
Clinical Profile of 24 AIDS Patients with Cryptococcal Meningitis in the HAART Era: A Report from an Infectious Diseases Tertiary Hospital in Western Romania


 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spadari, C.d.C.; Wirth, F.; Lopes, L.B.; Ishida, K. New approaches for cryptococcosis treatment. Microorganisms 2020, 8, 613. [Google Scholar] [CrossRef]
- Park, B.J.; Wannemuehler, K.A.; Marston, B.J.; Govender, N.; Pappas, P.G.; Chiller, T.M. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 2009, 23, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Situational Analysis. World AIDS Day. Available online: https://www.dsptimis.ro/promovare/zml_hiv_19_analiza.pdf2018 (accessed on 14 March 2021).
- Comisia Națională de Luptă Anti-SIDA–Date Statistice. Evoluția Infecției HIV/SIDA în România. 31 Decembrie 2017. Available online: http://cnlas.ro/images/doc/31122017_rom.pdf2017 (accessed on 14 March 2021).
- Montoya, M.C.; Magwene, P.M.; Perfect, J.R. Associations between Cryptococcus genotypes, phenotypes, and clinical parameters of human disease: A review. J. Fungi 2021, 7, 260. [Google Scholar] [CrossRef]
- Bicanic, T.; Brouwer, A.E.; Meintjes, G.; Rebe, K.; Limmathurotsakul, D.; Chierakul, W.; Teparrakkul, P.; Loyse, A.; White, N.J.; Wood, R.; et al. Relationship of cerebrospinal fluid pressure, fungal burden and outcome in patients with cryptococcal meningitis undergoing serial lumbar punctures. AIDS 2009, 23, 701–706. [Google Scholar] [CrossRef]
- Bicanic, T.; Harrison, T.S. Cryptococcal meningitis. Br. Med. Bull. 2004, 72, 99–118. [Google Scholar] [CrossRef] [Green Version]
- CDC. Preventing Deaths from Cryptococcal Meningitis. 2020. Available online: https://www.cdc.gov/fungal/cdc-and-fungal/cryptococcal-meningitis.html (accessed on 19 May 2021).
- Skipper, C.; Abassi, M.; Boulware, D.R. Diagnosis and management of central nervous system cryptococcal infections in HIV-infected adults. J. Fungi 2019, 5, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momin, M.; Webb, G. The environmental effects on virulence factors and the antifungal susceptibility of Cryptococcus neoformans. Int. J. Mol. Sci. 2021, 22, 6302. [Google Scholar] [CrossRef]
- Feldmesser, M.; Tucker, S.; Casadevall, A. Intracellular parasitism of macrophages by Cryptococcus neoformans. Trends Microbiol. 2001, 9, 273–278. [Google Scholar] [CrossRef]
- Alanio, A.; Desnos-Ollivier, M.; Dromer, F. Dynamics of Cryptococcus neoformans—Macrophage interactions reveal that fungal background influences outcome during Cryptococcal Meningoencephalitis in humans. mBio 2011, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steenbergen, J.N.; Casadevall, A. Prevalence of Cryptococcus neoformans var. neoformans (Serotype D) and Cryptococcus neoformans var. grubii (Serotype A) Isolates in New York City. J. Clin. Microbiol. 2000, 38, 1974–1976. [Google Scholar] [CrossRef] [Green Version]
- Abassi, M.; Boulware, D.R.; Rhein, J. Cryptococcal Meningitis: Diagnosis and Management Update. Curr. Trop. Med. Rep. 2015, 2, 90–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streinu-Cercel, A.; Săndulescu, O.; Poiană, C.; Dorobanțu, M.; Mircescu, G.; Lăzureanu, V.E.; Dumitru, I.M.; Chirilă, O.; Streinu-Cercel, A.; Extended Consensus Group. Consensus statement on the assessment of comorbidities in people living with HIV in Romania. Germs 2019, 9, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Comisia Națională de Luptă Anti-SIDA–Date Statistice. Evoluția Infecției HIV/SIDA în România. 31 Decembrie 2020. Available online: https://www.cnlas.ro/images/doc/31122020_rom.pdf (accessed on 19 May 2021).
