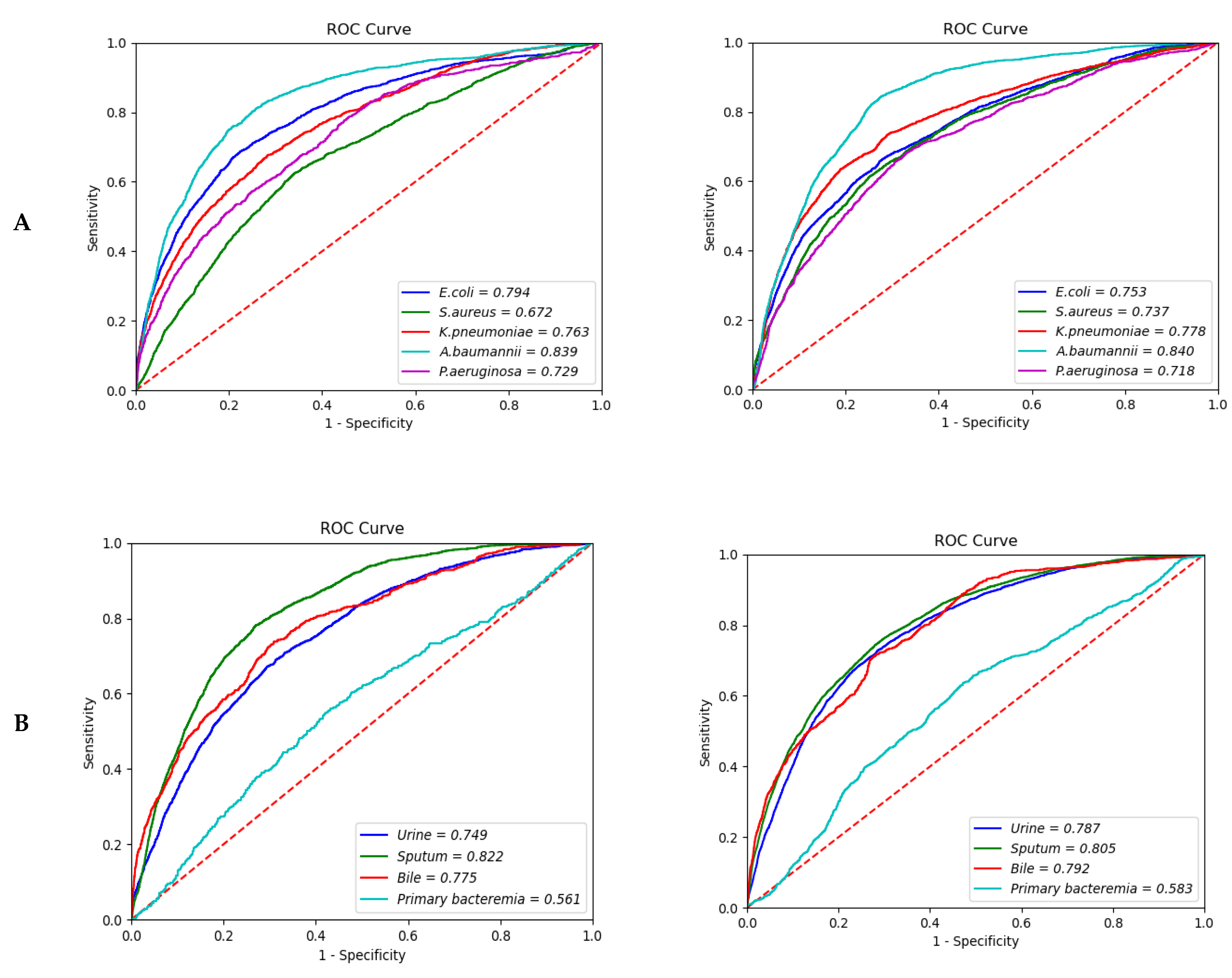
3.3. Type of Pathogen
3.4. Source of Infection
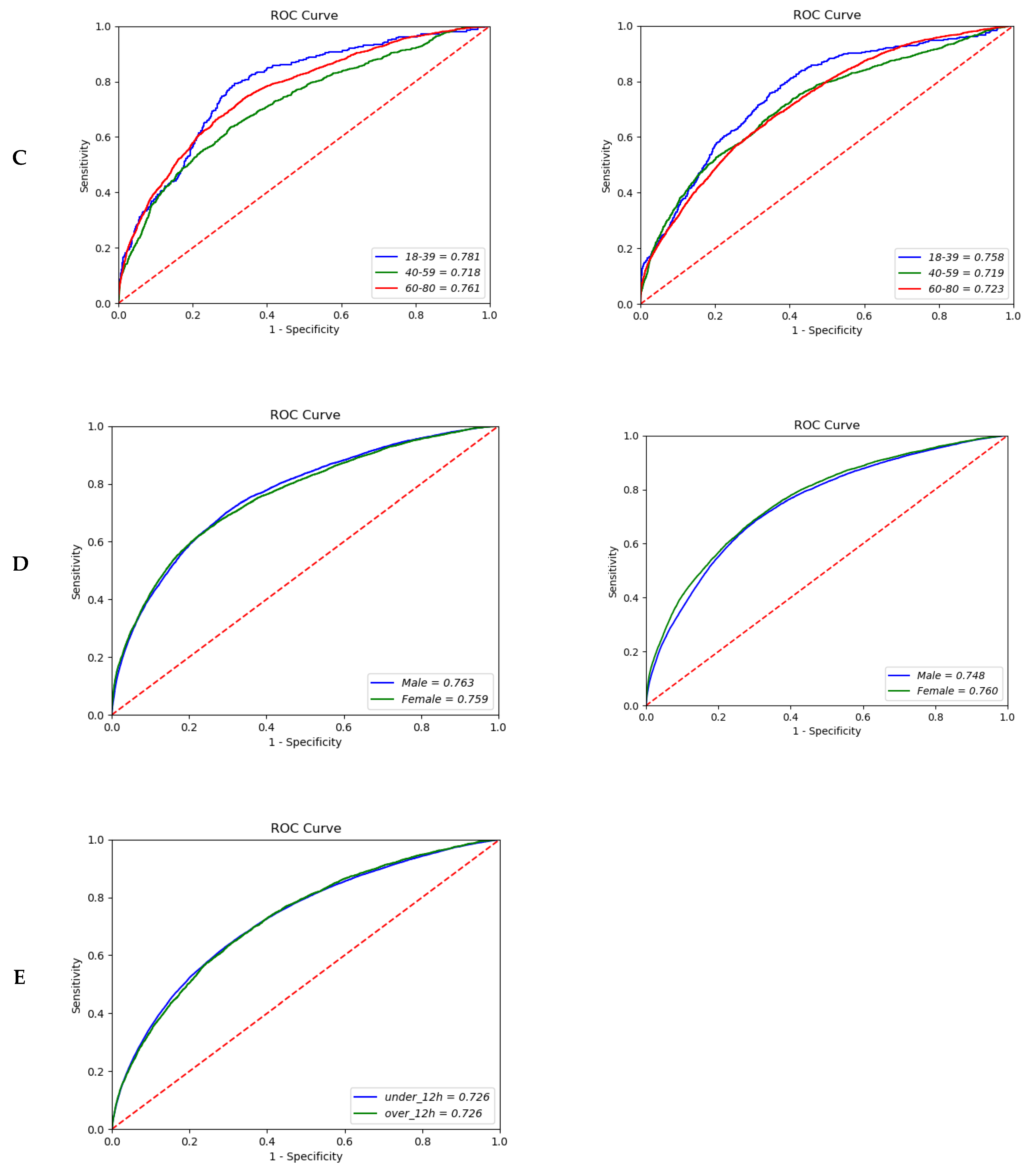
3.5. Age and Sex Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bates, D.W.; Pruess, K.E.; Lee, T.H. How bad are bacteremia and sepsis? Outcomes in a cohort with suspected bacteremia. Arch. Intern. Med. 1995, 155, 593–598. [Google Scholar] [CrossRef]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial bloodstream infections in us hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Vallés, J.; Rello, J.; Ochagavía, A.; Garnacho, J.; Alcalá, M.A. Community-acquired bloodstream infection in critically ill adult patients: Impact of shock and inappropriate antibiotic therapy on survival. Chest 2003, 123, 1615–1624. [Google Scholar] [CrossRef]
- Lachhab, Z.; Frikh, M.; Maleb, A.; Kasouati, J.; Doghmi, N.; Ben Lahlou, Y.; Belefquih, B.; Lemnouer, A.; Elouennass, M. Bacteraemia in intensive care unit: Clinical, bacteriological, and prognostic prospective study. Can. J. Infect. Dis. Med. Microbiol. 2017, 2017, 4082938. [Google Scholar] [CrossRef] [PubMed]
- Retamar, P.; Portillo, M.M.; López-Prieto, M.D.; Rodríguez-López, F.; de Cueto, M.; García, M.V.; Gómez, M.J.; Del Arco, A.; Muñoz, A.; Sánchez-Porto, A.; et al. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: A propensity score-based analysis. Antimicrob. Agents Chemother. 2012, 56, 472–478. [Google Scholar] [CrossRef] [Green Version]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Goosens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M.; Group, E.P. Outpatient antibiotic use in europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Mohan, S.; Thirumalai, C.; Srivastava, G. Effective heart disease prediction using hybrid machine learning techniques. IEEE Access 2019, 7, 81542–81554. [Google Scholar] [CrossRef]
- Angraal, S.; Mortazavi, B.J.; Gupta, A.; Khera, R.; Ahmad, T.; Desai, N.R.; Jacoby, D.L.; Masoudi, F.A.; Spertus, J.A.; Krumholz, H.M. Machine learning prediction of mortality and hospitalization in heart failure with preserved ejection fraction. JACC Heart Fail. 2020, 8, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Prater, A.B.; Hutson, R.K.; Andriole, K.P.; Dreyer, K.J.; Morey, J.; Prevedello, L.M.; Clark, T.J.; Geis, J.R.; Itri, J.N. Machine learning in radiology: Applications beyond image interpretation. J. Am. Coll. Radiol. 