
The Diagnostic Role of Uric Acid to Creatinine Ratio for the Identification of Patients with Adverse Pulmonary Embolism Outcomes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
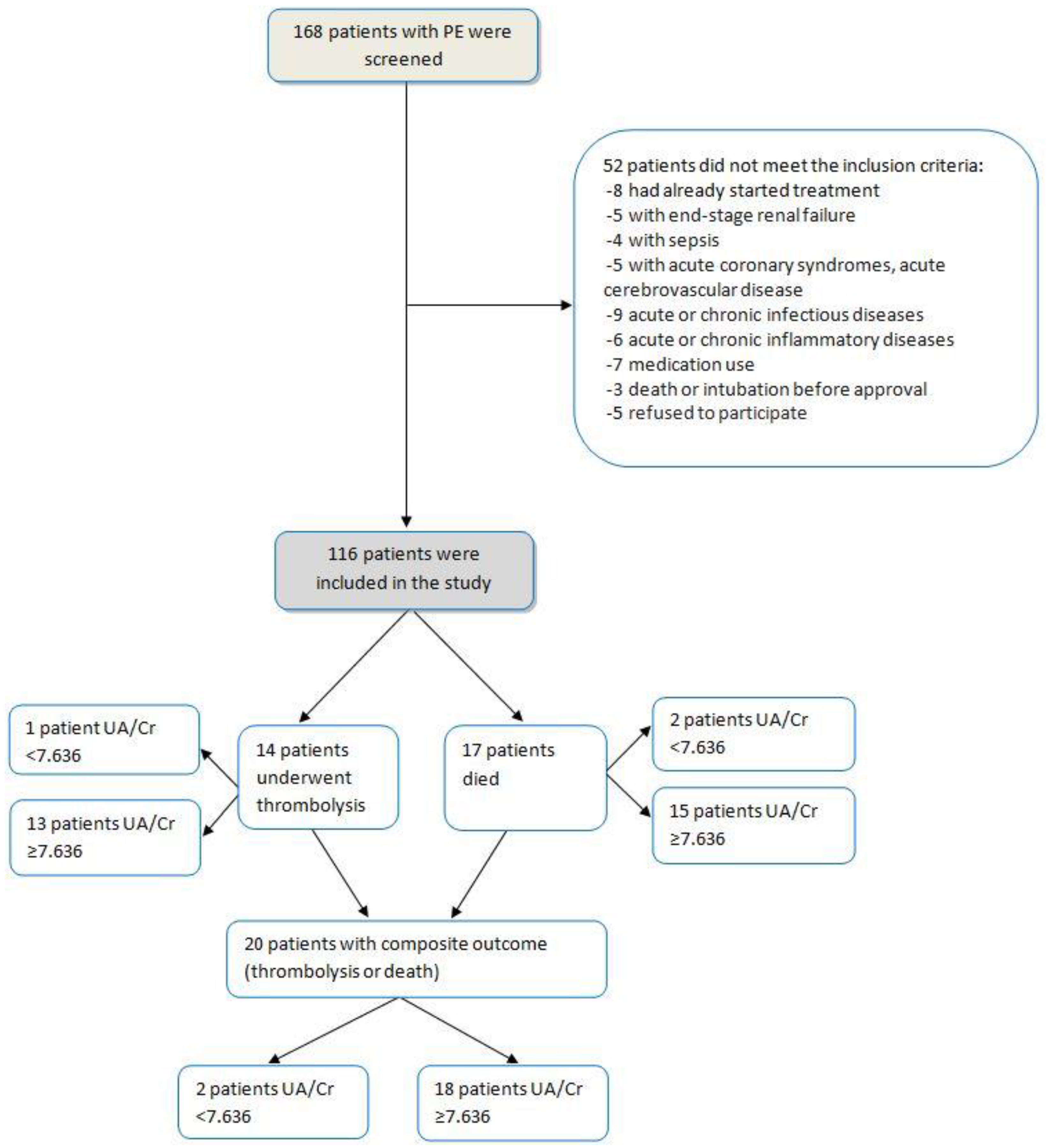
2.2. Subjects and Setting
2.3. Biochemical Analysis
2.4. Statistical Analysis
3. Results
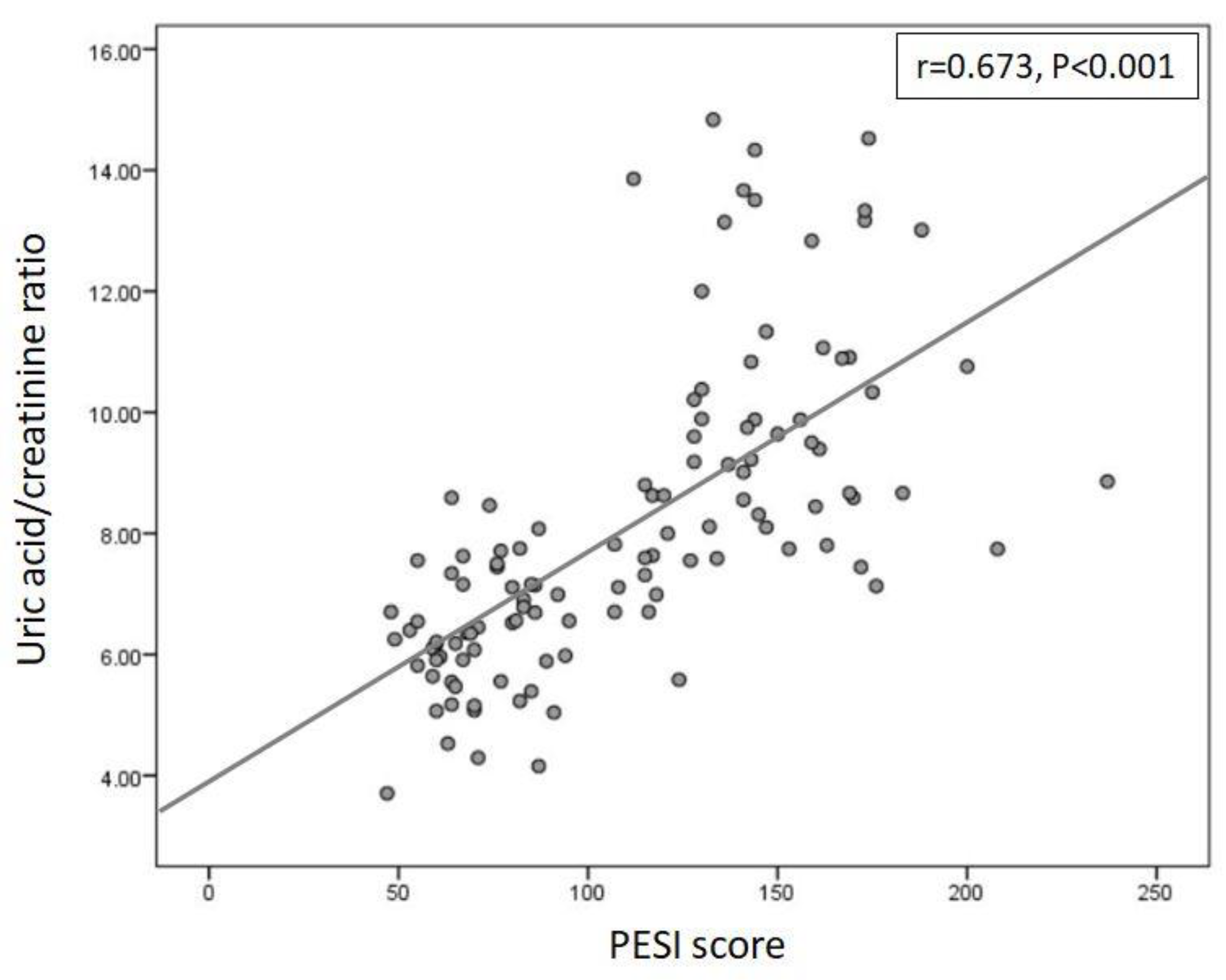
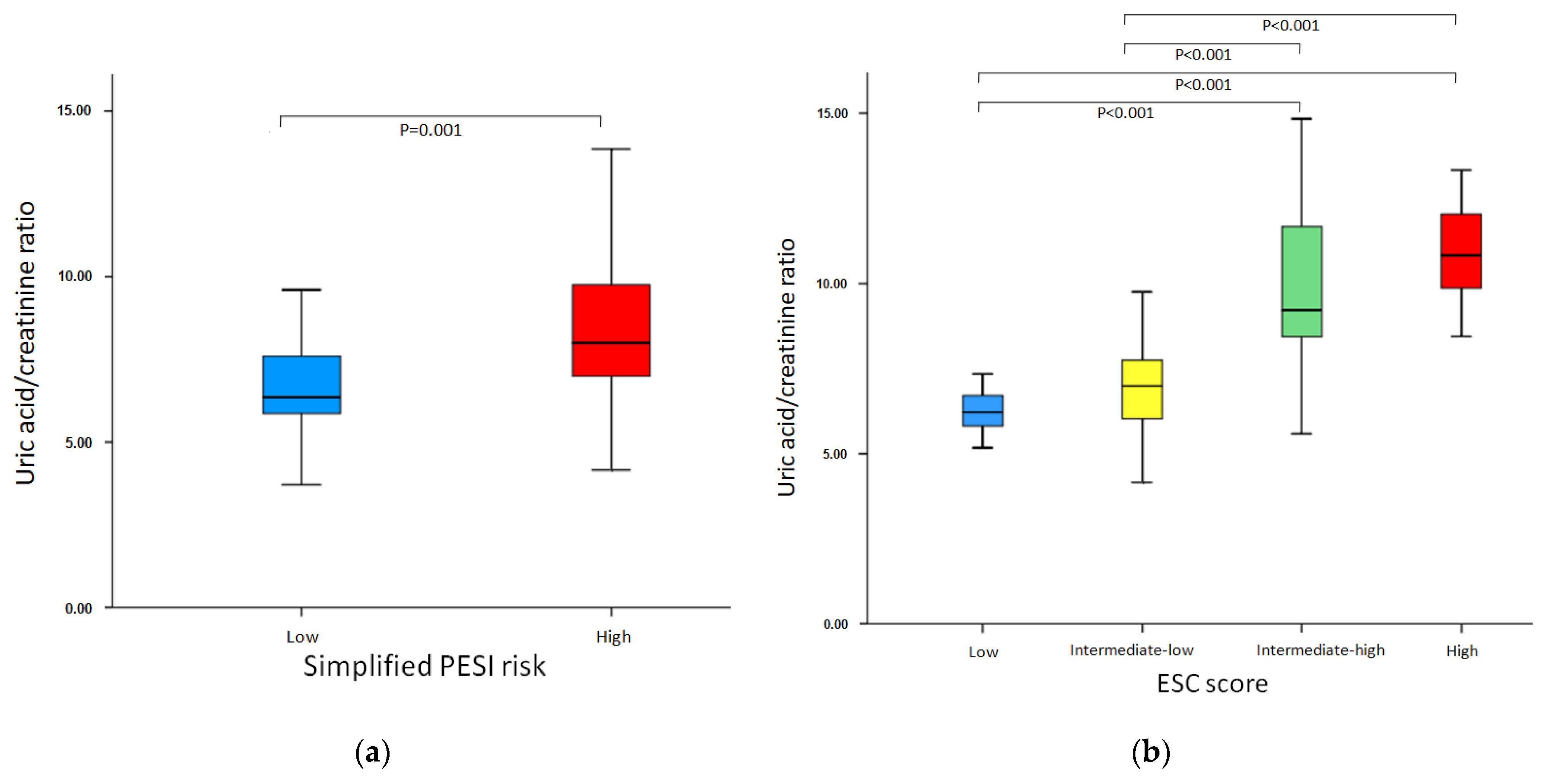
3.1. Association of UA/Cr with PESI Score, Simplified PESI and ESC Risk-Stratification
3.2. Association of UA/Cr Levels with Hospitalization Outcome
3.3. Associations of Demographic and Clinical Variables with Duration of Hospitalization, 30-Day Mortality and Adverse Composite Outcome
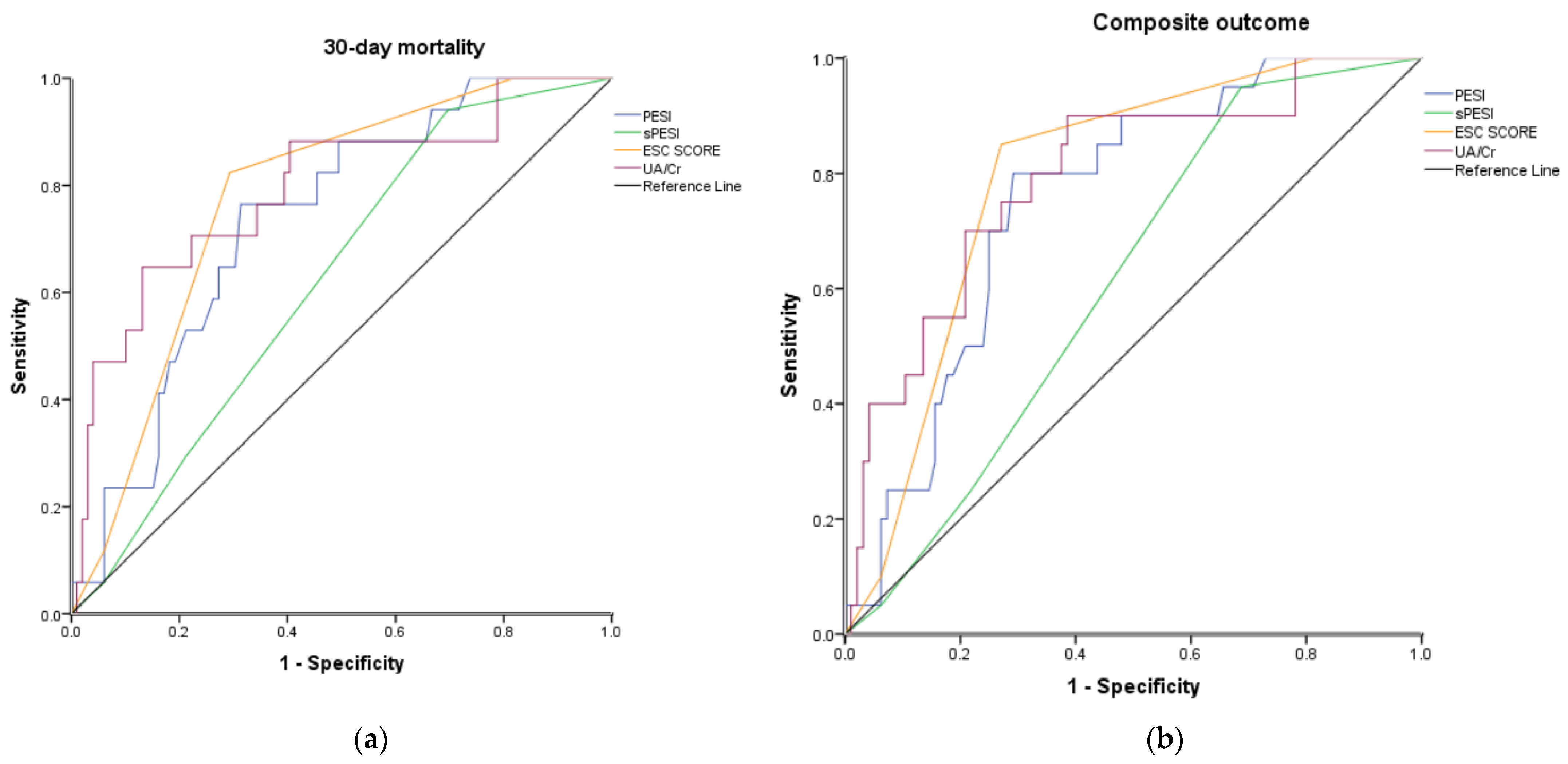
3.4. Comparison with Existing Risk-Factor Prediction Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism Developed in Collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Agnelli, G.; Lankeit, M.; Masotti, L.; Pruszczyk, P.; Casazza, F.; Vanni, S.; Nitti, C.; Kamphuisen, P.; Vedovati, M.C.; et al. Acute Pulmonary Embolism: Mortality Prediction by the 2014 European Society of Cardiology Risk Stratification Model. Eur. Respir. J. 2016, 48, 780–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papaioannou, A.I.; Kostikas, K. Clinical Decision Rules for The Diagnostic Management of Suspected Acute Pulmonary Embolism: The Clinician… Rules. Pneumon 2011, 24, 221–223. [Google Scholar]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Stiell, I.; Dreyer, J.F.; Barnes, D.; Forgie, M.; Kovacs, G.; Ward, J.; Kovacs, M.J. Excluding Pulmonary Embolism at the Bedside without Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Emergency Department by Using a Simple Clinical Model and D-Dimer. Ann. Intern. Med. 2001, 135, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wicki, J.; Perneger, T.V.; Junod, A.F.; Bounameaux, H.; Perrier, A. Assessing Clinical Probability of Pulmonary Embolism in the Emergency Ward: A Simple Score. Arch. Intern. Med. 2001, 161, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Le Gal, G.; Righini, M.; Roy, P.-M.; Sanchez, O.; Aujesky, D.; Bounameaux, H.; Perrier, A. Prediction of Pulmonary Embolism in the Emergency Department: The Revised Geneva Score. Ann. Intern. Med. 2006, 144, 165–171. [Google Scholar] [CrossRef]
