
Accuracy and Clinical Relevance of Intra-Tumoral Fusobacterium nucleatum Detection in Formalin-Fixed Paraffin-Embedded (FFPE) Tissue by Droplet Digital PCR (ddPCR) in Colorectal Cancer

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Tissue Samples
2.2. Detection of Fn DNA by Quantitative PCR (qPCR)
2.3. Detection of Fn DNA by Droplet Digital PCR (ddPCR)
2.4. Optimization and Analytical Assessment of ddPCR-Based Fn DNA Detection Assay
2.5. Determination of the Limit of Blank (LoB) and Limit of Detection (LoD) of Fn ddPCR
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Optimization of ddPCR Assay and Determination of Fn ddPCR LoB and LoD
3.3. Detection of Fn DNA by ddPCR and Comparison with qPCR
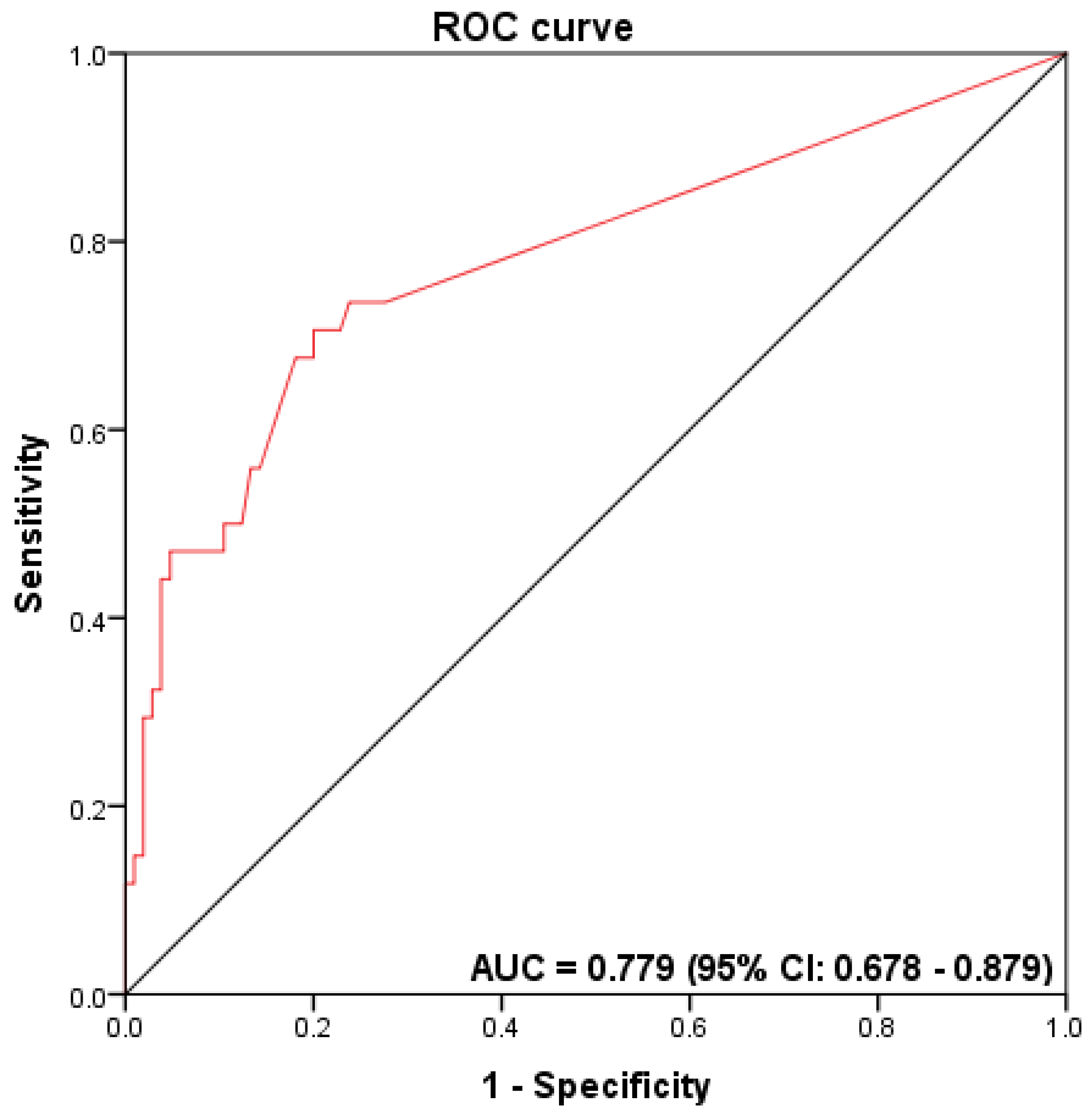
3.4. Accuracy Measurements for Fn Detection
3.5. Association between Fn Status and Patients’ Clinical-Pathological and Molecular Features
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Estimativa 2020/Incidência de Câncer no Brasil. 2020. Available online: https://www.inca.gov.br/estimativa (accessed on 19 May 2021).