- Guess, T.E.; Rosen, J.A.; McClelland, E.E. An overview of sex bias in C. neoformans infections. J. Fungi 2018, 4, 49. [Google Scholar] [CrossRef] [Green Version]
- Lakshmi, V.; Sudha, T.; Teja, V.D.; Umabala, P. Prevalence of central nervous system cryptococcosis in human immunodeficiency virus reactive hospitalized patients. Indian J. Med. Microbiol. 2007, 25, 146–149. [Google Scholar] [CrossRef]
- Kumar, S.; Wanchu, A.; Chakrabarti, A.; Sharma, A.; Bambery, P.; Singh, S. Cryptococcal meningitis in HIV infected: Experience from a North Indian tertiary center. Neurol. India 2008, 56, 444–449. [Google Scholar] [CrossRef] [Green Version]
- Brizendine, K.D.; Baddley, J.W.; Pappas, P.G. Predictors of mortality and differences in clinical features among patients with Cryptococcosis according to immune status. PLoS ONE 2013, 8, e60431. [Google Scholar] [CrossRef]
- O’Kelly, B.; Mohamed, A.; Bergin, C.; Lyons, F.; Rogers, T.R.; O’Connell, B.; Devitt, E. Successful treatment of Cryptococcal Meningitis and Cryptococcoma with Isavuconazole in a patient living with HIV. J. Fungi 2021, 7, 425. [Google Scholar] [CrossRef]
- Manosuthi, W.; Athichathanabadi, C.; Uttayamakul, S.; Phoorisri, T.; Sungkanuparph, S. Plasma nevirapine levels, adverse events and efficacy of antiretroviral therapy among HIV-infected patients concurrently receiving nevirapine-based antiretroviral therapy and fluconazole. BMC Infect. Dis. 2007, 7, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.D.; Achan, B.; Hullsiek, K.H.; McDonald, T.R.; Okagaki, L.H.; Alhadab, A.A.; Akampurira, A.; Rhein, J.R.; Meya, D.B.; Boulware, D.R.; et al. Increased antifungal drug resistance in clinical isolates of Cryptococcus neoformans in Uganda. Antimicrob. Agents Chemother. 2015, 59, 7197–7204. [Google Scholar] [CrossRef] [Green Version]