- Gospodaryov, D.V.; Lushchak, V. Oxidative stress: Cause and consequence of diseases. In Oxidative Stress and Diseases, 1st ed.; Lushchak, V., Ed.; InTech: Rijeka, Croatia, 2012; Volume 1, pp. 13–38. [Google Scholar]
- Hisatome, I.; Li, P.; Miake, J.; Taufiq, F.; Mahati, E.; Maharani, N.; Utami, S.B.; Kuwabara, M.; Bahrudin, U.; Ninomiya, H. Uric Acid as a Risk Factor for Chronic Kidney Disease and Cardiovascular Disease—Japanese Guideline on the Management of Asymptomatic Hyperuricemia. Circ. J. 2020, 85, 130–138. [Google Scholar] [CrossRef]
- Lindman, B.R.; Dávila-Román, V.G.; Mann, D.L.; McNulty, S.; Semigran, M.J.; Lewis, G.D.; de las Fuentes, L.; Joseph, S.M.; Vader, J.; Hernandez, A.F.; et al. Cardiovascular Phenotype in HFpEF Patients with or without Diabetes: A RELAX Trial Ancillary Study. J. Am. Coll. Cardiol. 2014, 64, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Bendayan, D.; Shitrit, D.; Ygla, M.; Huerta, M.; Fink, G.; Kramer, M.R. Hyperuricemia as a Prognostic Factor in Pulmonary Arterial Hypertension. Respir. Med. 2003, 97, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Korkmaz, A.; Ozlu, T.; Ozsu, S.; Kazaz, Z.; Bulbul, Y. Long-Term Outcomes in Acute Pulmonary Thromboembolism: The Incidence of Chronic Thromboembolic Pulmonary Hypertension and Associated Risk Factors. Clin. Appl. Thromb. Hemost. 2012, 18, 281–288. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; Cook, S.; Choi, H.K. Serum Concentrations of Uric Acid and the Metabolic Syndrome among US Children and Adolescents. Circulation 2007, 115, 2526–2532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartziokas, K.; Papaioannou, A.I.; Haniotou, A.; Nena, E.; Kostikas, K.; Steiropoulos, P. Serum Uric Acid and Arterial Lactate Levels in Patients with Obstructive Sleep Apnea Syndrome: The Effect of CPAP Treatment. Postgrad. Med. 2021, 133, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Ioachimescu, A.G.; Brennan, D.M.; Hoar, B.M.; Hazen, S.L.; Hoogwerf, B.J. Serum Uric Acid Is an Independent Predictor of All-Cause Mortality in Patients at High Risk of Cardiovascular Disease: A Preventive Cardiology Information System (PreCIS) Database Cohort Study. Arthritis Rheum. 2008, 58, 623–630. [Google Scholar] [CrossRef]
- Warwick, G.; Thomas, P.S.; Yates, D.H. Biomarkers in Pulmonary Hypertension. Eur. Respir. J. 2008, 32, 503–512. [Google Scholar] [CrossRef]