- Souza, D.L.; Jerez-Roig, J.; Cabral, F.J.; de Lima, J.R.; Rutalira, M.K.; Costa, J.A. Colorectal cancer mortality in Brazil: Predictions until the year 2025 and cancer control implications. Dis. Colon Rectum 2014, 57, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E.J.; Grady, W.M.; Lieberman, D.; Seufferlein, T.; Sung, J.J.; Boelens, P.G. Colorectal cancer. Nat. Rev. Dis. Primers 2015, 1, 15065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inamura, K. Colorectal Cancers: An Update on Their Molecular Pathology. Cancers 2018, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Krimpenfort, P.; Song, J.-Y.; Proost, N.; Zevenhoven, J.; Jonkers, J.; Berns, A. Deleted in colorectal carcinoma suppresses metastasis in p53-deficient mammary tumours. Nat. Cell Biol. 2012, 482, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Diakowska, D.; Kapturkiewicz, B.; Bębenek, M.; Gamian, A. Profiles of circulating inflammatory cytokines in colorectal cancer (CRC), high cancer risk conditions, and health are distinct. Possible implications for CRC screening and surveillance. Cancer Lett. 2013, 337, 107–114. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Carneseca, E.C.; Mauad, E.C.; De Araujo, M.A.A.; DalBó, R.M.; Longatto-Filho, A.; Vazquez, V.D.L. The Hospital de Câncer de Barretos Registry: An analysis of cancer survival at a single institution in Brazil over a 10-year period. BMC Res. Notes 2013, 6, 141. [Google Scholar] [CrossRef] [Green Version]
- FDA-NIH Biomarker Working Group BEST (Biomarkers, EndpointS, and other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA, 2016. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK326791/ (accessed on 12 October 2020).
- Janney, A.; Powrie, F.; Mann, E.H. Host–microbiota maladaptation in colorectal cancer. Nat. Cell Biol. 2020, 585, 509–517. [Google Scholar] [CrossRef]
- Brennan, C.A.; Garrett, W.S. Gut Microbiota, Inflammation, and Colorectal Cancer. Annu. Rev. Microbiol. 2016, 70, 395–411. [Google Scholar] [CrossRef] [Green Version]
- Kostic, A.D.; Chun, E.; Robertson, L.; Glickman, J.N.; Gallini, C.A.; Michaud, M.; Clancy, T.E.; Chung, D.C.; Lochhead, P.; Hold, G.L.; et al. Fusobacterium nucleatum Potentiates Intestinal Tumorigenesis and Modulates the Tumor-Immune Microenvironment. Cell Host Microbe 2013, 14, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Rubinstein, M.R.; Wang, X.; Liu, W.; Hao, Y.; Cai, G.; Han, Y.W. Fusobacterium nucleatum Promotes Colorectal Carcinogenesis by Modulating E-Cadherin/β-Catenin Signaling via its FadA Adhesin. Cell Host Microbe 2013, 14, 195–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Weng, W.; Peng, J.; Hong, L.; Yang, L.; Toiyama, Y.; Gao, R.; Liu, M.; Yin, M.; Pan, C.; et al. Fusobacterium nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor-κB, and Up-regulating Expression of MicroRNA-21. Gastroenterology 2017, 152, 851–866.e24. [Google Scholar] [CrossRef] [Green Version]