- Sungkanuparph, S.; Savetamornkul, C.; Pattanapongpaiboon, W. Primary Prophylaxis for Cryptococcosis with fluconazole in human immunodeficiency virus–infected patients with CD4 T-cell counts < 100 cells/microL and receiving antiretroviral therapy. Clin. Infect. Dis. 2017, 64, 967–970. [Google Scholar] [CrossRef]
- Huang, L.; Ye, H.; Qu, J.; Liu, Y.; Zhong, C.; Tang, G.; Liu, Y.; Huang, Y.; Lv, X. Analysis of cerebrospinal fluid protein concentrations of patients with cryptococcal meningitis treated with antifungal agents. BMC Infect. Dis. 2015, 15, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajasingham, R.; Meya, D.B.; Greene, G.S.; Jordan, A.; Nakawuka, M.; Chiller, T.M.; Boulware, D.R.; Larson, B.A. Evaluation of a national cryptococcal antigen screening program for HIV-infected patients in Uganda: A cost-effectiveness modeling analysis. PLoS ONE 2019, 14, e0210105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perfect, J.R.; Dismukes, W.E.; Dromer, F.; Goldman, D.L.; Graybill, J.R.; Hamill, R.J.; Harrison, T.S.; Larsen, R.A.; Lortholary, O.; Nguyen, M.H.; et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of America. Clin. Infect. Dis. 2010, 50, 291–322. [Google Scholar] [CrossRef] [Green Version]
- Graybill, J.R.; Sobel, J.; Saag, M.; van Der Horst, C.; Powderly, W.; Cloud, G.; Riser, L.; Hamill, R.; Dismukes, W.; NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. Clin. Infect. Dis. 2000, 30, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| AIDS Antiretroviral Treatment Regimens | Meningitis Treatment |
|---|---|
| Regimen 1: abacavir 600 mg + lamivudin 300 mg once a day | Amphotericin B (0.5–1 mg/kg/day) and oral flucytosine (150 mg/kg/day) for 2 weeks as induction therapy, followed by oral fluconazole (400 mg/day) for 10 weeks treatment, mannitol solution 20% (3 × 250 mL/day), and dexamethasone (4 mg/mL, 4 × 4 mg/day) |
| Regimen 2: lopinavir, ritonavir (Kaletra) 200 mg/50 mg; tabs, 800/200 mg (four 200/50 mg tabs) once daily and lamivudine 150 mg, zidovudine 300 mg; twice daily | |