- Garcia-Pachon, E.; Padilla-Navas, I.; Shum, C. Serum Uric Acid to Creatinine Ratio in Patients with Chronic Obstructive Pulmonary Disease. Lung 2007, 185, 21–24. [Google Scholar] [CrossRef]
- DurmusKocak, N.; Sasak, G.; Aka Akturk, U.; Akgun, M.; Boga, S.; Sengul, A.; Gungor, S.; Arinc, S. Serum Uric Acid Levels and Uric Acid/Creatinine Ratios in Stable Chronic Obstructive Pulmonary Disease (COPD) Patients: Are These Parameters Efficient Predictors of Patients at Risk for Exacerbation and/or Severity of Disease? Med. Sci. Monit. 2016, 22, 4169–4176. [Google Scholar] [CrossRef]
- Rumora, L.; Hlapčić, I.; Popović-Grle, S.; Rako, I.; Rogić, D.; Čepelak, I. Uric Acid and Uric Acid to Creatinine Ratio in the Assessment of Chronic Obstructive Pulmonary Disease: Potential Biomarkers in Multicomponent Models Comprising IL-1beta. PLoS ONE 2020, 15, e0234363. [Google Scholar] [CrossRef]
- Tao, J.; Shen, X.; Li, J.; Cha, E.; Gu, P.P.; Liu, J.; Zhu, W.; He, L.L.; Li, G.Q.; Wang, Z. Serum Uric Acid to Creatinine Ratio and Metabolic Syndrome in Postmenopausal Chinese Women. Medicine 2020, 99, e19959. [Google Scholar] [CrossRef]
- Li, M.; Gu, L.; Yang, J.; Lou, Q. Serum Uric Acid to Creatinine Ratio Correlates with β-Cell Function in Type 2 Diabetes. Diabetes. Metab. Res. Rev. 2018, 34, e3001. [Google Scholar] [CrossRef] [PubMed]
- Aujesky, D.; Obrosky, D.S.; Stone, R.A.; Auble, T.E.; Perrier, A.; Cornuz, J.; Roy, P.-M.; Fine, M.J. Derivation and Validation of a Prognostic Model for Pulmonary Embolism. Am. J. Respir. Crit. Care Med. 2005, 172, 1041–1046. [Google Scholar] [CrossRef]
- Jiménez, D.; Aujesky, D.; Moores, L.; Gómez, V.; Lobo, J.L.; Uresandi, F.; Otero, R.; Monreal, M.; Muriel, A.; Yusen, R.D. Simplification of the Pulmonary Embolism Severity Index for Prognostication in Patients with Acute Symptomatic Pulmonary Embolism. Arch. Intern. Med. 2010, 170, 1383–1389. [Google Scholar] [CrossRef] [Green Version]
- Numa, S.; Hirai, T.; Nakagawa, K.; Ohara, K.; Fukuda, N.; Nozawa, T.; Inoue, H. Hyperuricemia and Transesophageal Echocardiographic Thromboembolic Risk in Patients with Atrial Fibrillation at Clinically Low-Intermediate Risk. Circ. J. 2014, 78, 1600–1605. [Google Scholar] [CrossRef] [Green Version]