- Datorre, J.G.; de Carvalho, A.C.; Guimarães, D.P.; Reis, R.M. The Role of Fusobacterium nucleatum in Colorectal Carcinogenesis. Pathobiology 2021, 88, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Signat, B.; Roques, C.; Poulet, P.; Duffaut, D. Fusobacterium nucleatum in periodontal health and disease. Curr. Issues Mol. Biol. 2011, 13, 25–36. [Google Scholar] [PubMed]
- de Carvalho, A.C.; de Mattos Pereira, L.; Datorre, J.G.; Dos Santos, W.; Berardinelli, G.N.; Matsushita, M.D.; Oliveira, M.A.; Durães, R.O.; Guimarães, D.P.; Reis, R.M. Microbiota Profile and Impact of Fusobacterium nucleatum in Colorectal Cancer Patients of Barretos Cancer Hospital. Front. Oncol. 2019, 9, 813. [Google Scholar] [CrossRef] [Green Version]
- Mima, K.; Nishihara, R.; Qian, Z.R.; Cao, Y.; Sukawa, Y.; Nowak, J.A.; Yang, J.; Dou, R.; Masugi, Y.; Song, M.; et al. Fusobacterium nucleatum in colorectal carcinoma tissue and patient prognosis. Gut 2016, 65, 1973–1980. [Google Scholar] [CrossRef] [Green Version]
- Mima, K.; Sukawa, Y.; Nishihara, R.; Qian, Z.R.; Yamauchi, M.; Inamura, K.; Kim, S.A.; Masuda, A.; Nowak, J.A.; Nosho, K.; et al. Fusobacterium nucleatum and T Cells in Colorectal Carcinoma. JAMA Oncol. 2015, 1, 653–661. [Google Scholar] [CrossRef] [Green Version]
- Pignatelli, P.; Iezzi, L.; Pennese, M.; Raimondi, P.; Cichella, A.; Bondi, D.; Grande, R.; Cotellese, R.; Di Bartolomeo, N.; Innocenti, P.; et al. The Potential of Colonic Tumor Tissue Fusobacterium nucleatum to Predict Staging and Its Interplay with Oral Abundance in Colon Cancer Patients. Cancers 2021, 13, 1032. [Google Scholar] [CrossRef]
- Villar-Ortega, P.; Expósito-Ruiz, M.; Gutiérrez-Soto, M.; Ruiz-Cabello Jiménez, M.; Navarro-Marí, J.M.; Gutiérrez-Fernández, J. The association between Fusobacterium nucleatum and cancer colorectal: A systematic review and meta-analysis. Enferm. Infecc. Microbiol. Clin. 2021, in press. [Google Scholar] [CrossRef]
- Huangfu, S.-C.; Zhang, W.-B.; Zhang, H.-R.; Li, Y.; Zhang, Y.-R.; Nie, J.-L.; Chu, X.-D.; Chen, C.-S.; Jiang, H.-P.; Pan, J.-H. Clinicopathological and prognostic significance of Fusobacterium nucleatum infection in colorectal cancer: A meta-analysis. J. Cancer 2021, 12, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Gethings-Behncke, C.; Coleman, H.G.; Jordao, H.W.; Longley, D.B.; Crawford, N.; Murray, L.J.; Kunzmann, A.T. Fusobacterium nucleatum in the Colorectum and Its Association with Cancer Risk and Survival: A Systematic Review and Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2020, 29, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Shang, F.-M.; Liu, H.-L. Fusobacterium nucleatum and colorectal cancer: A review. World J. Gastrointest. Oncol. 2018, 10, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Hussan, H.; Clinton, S.K.; Roberts, K.; Bailey, M. Fusobacterium’s link to colorectal neoplasia sequenced: A systematic review and future insights. World J. Gastroenterol. 2017, 23, 8626–8650. [Google Scholar] [CrossRef]