2018, 15, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.L.H.; To, C.C.K.; Lee, A.L.S.; Chan, R.C.K.; Wong, J.S.H.; Wong, C.W.; Chow, V.C.Y.; Lai, R.W.M. Deep learning model for prediction of extended-spectrum beta-lactamase (esbl) production in community-onset enterobacteriaceae bacteraemia from a high esbl prevalence multi-centre cohort. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1049–1061. [Google Scholar] [CrossRef]
- Forsblom, E.; Ruotsalainen, E.; Järvinen, A. Improved outcome with early rifampicin combination treatment in methicillin-sensitive staphylococcus aureus bacteraemia with a deep infection focus–a retrospective cohort study. PLoS ONE 2015, 10, e0122824. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.; Jay, M.; Hoffman, J.L.; Calvert, J.; Barton, C.; Shimabukuro, D.; Shieh, L.; Chettipally, U.; Fletcher, G.; Kerem, Y.; et al. Multicentre validation of a sepsis prediction algorithm using only vital sign data in the emergency department, general ward and icu. BMJ Open 2018, 8, e017833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemati, S.; Holder, A.; Razmi, F.; Stanley, M.D.; Clifford, G.D.; Buchman, T.G. An interpretable machine learning model for accurate prediction of sepsis in the icu. Crit. Care Med. 2018, 46, 547. [Google Scholar] [CrossRef]
- Jin, S.J.; Kim, M.; Yoon, J.H.; Song, Y.G. A new statistical approach to predict bacteremia using electronic medical records. Scand. J. Infect. Dis. 2013, 45, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Dong, J.J.; Jeong, S.J.; Chae, M.H.; Lee, B.S.; Kim, H.J.; Ko, S.H.; Song, Y.G. Early detection of bacteraemia using ten clinical variables with an artificial neural network approach. J. Clin. Med. 2019, 8, 1592. [Google Scholar] [CrossRef] [Green Version]
- Mozes, B.; Milatiner, D.; Block, C.; Blumstein, Z.; Halkin, H. Inconsistency of a model aimed at predicting bacteremia in hospitalized patients. J. Clin. Epidemiol. 1993, 46, 1035–1040. [Google Scholar] [CrossRef]