- Babaoglu, E.; Hasanoglu, H.C.; Senturk, A.; Karalezli, A.; Kilic, H.; Aykun, G.; Oztuna, D. Importance of Biomarkers in Risk Stratification of Pulmonary Thromboembolism Patients. J. Investig. Med. 2014, 62, 328–331. [Google Scholar] [CrossRef]
- Akbar, S.R.; Long, D.M.; Hussain, K.; Alhajhusain, A.; Ahmed, U.S.; Iqbal, H.I.; Ali, A.W.; Leonard, R.; Dalton, C. Hyperuricemia: An Early Marker for Severity of Illness in Sepsis. Int. J. Nephrol. 2015, 2015, 301021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolliscroft, J.O.; Colfer, H.; Fox, I.H. Hyperuricemia in Acute Illness: A Poor Prognostic Sign. Am. J. Med. 1982, 72, 58–62. [Google Scholar] [CrossRef]
- Voelkel, M.A.; Wynne, K.M.; Badesch, D.B.; Groves, B.M.; Voelkel, N.F. Hyperuricemia in Severe Pulmonary Hypertension. Chest 2000, 117, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, Y.; Nagaya, N.; Satoh, T.; Uematsu, M.; Kyotani, S.; Sakamaki, F.; Nakanishi, N.; Miyatake, K. Serum Uric Acid Level Increases in Proportion to the Severity of Pulmonary Thromboembolism. Circ. J. 2002, 66, 571–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozsu, S.; Çoşar, A.M.; Aksoy, H.B.; Bülbül, Y.; Oztuna, F.; Karahan, S.C.; Ozlu, T. Prognostic Value of Uric Acid for Pulmonary Thromboembolism. Respir. Care 2017, 62, 1091–1096. [Google Scholar] [CrossRef] [Green Version]
- Bartziokas, K.; Papaioannou, A.I.; Loukides, S.; Papadopoulos, A.; Haniotou, A.; Papiris, S.; Kostikas, K. Serum Uric Acid as a Predictor of Mortality and Future Exacerbations of COPD. Eur. Respir. J. 2014, 43, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Hare, J.M.; Johnson, R.J. Uric Acid Predicts Clinical Outcomes in Heart Failure: Insights Regarding the Role of Xanthine Oxidase and Uric Acid in Disease Pathophysiology. Circulation 2003, 107, 1951–1953. [Google Scholar] [CrossRef] [Green Version]
- Țăpoi, L.; Șalaru, D.L.; Sascău, R.; Stătescu, C. Uric Acid-An Emergent Risk Marker for Thrombosis? J. Clin. Med. Res. 2021, 10, 1951–1953. [Google Scholar] [CrossRef]
- Pugliese, N.R.; Mengozzi, A.; Virdis, A.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; Rivasi, G.; Salvetti, M.; Barbagallo, C.M.; et al. The Importance of Including Uric Acid in the Definition of Metabolic Syndrome When Assessing the Mortality Risk. Clin. Res. Cardiol. 2021, 110, 1073–1082. [Google Scholar] [CrossRef]