| Regimen 3: lopinavir, ritonavir (Kaletra) 200 mg/50 mg; tabs, 800/200 mg (four 200/50 mg tabs) once daily, abacavir (Ziagen) tablets (300 mg) twice daily, lamivudine (Epivir) 300 mg tablets, twice daily | |
| Regimen 4: lopinavir, ritonavir (Kaletra) 200 mg/50 mg; tabs, 800/200 mg (four 200/50 mg tabs) once daily, abacavir 600 mg + lamivudine 300 mg (Kivexa) once daily |
| Patient Characteristics | n (Frequency) | Mean ± SD (Range) |
|---|---|---|
| Age | 41.36 ± 6.7 (32–52) | |
| <40 years | 10 (41.7%) | |
| ≥40 | 14 (58.3%) | |
| Gender | ||
| Female | 7 (29.2%) | 42.33 ± 8.5 (36–52) |
| Male | 17 (70.8%) | 41 ± 6.6 (32–51) |
| Area of residence | ||
| Urban | 6 (25.0%) | |
| Rural | 18 (75.0%) | |
| Etiology of HIV | ||
| Blood transfusion | 5 (20.8%) | |
| Sexual contact | 19 (79.2%) | |
| HIV Stage—AIDS | 24 (100%) | |
| Serotype A C.neoformans | 24 (100%) | |
| HIV viral load (thousand copies/µL) | 145 ± 101 (42–1356) | |
| AIDS antiretroviral treatment regimen * | ||
| Regimen 1 | 1 (4.2%) | |
| Regimen 2 | 4 (16.7%) | |
| Regimen 3 | 6 (25.0%) | |
| Regimen 4 | 13 (54.1%) | |
| ICU admission | 6 (25.0%) | |
| Duration of hospitalization (days) | 25.27 ± 11 (14–42) | |
| In-hospital complications | ||
| Acute kidney injury | 3 (12.5%) | |
| ARDS | 3 (12.5%) | |
| Hepatocytolisis syndrome | 2 (8.3%) | |
| Anemia | 3 (12.5%) | |
| Septic shock | 2 (8.3%) | |
| Oral candidiasis | 4 (16.7%) | |
| Tuberculosis | 4 (16.7%) | |
| Nosocomial pneumonia | 2 (8.3%) | |
| Mortality | 8 (33.3%) |
| Variable | Value, Mean ± SD (Range) | |
|---|---|---|
| Serum Profile | WBC (thousands/mm3) | 12.5 ± 4.3 (9–24) |
| Lymphocytes (%) | 13.4 ± 16.9 (4–49) | |
| ESR (mm/h) | 105.7 ± 15.3 (84–131) | |
| CRP (mg/L) | 92.2 ± 116.3 (29–428) | |
| ASTO (<200 Todd units/mL) | 121.1 ± 38.2 (80–200) | |
| Fibrinogen (g/L) | 286.4 ± 71.3 (210–389) | |
| Ht (%) | 26.8 ± 7.1 (11–39) | |
| Hg (g/dL) | 9.2 ± 2.2 (8–13) | |
| AST (U/L) | 191.6 ± 228.4 (12–642) | |
| ALT (U/L) | 217.7 ± 275.9 (9–752) | |