- Bates, D.W.; Sands, K.; Miller, E.; Lanken, P.N.; Hibberd, P.L.; Graman, P.S.; Schwartz, J.S.; Kahn, K.; Snydman, D.R.; Parsonnet, J.; et al. Predicting bacteremia in patients with sepsis syndrome. Academic medical center consortium sepsis project working group. J. Infect. Dis. 1997, 176, 1538–1551. [Google Scholar] [CrossRef] [Green Version]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. Cdc/nhsn surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Ke, G.; Meng, Q.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.-Y. Lightgbm: A highly efficient gradient boosting decision tree. Adv. Neural Inf. Process. Syst. 2017, 30, 3146–3154. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Krogh, A.; Hertz, J.A. A simple weight decay can improve generalization. In Proceedings of the Advances in Neural Information Processing Systems, Denver, CO, USA, 30 November–3 December 1992; pp. 950–957. [Google Scholar]
- Tieleman, T.; Hinton, G. Lecture 6.5-rmsprop: Divide the gradient by a running average of its recent magnitude. Neural Netw. Mach. Learn. 2012, 4, 26–31. [Google Scholar]
- Vinayak, R.K.; Gilad-Bachrach, R. Dart: Dropouts Meet Multiple Additive Regression Trees. In Proceedings of the Eighteenth International Conference on Artificial Intelligence and Statistics, San Diego, CA, USA, 10–12 May 2015; pp. 489–497. [Google Scholar]
- Nathan, C. Neutrophils and immunity: Challenges and opportunities. Nat. Rev. Immunol. 2006, 6, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Papayannopoulos, V. Neutrophil extracellular traps in immunity and disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.P.; Nicholls, A.J.; Wong, C.H. Partners in crime: Neutrophils and monocytes/macrophages in inflammation and disease. Cell Tissue Res. 2018, 371, 551–565. [Google Scholar] [CrossRef] [Green Version]
- Guclu, E.; Durmaz, Y.; Karabay, O. Effect of severe sepsis on platelet count and their indices. Afr. Health Sci. 2013, 13, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Pigozzi, L.; Aron, J.P.; Ball, J.; Cecconi, M. Understanding platelet dysfunction in sepsis. Intensive Care Med. 2016, 42, 583–586. [Google Scholar] [CrossRef]
- Katz, J.N.; Kolappa, K.P.; Becker, R.C. Beyond thrombosis: The versatile platelet in critical illness. Chest 2011, 139, 658–668. [Google Scholar] [CrossRef]