- Casiglia, E.; Tikhonoff, V.; Virdis, A.; Masi, S.; Barbagallo, C.M.; Bombelli, M.; Bruno, B.; Cicero, A.F.G.; Cirillo, M.; Cirillo, P.; et al. Serum Uric Acid and Fatal Myocardial Infarction: Detection of Prognostic Cut-off Values: The URRAH (Uric Acid Right for Heart Health) Study. J. Hypertens. 2020, 38, 412–419. [Google Scholar] [CrossRef]
- Zhang, X.; Hu, M.; Wang, X.; Zhang, C.; Chen, W.; Chen, S.; Zhou, J.; Chen, Y.; Lou, L.; Chen, G.; et al. New Perspective on the Risk Markers for Left Atrial Thrombosis in Patients with Atrial Fibrillation. Eur. J. Prev. Cardiol. 2020, 28, 641–647. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 116) | UA/Create < 7.636 (n = 61) | UA/Create ≥ 7.636 (n = 55) | p |
|---|---|---|---|---|
| Demographic Factors | ||||
| Age, mean ± SD, years | 53.47 ± 7.87 | 54.48 ± 7.32 | 52.35 ± 8.37 | 0.132 |
| Male sex, n (%) | 45 (38.8) | 23 (37.7) | 22 (39.9) | 1.000 |
| Clinical Parameters | ||||
| SBP, median (IQR) | 135 (120–140) | 137 (128–146) | 135 (120–140) | 0.091 |
| Heart Rate, median (IQR) | 100 (95–105) | 100 (97–106) | 101 (92–106) | 0.956 |
| Respiratory Rate, median (IQR) | 28 (21–31) | 21(18.5–23.5) | 31(30–32) | <0.001 |
| Comorbidities, n (%) | ||||
| Malignancy | 27 (23.2) | 11 (18.1) | 16 (29.1) | 0.190 |
| Thrombophilia | 21 (18.1) | 12 (19.7) | 9 (16.3) | 0.470 |
| DVT symptoms | 29 (25) | 17 (27.8) | 12 (21.8) | 0.286 |
| Cardiopulmonary disease | 33 (28.4) | 8 (13.1) | 22 (39.9) | 0.004 |
| Laboratory Biomarkers, median (IQR) | ||||
| Ua/Cr | 7.59 (6.34–9.35) | 6.40 (5.61–7.12) | 9.5 (8.12–10.61) | <0.001 |
| UA, mg/dL | 6.8 (6.4–7.87) | 6.5 (6.1–6.9) | 7.7 (6.9–8.5) | <0.001 |
| D-dimers, ng/mL | 475 (350–720) | 380 (300–640) | 520 (390–740) | 0.013 |
| Oxygen saturation (%) | 91 (88–93) | 91 (88–93) | 90 (87–93) | 0.987 |
| PaO2, mm Hg | 73 (70–75) | 73 (70–75.5) | 73 (71.7–74.7) | 0.640 |
| PaCO2, mm Hg | 36 (33.4–38.6) | 34.3 (32.1–36.4) | 37.9 (34.8–38.2) | <0.001 |
| Lactic acid, mmol/L | 1.73 (1.72–1.77) | 1.73 (1.72–1.74) | 1.74 (1.73–1.78) | 0.002 |
| WBC χ103/μL | 9.9 (8.94–12.5) | 9.9 (8.8–12.06) | 10.1 (9–12.97) | 0.437 |
| Platelets χ103/μL | 365 (295–457) | 370 (300–467) | 359 (280–447) | 0.617 |
| CRP, mg/dL | 68 (12–100) | 54 (11–87) | 78 (14–138) | 0.180 |
| Na mEq/L | 138 (135–140) | 138 (136–139) | 137 (134–139) | 0.122 |
| HSTPN, pg/mL | 20 (14–40) | 31 (14–45) | 17 (14–29) | <0.001 |
| Pulmonary Embolism Classification Tools | ||||