| Creatinine (µmol/L) | 0.60 ± 0.23 (0.22–0.90) | |
| CSF Profile | WBC (thousands/mm3) | 19.2 ± 7.9 (1–30) |
| Protein (g/dL) | 46.2 ± 47.4 (0.48–118.9) | |
| Glucose (mmol/L) | 2.4 ± 0.95 (1.2–4.2) | |
| Lactate (mmol/L) | 19.2 ± 13.1 (3.8–54.6) | |
| Opening pressure (cm H2O) | 21.1 ± 8.8 (8–29) | |
| CD4 (cells/µL) | 24.9 ± 22.1 (9–69) | |
| CD8 (cells/µL) | 162.5 ± 349.3 (29–1215) | |
| CD3 (cells/µL) | 62.6 ± 37.2 (289–154) | |
| CD4/CD8 (cells/µL) | 0.36 ± 0.5 (0–1) |
| Study Variables | Outcome | p-Value | ||
|---|---|---|---|---|
| Died (n = 6) | Survived (n = 18) | |||
| Age group | <40 years (n = 11) | 5 (45.5%) | 6 (54.5%) | 0.033 ₣,* |
| ≥40 years (n = 13) | 1 (7.7%) | 12 (92.3%) | ||
| Gender | Female (n = 7) | 2 (28.5%) | 5 (71.5%) | 0.795 ₣ |
| Male (n = 17) | 4 (23.5%) | 13 (76.5%) | ||
| Area of residence | Urban (n = 6) | 3 (50.0%) | 3 (50.0%) | 0.102 ₣ |
| Rural (n = 18) | 3 (16.6%) | 15 (83.4%) | ||
| HIV transmission | Blood transfusion (n = 5) | 2 (40.0%) | 3 (60.0%) | 0.383 ₣ |
| Sexual contact (n = 19) | 4 (21.0%) | 15 (79.0%) | ||
| HIV viral load (thousand copies/µL) | 158 ± 87 | 139 ± 114 | 0.713 t | |
| AIDS antiretroviral treatment regimen | Regimen 1 (n = 1) | 1 (100%) | 0 (0.0%) | 0.276 χ |
| Regimen 2 (n = 4) | 1 (25.0%) | 3 (75.0%) | ||
| Regimen 3 (n = 6) | 2 (33.3%) | 4 (66.7%) | ||
| Regimen 4 (n = 13) | 2 (15.4%) | 11 (84.6%) | ||
| Serum Profile | WBC (thousands/mm3) | 11.5 (10.3–21) | 10 (9–14) | 0.444 Ư |
| Lymphocytes (%) | 4.5 (4–6) | 8 (5–46) | 0.065 Ư | |
| ESR (mm/h) | 111 ± 11.6 | 102.7 ± 17.1 | 0.415 t | |
| CRP (mg/L) | 79.5 (40.3–344.5) | 35 (34–100) | 0.449 Ư | |
| ASTO (<200 Todd units/mL) | 137.5 ± 53.2 | 111.7 ± 27.1 | 0.305 t | |
| Fibrinogen (g/L) | 283 ± 71.9 | 288.3 ± 76.6 | 0.913 t | |
| Hematocrit (%) | 29.5 (15.5–33) | 26 (23–29) | 0.510 Ư | |
| Hemoglobin (g/dL) | 11 (9.3–12.8) | 9 (8–13) | 0.565 Ư | |
| AST (U/L) | 109 (15.3–205.8) | 94 (25–598) | 0.394 Ư | |
| ALT (U/L) | 88.5 (14.8–181) | 149 (32–741) | 0.298 Ư | |