- Huggett, J.F.; Foy, C.A.; Benes, V.; Emslie, K.R.; Garson, J.; Haynes, R.J.; Hellemans, J.; Kubista, M.; Mueller, R.D.; Nolan, T.; et al. The Digital MIQE Guidelines: Minimum Information for Publication of Quantitative Digital PCR Experiments. Clin. Chem. 2013, 59, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Schiavetto, C.M.; de Abreu, P.M.; von Zeidler, S.V.; de Jesus, L.M.; Carvalho, R.S.; Cirino, M.T.; Carloni, A.C.; Oliveira, C.; Scapulatempo-Neto, C.; de Almeida, G.C.; et al. Human Papillomavirus DNA Detection by Droplet Digital PCR in Formalin-Fixed Paraffin-Embedded Tumor Tissue from Oropharyngeal Squamous Cell Carcinoma Patients. Mol. Diagn. Ther. 2021, 25, 59–70. [Google Scholar] [CrossRef]
- Berardinelli, G.N.; Scapulatempo-Neto, C.; Durães, R.; De Oliveira, M.A.; Guimarães, D.; Reis, R. Advantage of HSP110 (T17) marker inclusion for microsatellite instability (MSI) detection in colorectal cancer patients. Oncotarget 2018, 9, 28691–28701. [Google Scholar] [CrossRef] [Green Version]
- Schmittgen, T.D.; Livak, K.J. Analyzing real-time PCR data by the comparative C(T) method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef]
- Suehiro, Y.; Sakai, K.; Nishioka, M.; Hashimoto, S.; Takami, T.; Higaki, S.; Shindo, Y.; Hazama, S.; Oka, M.; Nagano, H.; et al. Highly sensitive stool DNA testing of Fusobacterium nucleatum as a marker for detection of colorectal tumours in a Japanese population. Ann. Clin. Biochem. Int. J. Lab. Med. 2017, 54, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Huggett, J.F.; The dMIQE Group; Whale, A.S.; De Spiegelaere, W.; Trypsteen, W.; Nour, A.A.; Bae, Y.-K.; Benes, V.; Burke, D.; Cleveland, M.; et al. The Digital MIQE Guidelines Update: Minimum Information for Publication of Quantitative Digital PCR Experiments for 2020. Clin. Chem. 2020, 66, 1012–1029. [Google Scholar] [CrossRef]
- Armbruster, D.; Pry, T. Limit of Blank, Limit of Detection and Limit of Quantitation. Clin. Biochem. Rev. 2008, 29, S49–S52. [Google Scholar]
- Lee, S.A.; Liu, F.; Riordan, S.M.; Lee, C.S.; Zhang, L. Global Investigations of Fusobacterium nucleatum in Human Colorectal Cancer. Front. Oncol. 2019, 9, 566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imrit, K.; Goldfischer, M.; Wang, J.; Green, J.; Levine, J.; Lombardo, J.; Hong, T. Identification of Bacteria in Formalin-Fixed, Paraffin-Embedded Heart Valve Tissue via 16S rRNA Gene Nucleotide Sequencing. J. Clin. Microbiol. 2006, 44, 2609–2611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mima, K.; Cao, Y.; Chan, A.T.; Qian, Z.R.; Nowak, J.A.; Masugi, Y.; Shi, Y.; Song, M.; Da Silva, A.; Gu, M.; et al. Fusobacterium nucleatum in Colorectal Carcinoma Tissue According to Tumor Location. Clin. Transl. Gastroenterol. 2016, 7, e200. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Coker, O.O.; Nakatsu, G.; Wu, W.K.K.; Zhao, L.; Chen, Z.; Chan, F.K.L.; Kristiansen, K.; Sung, J.J.Y.; Wong, S.H.; et al. Multi-cohort analysis of colorectal cancer metagenome identified altered bacteria across populations and universal bacterial markers. Microbiome 2018, 6, 70. [Google Scholar] [CrossRef]