- de Stoppelaar, S.F.; van’t Veer, C.; van der Poll, T. The role of platelets in sepsis. Thromb. Haemost. 2014, 112, 666–677. [Google Scholar]
- Akca, S.; Haji-Michael, P.; De Mendonça, A.; Suter, P.; Levi, M.; Vincent, J.-L. Time course of platelet counts in critically ill patients. Crit. Care Med. 2002, 30, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Blyth, C.C.; Campbell, A.J.; Bowen, A.C. Infection characteristics and treatment of staphylococcus aureus bacteraemia at a tertiary children’s hospital. BMC Infect. Dis. 2018, 18, 387. [Google Scholar] [CrossRef]
- Antonio, M.; Gudiol, C.; Royo-Cebrecos, C.; Grillo, S.; Ardanuy, C.; Carratalà, J. Current etiology, clinical features and outcomes of bacteremia in older patients with solid tumors. J. Geriatr. Oncol. 2019, 10, 246–251. [Google Scholar] [CrossRef]
- Lee, C.-C.; Lee, C.-H.; Hong, M.-Y.; Tang, H.-J.; Ko, W.-C. Timing of appropriate empirical antimicrobial administration and outcome of adults with community-onset bacteremia. Crit. Care 2017, 21, 119. [Google Scholar] [CrossRef] [Green Version]
- Gavazzi, G.; Krause, K.-H. Ageing and infection. Lancet Infect. Dis. 2002, 2, 659–666. [Google Scholar] [CrossRef]
- Werner, H.; Kuntsche, J. Infection in the elderly—What is different? Z. Fur Gerontol. Und Geriatr. 2000, 33, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Ratzinger, F.; Haslacher, H.; Perkmann, T.; Pinzan, M.; Anner, P.; Makristathis, A.; Burgmann, H.; Heinze, G.; Dorffner, G. Machine learning for fast identification of bacteraemia in sirs patients treated on standard care wards: A cohort study. Sci. Rep. 2018, 8, 12233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, F.F.; Petersen, J.A. Novel biomarkers for sepsis: A narrative review. Eur. J. Intern. Med. 2017, 45, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Dolin, H.H.; Papadimos, T.J.; Stepkowski, S.; Chen, X.; Pan, Z.K. A novel combination of biomarkers to herald the onset of sepsis prior to the manifestation of symptoms. Shock 2018, 49, 364. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type of Data | Model | AUROC (95% CI) | Sensitivity | Specificity |
|---|---|---|---|---|
| 12 h | MLP | 0.762 (0.7617–0.7623) | 0.695 | 0.706 |
| Random Forest | 0.758 (0.7572–0.7591) | 0.664 | 0.723 | |