| Creatinine (µmol/L) | 0.65 ± 0.32 | 0.58 ± 0.19 | 0.665 t | |
| CSF Profile | WBC (thousands/mm3) | 18.8 ± 12.7 | 19.4 ± 4.9 | 0.900 t |
| Protein (g/dL) | 29.2 (3.4–98.5) | 23.8 (14.2–117.9) | 0.450 Ư | |
| Glucose (mmol/L) | 2.3 ± 0.78 | 2.5 ± 1.08 | 0.785 t | |
| Lactate (mmol/L) | 13.9 (5.5–18.6) | 20.9 (14.3–21) | 0.088 Ư | |
| Opening pressure (cm H2O) | 28.3 ± 0.96 | 16.3 ± 8.4 | 0.025 t,* | |
| CD4 (cel/µL) | 33 ± 31.6 | 20.3 ± 15.6 | 0.386 t | |
| CD8 (cel/µL) | 68.5 (53.8–68.5) | 59 (46–62) | 0.256 Ư | |
| CD3 (cel/µL) | 63.5 (31.5) | 49 (34–73) | 0.850 Ư | |
| CD4/CD8 (cel/µL) | 0.53 (0.09–0.97) | 0.10 (0.01–0.26) | 0.053 Ư | |
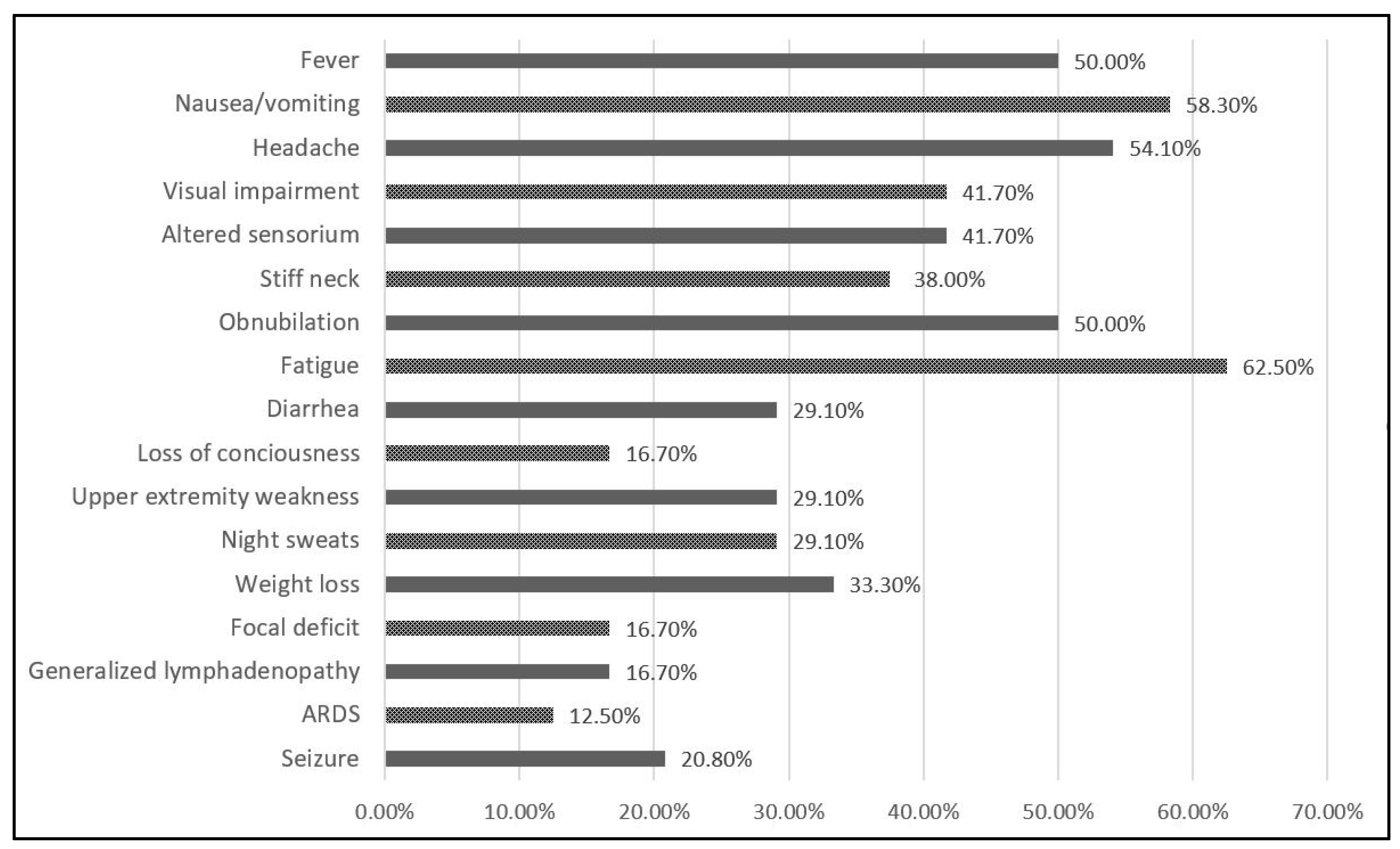
| Sign and symptoms | Fever | 6 (100%) | 6 (33.3%) | 0.004 ₣,* |
| Nausea/vomiting | 6 (100%) | 8 (44.4%) | 0.029 ₣,* | |
| Headache | 5 (83.3%) | 8 (44.4%) | 0.156 ₣ | |
| Visual Impairment | 6 (100%) | 4 (22.2%) | 0.001 ₣,* | |
| Altered sensorium | 5 (83.3%) | 5 (27.8%) | 0.017 ₣,* | |
| Stiff neck | 5 (83.3%) | 4 (22.2%) | 0.013 ₣,* | |
| Fatigue | 6 (100%) | 8 (44.4%) | 0.029 ₣,* | |
| Diarrhea | 4 (66.7%) | 3 (16.7%) | 0.019 ₣,* | |
| Loss of consciousness | 2 (33.3%) | 2 (11.1%) | 0.205 ₣,* | |
| Upper extremity weakness | 4 (66.7%) | 3 (16.7%) | 0.019 ₣,* | |
| Night sweats | 3 (50.0%) | 4 (22.2%) | 0.194 ₣,* | |
| Weight loss | 5 (83.3%) | 3 (16.7%) | 0.002 ₣,* | |
| Focal deficit | 2 (33.3%) | 2 (11.1%) | 0.205 ₣,* | |
| Generalized lymphadenopathy | 3 (50.0%) | 1 (5.6%) | 0.011 ₣,* | |
| Seizure | 4 (66.7%) | 1 (5.6%) | 0.001 ₣,* | |
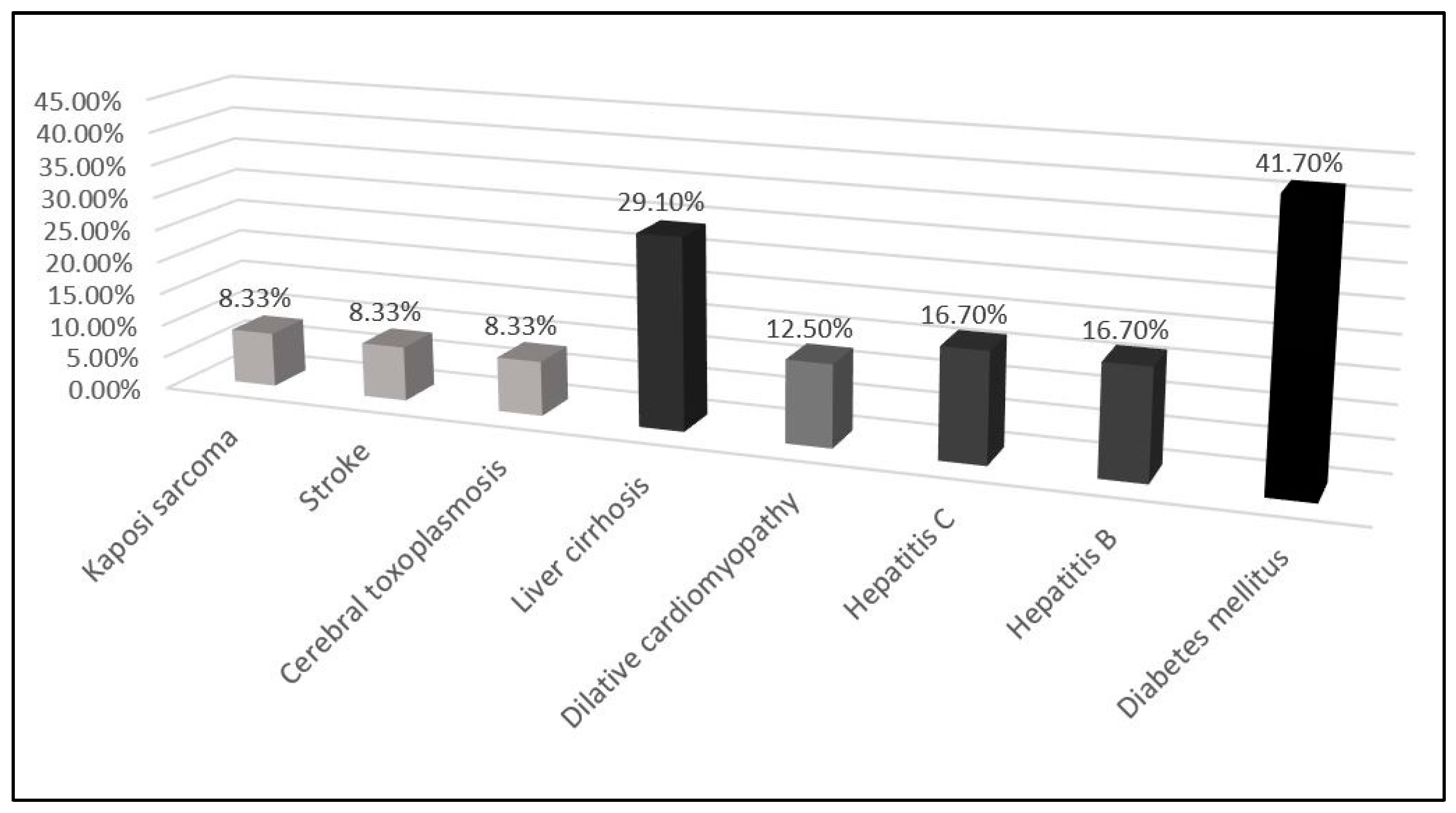
| Comorbidities | Kaposi sarcoma | 2 (33.3%) | 0 (0%) | 0.010 ₣,* |
| Stroke | 1 (16.7%) | 1 (5.6%) | 0.393 ₣ | |
| Cerebral toxoplasmosis | 2 (33.3%) | 0 (0%) | 0.010 ₣,* | |
| Liver cirrhosis | 4 (66.7%) | 3 (16.7%) | 0.019 ₣,* | |
| Dilated cardiomyopathy | 2 (33.3%) | 1 (5.6%) | 0.074 ₣ | |
| Hepatitis C | 3 (50.0%) | 1 (5.6%) | 0.011 ₣,* | |