- Castellarin, M.; Warren, R.L.; Freeman, J.D.; Dreolini, L.; Krzywinski, M.; Strauss, J.; Barnes, R.; Watson, P.; Allen-Vercoe, E.; Moore, R.A.; et al. Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Res. 2012, 22, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, L.; Cui, X.; Hu, J.; Li, Z.; Choi, J.R.; Yang, Q.; Lin, M.; Hui, L.Y.; Xu, F. Advances in digital polymerase chain reaction (dPCR) and its emerging biomedical applications. Biosens. Bioelectron. 2017, 90, 459–474. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Griffith, J.; Dorevitch, S.; Weisberg, S. Effectiveness of qPCR permutations, internal controls and dilution as means for minimizing the impact of inhibition while measuring Enterococcus in environmental waters. J. Appl. Microbiol. 2012, 113, 66–75. [Google Scholar] [CrossRef]
- Yuan, D.; Cui, M.; Yu, S.; Wang, H.; Jing, R. Droplet digital PCR for quantification of PML-RARα in acute promyelocytic leukemia: A comprehensive comparison with real-time PCR. Anal. Bioanal. Chem. 2019, 411, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Dingle, T.; Sedlak, R.H.; Cook, L.; Jerome, K.R. Tolerance of Droplet-Digital PCR vs Real-Time Quantitative PCR to Inhibitory Substances. Clin. Chem. 2013, 59, 1670–1672. [Google Scholar] [CrossRef] [Green Version]
- Tahara, T.; Yamamoto, E.; Suzuki, H.; Maruyama, R.; Chung, W.; Garriga, J.; Jelinek, J.; Yamano, H.-O.; Sugai, T.; An, B.; et al. Fusobacterium in Colonic Flora and Molecular Features of Colorectal Carcinoma. Cancer Res. 2014, 74, 1311–1318. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, L.; Schmid, J.; Ebert, M.; Soucek, P.; Kunicka, T.; Liška, V.; Bruha, J.; Neary, P.; DeZeeuw, N.; Tommasino, M.; et al. Fusobacterium nucleatum associates with stages of colorectal neoplasia development, colorectal cancer and disease outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1381–1390. [Google Scholar] [CrossRef]
- Lee, D.-W.; Han, S.-W.; Kang, J.-K.; Bae, J.M.; Kim, H.-P.; Won, J.-K.; Jeong, S.-Y.; Park, K.J.; Kang, G.H.; Kim, T.-Y. Association Between Fusobacterium nucleatum, Pathway Mutation, and Patient Prognosis in Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 3389–3395. [Google Scholar] [CrossRef]
- Ito, M.; Kanno, S.; Nosho, K.; Sukawa, Y.; Mitsuhashi, K.; Kurihara, H.; Igarashi, H.; Takahashi, T.; Tachibana, M.; Takahashi, H.; et al. Association of Fusobacterium nucleatum with clinical and molecular features in colorectal serrated pathway. Int. J. Cancer 2015, 137, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Nosho, K.; Sukawa, Y.; Adachi, Y.; Ito, M.; Mitsuhashi, K.; Kurihara, H.; Kanno, S.; Yamamoto, I.; Ishigami, K.; Igarashi, H.; et al. Association of Fusobacterium nucleatum with immunity and molecular alterations in colorectal cancer. World J. Gastroenterol. 2016, 22, 557. [Google Scholar] [CrossRef] [PubMed]