| ESC 2019 algorithm | ||||
| Low, n (%) | 18 (15.5) | 17 (27.9) | 1 (1.8) | <0.001 |
| Intermediate-low, n (%) | 55 (47.4) | 39 (63.9) | 16 (29.1) | <0.001 |
| Intermediate-high, n (%) | 35 (30.2) | 5 (8.2) | 30 (54.5) | <0.001 |
| High, n (%) | 8 (6.9) | 0 (0) | 8 (13.8) | 0.002 |
| PESI, median (IQR) | 113 (70–144) | 76 (62–88) | 144 (126–161) | <0.001 |
| sPESI, median (IQR) | 1 (0–1) | 1 (0–1) | 1 (1–2) | 0.019 |
| sPESI risk, high, n (%) | 85 (73.2) | 37 (60.6) | 48 (87.2) | 0.001 |
| Total | UA/Create < 7.636 | UA/Create ≥ 7.636 | p | |
|---|---|---|---|---|
| Subjects, n | 116 | 61 | 55 | |
| Hospitalization days, median (IQR) | 6 (5–8) | 6 (5.5–8.5) | 7 (5–11) | 0.003 |
| Mortality, n (%) | 17 (14.6) | 2 (3.2) | 15 (27.3) | <0.001 |
| Thrombolysis, n (%) | 14 (12) | 1 (1.6) | 13 (23.6) | <0.001 |
| Composite outcome, n (%) | 20 (17.2) | 2 (3.4) | 18 (32.7) | <0.001 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variables | HR (95% CI) | Beta | p | HR (95% CI) | Beta | p |
| Age | 0.002 (−0.085–0.090) | 0.004 | 0.962 | |||
| Μale | 1.135 (−0.258–2.528) | 0.15 | 0.109 | |||
| Malignancy | 2.199 (0.627–3.772) | 0.251 | 0.007 | 1.373 (−0.416–3.162) | 0.157 | 0.131 |
| RV dysfunction | 1.875 (0.542–3.209) | 0.252 | 0.006 | 0.723 (−1.100–2.546) | 0.097 | 0.433 |
| Cardiopulmonary disease | 0.260 (−1.261–1.780) | 0.032 | 0.736 | |||
| Heart rate | −0.030 (−0.114–0.055) | −0.065 | 0.490 | |||
| Respiratory rate | 0.108 (−0.010–0.226) | 0.168 | 0.071 | −0.154 (−0.343–0.036) | −0.239 | 0.11 |
| SBP | −0.029 (−0.069–0.010) | −0.136 | 0.144 | |||
| Oxygen saturation | 0.044 (−0.105–0.194) | 0.055 | 0.558 | |||
| PaCO2 | 0.137 (−0.091–0.365) | 0.111 | 0.237 | |||
| WBC | 0.001 (0.000–0.001) | 0.412 | <0.001 | 0.001 (0.000–0.001) | 0.35 | <0.001 |
| Na | −0.257 (−0.503–−0.012) | −0.191 | 0.04 | 0.103 (−0.163–0.369) | 0.076 | 0.444 |
| Hs TPNI | −0.012 (−0.052–0.027) | −0.057 | 0.545 | |||
| CRP | 0.008 (0.000–0.015) | 0.192 | 0.039 | 0.003 (−0.005–0.010) | 0.064 | 0.507 |
| Platelets | −0.006 (−0.011–−0.001) | −0.207 | 0.026 | −0.001 (0.000–0.000) | −0.258 | 0.002 |
| UA/Creat | 0.574 (0.316–0.831) | 0.382 | <0.001 | 0.598 (0.209–0.987) | 0.398 | 0.003 |
| PESI score | 0.024 (0.008–0.039) | 0.275 | 0.003 | 0.006 (−0.021–0.034) | 0.006 | 0.652 |
| sPESI score | 0.971 (−0.570–2.512) | 0.116 | 0.214 | |||