| Hepatitis B | 2 (33.3%) | 2 (11.1%) | 0.205 ₣ | |
| Altered mental status | 1 (16.7%) | 1 (5.6%) | 0.393 ₣ | |
| Diabetes Mellitus | 6 (100%) | 4 (22.2%) | 0.001 ₣,* | |
| Admitted to ICU | 2 (33.3%) | 1 (5.6%) | 0.074 ₣ | |
| In-hospital complication | Hepatocytolisis syndrome | 1 (16.7%) | 1 (5.6%) | 0.393 ₣ |
| Acute kidney injury | 1 (16.7%) | 1 (5.6%) | 0.393 ₣ | |
| Anemia | 1 (16.7%) | 2 (11.1%) | 0.721 ₣ | |
| Septic shock | 3 (50.0%) | 0 (0%) | 0.001 ₣ | |
| Oral candidiasis | 2 (33.3%) | 1 (5.6%) | 0.074 ₣ | |
| Tuberculosis | 2 (33.3%) | 1 (5.6%) | 0.074 ₣ | |
| Nosocomial pneumonia | 1 (16.7%) | 0 (0%) | 0.076 ₣ | |
| ARDS | 3 (50.0%) | 0 (0.0%) | 0.001 ₣ | |
| Hospital stay (days) | 32 (17.3–41.5) | 19 (16–32) | 0.296 Ư | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marincu, I.; Citu, C.; Vidican, I.; Bratosin, F.; Mares, M.; Suciu, O.; Frent, S.; Bota, A.V.; Timircan, M.; Bratu, M.L.; et al. Clinical Profile of 24 AIDS Patients with Cryptococcal Meningitis in the HAART Era: A Report from an Infectious Diseases Tertiary Hospital in Western Romania. Diagnostics 2022, 12, 54. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010054
Marincu I, Citu C, Vidican I, Bratosin F, Mares M, Suciu O, Frent S, Bota AV, Timircan M, Bratu ML, et al. Clinical Profile of 24 AIDS Patients with Cryptococcal Meningitis in the HAART Era: A Report from an Infectious Diseases Tertiary Hospital in Western Romania. Diagnostics. 2022; 12(1):54. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010054
Chicago/Turabian StyleMarincu, Iosif, Cosmin Citu, Iulia Vidican, Felix Bratosin, Mihai Mares, Oana Suciu, Stefan Frent, Adrian Vasile Bota, Madalina Timircan, Melania Lavinia Bratu, and et al. 2022. "Clinical Profile of 24 AIDS Patients with Cryptococcal Meningitis in the HAART Era: A Report from an Infectious Diseases Tertiary Hospital in Western Romania" Diagnostics 12, no. 1: 54. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010054