| XGBoost (Gbtree) | 0.745 (0.7446–0.7455) | 0.629 | 0.747 | |
| XGBoost (DART) | 0.744 (0.7439–0.7446) | 0.638 | 0.747 | |
| 24 h | MLP | 0.753 (0.7520–0.7529) | 0.602 | 0.730 |
| Random Forest | 0.738 (0.7383–0.7401) | 0.643 | 0.729 | |
| XGBoost (Gbtree) | 0.730 (0.7300–0.7304) | 0.607 | 0.729 | |
| XGBoost (DART) | 0.727 (0.7256–0.7275) | 0.602 | 0.702 |
| Rank | Data Fusion within 12-h | Data Fusion within 24-h |
|---|---|---|
| 1 | Monocyte | Monocyte |
| 2 | Platelet | Neutrophil |
| 3 | Hospital stay * | Platelet |
| 4 | Neutrophil | Albumin |
| 5 | T. bilirubin | ALP |
| 6 | BUN | T. bilirubin |
| 7 | Albumin | tCO2 |
| 8 | tCO2 | BUN |
| 9 | AST | Hospital stay * |
| 10 | ALP | CRP |
| 11 | ALT | Total Protein |
| 12 | White blood cell count | Creatinine |
| 13 | Chloride | ALT |
| 14 | aPTT | Pulse rate |
| 15 | Total Protein | Prothrombin time |
| 16 | Pulse rate | Hemoglobin |
| 17 | Respiratory rate | AST |
| 18 | DBP | Sodium |
| 19 | Creatinine | Chloride |
| 20 | CRP | ESR |
| Type of Data | Subgroup | With Bacteremia | Without Bacteremia | AUROC (95% CI) | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|
| 12 h | Pathogen | E. coli | 1805 | 14,068 | 0.794 (0.7928–0.7946) | 0.693 | 0.766 |
| S. aureus | 1827 | 14,068 | 0.672 (0.6717–0.6741) | 0.656 | 0.618 | ||
| K. pneumoniae | 1518 | 14,068 | 0.763 (0.7616–0.7658) | 0.677 | 0.716 | ||
| A. baumannii | 1727 | 14,068 | 0.839 (0.8388–0.8394) | 0.789 | 0.750 | ||
| P. aeruginosa | 855 | 14,068 | 0.729 (0.7278–0.7331) | 0.611 | 0.706 | ||
| Infection site | Urine | 2202 | 21,540 | 0.749 (0.7485–0.7504) | 0.642 | 0.725 | |
| Sputum | 3051 | 21,540 | 0.822 (0.8217–0.8229) | 0.792 | 0.715 | ||
| Bile | 650 | 21,540 | 0.775 (0.7742–0.7764) | 0.739 | 0.684 | ||
| Primary bacteremia | 557 | 21,540 | 0.561 (0.5572–0.5651) | 0.636 | 0.473 | ||
| Age | 18–39 years | 1377 | 3885 | 0.781 (0.7780–0.7868) | 0.3923 | 0.8898 | |
| 40–59 years | 5141 | 8359 | 0.718 (0.7152–0.7190) | 0.5818 | 0.7382 | ||
| 60–80 years | 8936 | 14,862 | 0.761 (0.7594–0.7622) | 0.7405 | 0.6597 | ||
| Sex | Male | 9416 | 117,535 | 0.763 (0.7630–0.7636) | 0.710 | 0.694 | |
| Female | 6038 | 81,236 | 0.759 (0.7586–0.7600) | 0.670 | 0.724 | ||