| ESC Risk Classification | 1.152 (0.329–1.975) | 0.251 | 0.006 | 0.190 (−1.042–1.421) | 0.041 | 0.761 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variables | HR (95% CI) | Beta | p | HR (95% CI) | Beta | p |
| Age | 0.974 (0.910–1.042) | 0.026 | 0.444 | |||
| Male | 0.890 (0.312–2.536) | −0.117 | 0.827 | |||
| Malignancy | 0.145 (0.048–0.435) | −1.930 | 0.001 | 0.110 (0.026–0.470) | −2.206 | 0.003 |
| RV dysfunction | 0.204 (0.057–0.777) | −1.561 | 0.019 | 1.006 (0.034–29.614) | 0.006 | 0.997 |
| Cardiopulmonary disease | 1.346 (0.405–4.476) | 0.297 | 0.627 | |||
| Heart rate | 1.008(0.946–1.074) | 0.008 | 0.806 | |||
| Respiratory rate | 1.166 (1.038–1.311) | 0.154 | 0.010 | 0.873 (0.679–1.123) | −0.136 | 0.291 |
| SBP | 0.981 (0.952–1.010) | −0.019 | 0.200 | |||
| Oxygen saturation | 0.990 (0.888–1.103) | −0.011 | 0.849 | |||
| PaCO2 | 1.467 (1.158–1.858) | 0.383 | 0.001 | 1.172 (0.859–1.597) | 0.158 | 0.316 |
| WBC | 1.000 (1.000–1.001) | 0.0003 | 0.004 | 1.000 (1.000–1.001) | 0.001 | 0.222 |
| Na | 0.658 (0.528–0.821) | −0.418 | <0.001 | 1.122 (0.766–1.642) | 0.115 | 0.555 |
| HSTPNI | 1.002 (0.973–1.032) | 0.002 | 0.894 | |||
| CRP | 1.008 (1.003–1.013) | 0.008 | 0.001 | 1.009 (1.002–1.015) | 0.009 | 0.007 |
| Platelets | 1.000 (1.000–1.001) | 0.001 | 0.120 | |||
| UA/Cr | 1.575 (1.264–1.963) | 0.454 | <0.001 | 1.620 (1.245–2.108) | 0.482 | <0.001 |
| PESI score | 1.020 (1.006–1.033) | 0.020 | 0.003 | 0.999 (0.965–1.034) | −0.001 | 0.951 |
| sPESI score | 1.577 (0.865–2.874) | 0.455 | 0.137 | |||
| ESC Risk Classification | 3.559 (1.696–7.469) | 1.269 | 0.001 | 2.215 (0.510–9.618) | 0.795 | 0.289 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variables | HR (95% CI) | Beta | p | HR (95% CI) | Beta | p |
| Age | 0.995 (0.935–1.058) | −0.005 | 0.868 | |||
| Male | 0.733 (0.277–1.940) | −0.310 | 0.532 | |||
| Malignancy | 0.215 (0.078–0.597) | −1.536 | 0.003 | 0.214 (0.062–0.735) | −1.540 | 0.014 |
| RV dysfunction | 0.162 (0.045–0.590) | −1.818 | 0.006 | 1.915 (0.162–22.627) | −0.650 | 0.606 |
| Cardiopulmonary disease | 0.913 (0.318–2.622) | −0.091 | 0.866 | |||
| Heart rate | 0.976 (0.919–1.036) | −0.025 | 0.421 | |||
| Respiratory rate | 1.179 (1.054–1.317) | 0.164 | 0.004 | 0.926 (0.770–1.112) | −0.077 | 0.411 |
| SBP | 0.992 (0.965–1.020) | −0.008 | 0.558 | |||