- Park, H.E.; Kim, J.H.; Cho, N.-Y.; Lee, H.S.; Kang, G.H. Intratumoral Fusobacterium nucleatum abundance correlates with macrophage infiltration and CDKN2A methylation in microsatellite-unstable colorectal carcinoma. Virchows Archiv 2017, 471, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Rezasoltani, S.; Sharafkhah, M.; Aghdaei, H.A.; Mojarad, E.N.; Dabiri, H.; Sepahi, A.A.; Modarressi, M.H.; Feizabadi, M.M.; Zali, M.R. Applying simple linear combination, multiple logistic and factor analysis methods for candidate fecal bacteria as novel biomarkers for early detection of adenomatous polyps and colon cancer. J. Microbiol. Methods 2018, 155, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Cilloni, D.; Petiti, J. Digital PCR in Myeloid Malignancies: Ready to Replace Quantitative PCR? Int. J. Mol. Sci. 2019, 20, 2249. [Google Scholar] [CrossRef] [Green Version]
- Kuypers, J.; Jerome, K.R. Applications of Digital PCR for Clinical Microbiology. J. Clin. Microbiol. 2017, 55, 1621–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Number of Cases (n) | (%) | |
|---|---|---|---|
| Mean age 60.65 ± 13.49 | |||
| Gender | Female | 65 | 46.5 |
| Male | 74 | 53.2 | |
| Clinical stage (at diagnosis) | 0/I | 36 | 26.1 |
| II/III | 98 | 69.6 | |
| IV | 6 | 4.3 | |
| Tumor location | Proximal colon | 38 | 27.3 |
| Distal colon | 72 | 51.8 | |
| Rectum | 29 | 20.9 | |
| Tumor (T) | Tis/T1/T2 | 44 | 31.7 |
| T3/T4 (a b) | 95 | 68.3 | |
| Tumor differentiation | Well to moderate | 126 | 92.0 |
| Poor | 11 | 8.0 | |
| MSI status # | MSS/MSI-low | 118 | 84.9 |
| MSI-high | 21 | 15.1 | |
| BRAFmutation # | Mutant | 11 | 8.0 |
| Wild-type | 127 | 92.0 | |
| MLH1 protein expression # | Positive | 105 | 86.1 |
| Negative | 17 | 13.9 | |
| MSH2 protein expression # | Positive | 119 | 97.9 |
| Negative | 3 | 2.1 | |
| MSH6 protein expression # | Positive | 121 | 99.3 |
| Negative | 1 | 0.7 | |
| PMS2 protein expression # | Positive | 107 | 87.7 |
| Negative | 15 | 12.3 | |
| Status | Alive without cancer | 78 | 56.1 |
| Alive with cancer | 7 | 5.0 | |
| Death from cancer | 38 | 27.3 | |
| Death from other causes | 15 | 10.8 |
| Variable | All Cases (%) | ddPCR | qPCR | |||||
|---|---|---|---|---|---|---|---|---|
| Neg/Low n = 111 (79.9) | High n = 28 (20.1) | p-Value * | Neg/Low n = 135 (97.1) | High n = 4 (2.9) | p-Value * | |||
| Age | Mean 60.65 ± 13.49 | |||||||
| Gender | Female | 65 (46.8) | 49 (75.4) | 16 (24.6) | 0.2 | 65 (48.1) | 0 (0.0) | 0.1 |
| Male | 74 (53.2) | 62 (83.8) | 12 (16.2) | 70 (51.9) | 4 (100.0) | |||
| Tumor location | Proximal colon | 38 (27.3) | 26 (23.4) | 12 (42.9) | 0.04 | 36 (26.7) | 2 (50.0) | 0.6 |
| Distal colon | 72 (58.1) | 58 (52.3) | 14 (50.0) | 70 (51.9) | 2 (50.0) | |||
| Rectum | 29 (20.9) | 27 (24.3) | 2 (7.1) | 29 (21.5) | 0 (0.0) | |||
| Tumor (T) | Tis/T1/T2 | 44 (31.7) | 36 (32.4) | 8 (28.6) | 0.6 | 42 (31.1) | 2 (50.0) | 0.5 |