| 24 h | Pathogen | E. coli | 2771 | 22,114 | 0.753 (0.7523–0.7353) | 0.639 | 0.738 |
| S. aureus | 2949 | 22,114 | 0.737 (0.7354–0.7376) | 0.668 | 0.684 | ||
| K. pneumoniae | 2376 | 22,114 | 0.778 (0.7777–0.7795) | 0.706 | 0.730 | ||
| A. baumannii | 2621 | 22,114 | 0.840 (0.8400–0.8407) | 0.817 | 0.747 | ||
| P. aeruginosa | 1280 | 22,114 | 0.718 (0.7170–0.7209) | 0.688 | 0.661 | ||
| Infection site | Urine | 3489 | 34,502 | 0.787 (0.7860–0.7878) | 0.751 | 0.689 | |
| Sputum | 4700 | 34,502 | 0.805 (0.8041–0.8052) | 0.670 | 0.756 | ||
| Bile | 1022 | 34,502 | 0.792 (0.7910–0.7936) | 0.659 | 0.740 | ||
| Primary bacteremia | 987 | 7169 | 0.583 (0.5823–0.5855) | 0.517 | 0.616 | ||
| Age | 18–39 years | 413 | 5712 | 0.758 (0.7554–0.7648) | 0.463 | 0.845 | |
| 40–59 years | 1415 | 12,415 | 0.719 (0.7176–0.7214) | 0.566 | 0.749 | ||
| 60–80 years | 3026 | 21,154 | 0.723 (0.7221–0.7238) | 0.560 | 0.713 | ||
| Sex | Male | 14,585 | 241,478 | 0.748 (0.7473–0.7481) | 0.673 | 0.707 | |
| Female | 10,030 | 164,521 | 0.760 (0.7597–0.7608) | 0.619 | 0.760 | ||
| Merge hour | Under 12 h | 323,949 | 20,608 | 0.726 (0.7261–0.7266) | 0.631 | 0.705 | |
| Over 12 h | 82,050 | 3957 | 0.726 (0.7253–0. 7258) | 0.653 | 0.679 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.H.; Dong, J.J.; Kim, S.; Kim, D.; Hyun, J.H.; Chae, M.-H.; Lee, B.S.; Song, Y.G. Prediction of Bacteremia Based on 12-Year Medical Data Using a Machine Learning Approach: Effect of Medical Data by Extraction Time. Diagnostics 2022, 12, 102. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010102
Lee KH, Dong JJ, Kim S, Kim D, Hyun JH, Chae M-H, Lee BS, Song YG. Prediction of Bacteremia Based on 12-Year Medical Data Using a Machine Learning Approach: Effect of Medical Data by Extraction Time. Diagnostics. 2022; 12(1):102. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010102
Chicago/Turabian StyleLee, Kyoung Hwa, Jae June Dong, Subin Kim, Dayeong Kim, Jong Hoon Hyun, Myeong-Hun Chae, Byeong Soo Lee, and Young Goo Song. 2022. "Prediction of Bacteremia Based on 12-Year Medical Data Using a Machine Learning Approach: Effect of Medical Data by Extraction Time" Diagnostics 12, no. 1: 102. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010102