| Oxygen saturation | 1.013 (0.908–1.131) | 0.013 | 0.811 | |||
| PaCO2 | 1.416 (1.148–1.746) | 0.348 | 0.001 | 1.123 (0.877–1.439) | 0.116 | 0.357 |
| WBC | 1.000 (1.000–1.001) | 0.001 | 0.012 | 1.000 (0.998–1.002) | 0.001 | 0.178 |
| Na | 0.703 (0.577–0.856) | −0.353 | <0.001 | 1.067 (0.790–1.844) | 0.065 | 0.673 |
| HSTPNI | 1.015 (0.988–1.042) | 0.014 | 0.283 | |||
| CRP | 1.007 (1.003–1.012) | 0.007 | 0.002 | 1.007 (1.001–1.012) | 0.007 | 0.013 |
| Platelets | 1.000 (1.000–1.000) | 0.000 | 0.199 | |||
| UA/Cr | 1.537 (1.248–1.894) | 0.430 | <0.001 | 1.521 (1.211–1.908) | 0.419 | <0.001 |
| PESI score | 1.022 (1.009–1.035) | 0.021 | 0.001 | 1.001 (0.973–1.030) | 0.001 | 0.951 |
| sPESI score | 1.491 (0.846–2.627) | 0.399 | 0.167 | |||
| ESC Risk Classification | 3.926 (1.899–8.117) | 1.368 | <0.001 | 2.100 (0.822–5.365) | 0.742 | 0.121 |
| 30-Day Mortality | Composite Outcome | |
|---|---|---|
| Predictors | AUC (95% CI) | AUC (95% CI) |
| PESI score | 0.734 (0.621–0.847) | 0.753 (0.651–0.855) |
| PESI score, class I–V | 0.738 (0.629–0.847) | 0.763 (0.664–0.861) |
| sPESI score | 0.622 (0.496–0.748) | 0.611 (0.495–0.727) |
| sPESI score, class 0–1 | 0.622 (0.495–0.749) | 0.631(0.513–0.749) |
| ESC 2019 Risk Classification | 0.774 (0.670–0.877) | 0.791 (0.697–0.884) |
| UA/Cr | 0.793 (0.667–0.918) | 0.793 (0.684–0.902) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartziokas, K.; Kyriakopoulos, C.; Potonos, D.; Exarchos, K.; Gogali, A.; Kostikas, K. The Diagnostic Role of Uric Acid to Creatinine Ratio for the Identification of Patients with Adverse Pulmonary Embolism Outcomes. Diagnostics 2022, 12, 193. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010193
Bartziokas K, Kyriakopoulos C, Potonos D, Exarchos K, Gogali A, Kostikas K. The Diagnostic Role of Uric Acid to Creatinine Ratio for the Identification of Patients with Adverse Pulmonary Embolism Outcomes. Diagnostics. 2022; 12(1):193. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010193
Chicago/Turabian StyleBartziokas, Konstantinos, Christos Kyriakopoulos, Dimitrios Potonos, Konstantinos Exarchos, Athena Gogali, and Konstantinos Kostikas. 2022. "The Diagnostic Role of Uric Acid to Creatinine Ratio for the Identification of Patients with Adverse Pulmonary Embolism Outcomes" Diagnostics 12, no. 1: 193. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010193