| T3/T4 (a b) | 95 (68.3) | 75 (67.6) | 20 (71.4) | 90 (68.9) | 2 (50.0) | |||
| Clinical stage | 0/I | 37 (26.6) | 30 (27.0) | 7 (25.0) | 1.0 | 35 (25.9) | 2 (50.0) | 0.3 |
| II/III | 96 (69.1) | 76 (68.5) | 20 (71.4) | 94 (69.6) | 2 (50.0) | |||
| IV | 6 ( 4.3) | 5 (4.5) | 1 (3.6) | 6 (4.4) | 0 (0.00) | |||
| Tumor differentiation | Well to moderate | 126 (92.0) | 104 (94.5) | 22 (81.5) | 0.02 | 124 (92.5) | 2 (66.7) | 0.2 |
| Poor | 11 (8.0) | 6 (5.5) | 5 (18.5) | 10 (7.5) | 1 (33.3) | |||
| MSI status | MSS/MSI-Low | 118 (84.9) | 101 (91.0) | 17 (60.7) | <0.001 | 116 (85.9) | 2 (50.0) | 0.1 |
| MSI-High | 21 (15.1) | 10 (9.0) | 11 (39.3) | 19 (14.1) | 2 (50.0) | |||
| BRAFmutation | Mutant | 11 (8.0) | 5 (4.5) | 6 (21.4) | 0.003 | 9 (6.7) | 2 (50.0) | 0.03 |
| WT | 127 (92.0) | 105 (95.5) | 22 (78.6) | 125 (93.3) | 2 (50.0) | |||
| MLH1 protein expression | Positive | 105 (86.1) | 90 (92.8) | 15 (60.0) | <0.001 | 103 (89.6) | 2 (50.0) | 0.09 |
| Negative | 17 (13.9) | 7 (7.2) | 10 (40.0) | 12 (10.4) | 2 (50.0) | |||
| MSH2 protein expression | Positive | 119 (97.5) | 95 (97.9) | 24 (96.4) | 0.5 | 115 (97.5) | 4 (100.0) | 1.0 |
| Negative | 3 (2.5) | 2 (2.1) | 1 (4.0) | 3 (2.5) | 0 (0.0) | |||
| MSH6 protein expression | Positive | 121 (99.2) | 96 (99.0) | 25 (100.0) | 1.0 | 117 (99.2) | 4 (100.0) | 1.0 |
| Negative | 1 (0.8) | 1 (1.0) | 0 (0.0) | 1 (0.8) | 0 (0.0) | |||
| PMS2 protein expression | Positive | 107 (87.7) | 91 (93.8) | 16 (64.0) | <0.001 | 105 (87.3) | 2 (50.0) | 0.07 |
| Negative | 15 (12.3) | 6 (6.2) | 9 (36.0) | 15 (12.7) | 2 (50.0) | |||
| Concordance Rate % (n) | Cohen’s Kappa | |
|---|---|---|
| FFPE ddPCR × FFPE qPCR | 82.8% (115/139) | 0.210 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Datorre, J.G.; de Carvalho, A.C.; dos Reis, M.B.; dos Reis, M.; Matsushita, M.; Santos, F.; Guimarães, D.P.; Reis, R.M. Accuracy and Clinical Relevance of Intra-Tumoral Fusobacterium nucleatum Detection in Formalin-Fixed Paraffin-Embedded (FFPE) Tissue by Droplet Digital PCR (ddPCR) in Colorectal Cancer. Diagnostics 2022, 12, 114. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010114
Datorre JG, de Carvalho AC, dos Reis MB, dos Reis M, Matsushita M, Santos F, Guimarães DP, Reis RM. Accuracy and Clinical Relevance of Intra-Tumoral Fusobacterium nucleatum Detection in Formalin-Fixed Paraffin-Embedded (FFPE) Tissue by Droplet Digital PCR (ddPCR) in Colorectal Cancer. Diagnostics. 2022; 12(1):114. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010114
Chicago/Turabian StyleDatorre, José Guilherme, Ana Carolina de Carvalho, Mariana Bisarro dos Reis, Monise dos Reis, Marcus Matsushita, Florinda Santos, Denise Peixoto Guimarães, and Rui Manuel Reis. 2022. "Accuracy and Clinical Relevance of Intra-Tumoral Fusobacterium nucleatum Detection in Formalin-Fixed Paraffin-Embedded (FFPE) Tissue by Droplet Digital PCR (ddPCR) in Colorectal Cancer" Diagnostics 12, no. 1: 114. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010114