
Assessing Putative Markers of Colorectal Cancer Stem Cells: From Colonoscopy to Gene Expression Profiling
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Specimens
2.2. mRNA Extraction
2.3. Assessment of RNA Concentration, Purity and Degradation
2.4. Two Step qRT-PCR
2.5. Reverse-Transcription
2.6. Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR)
2.7. Statistical Analysis
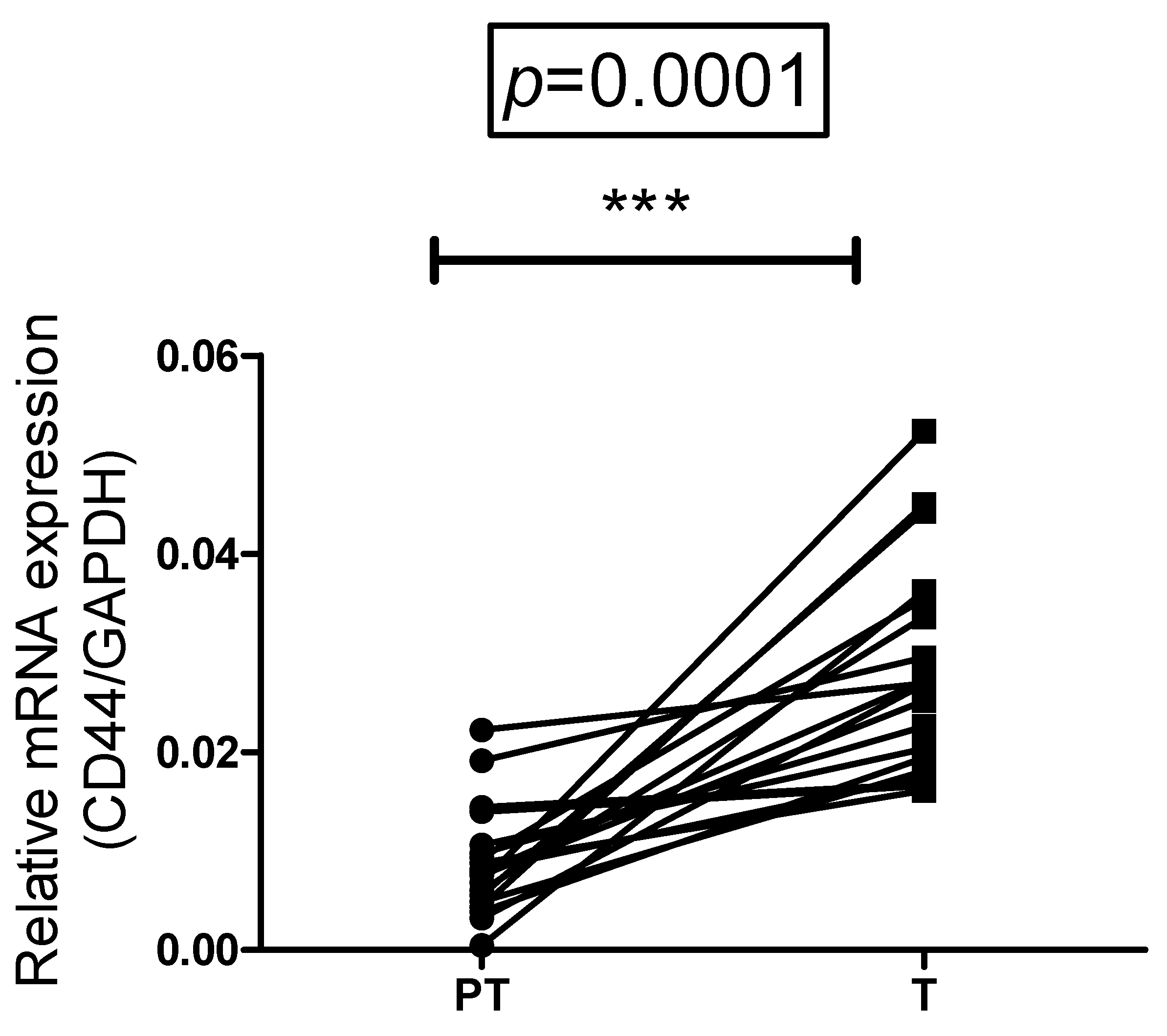
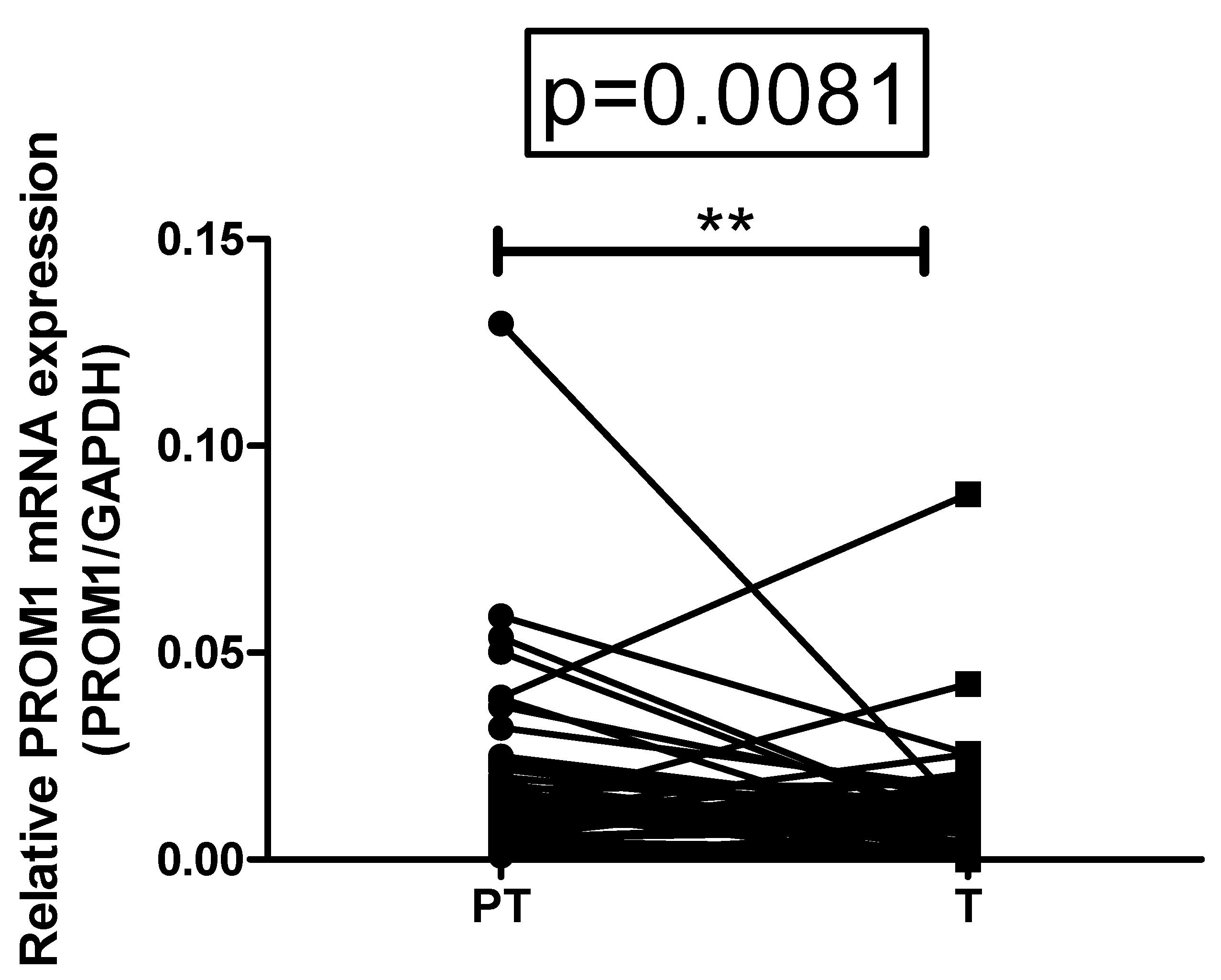
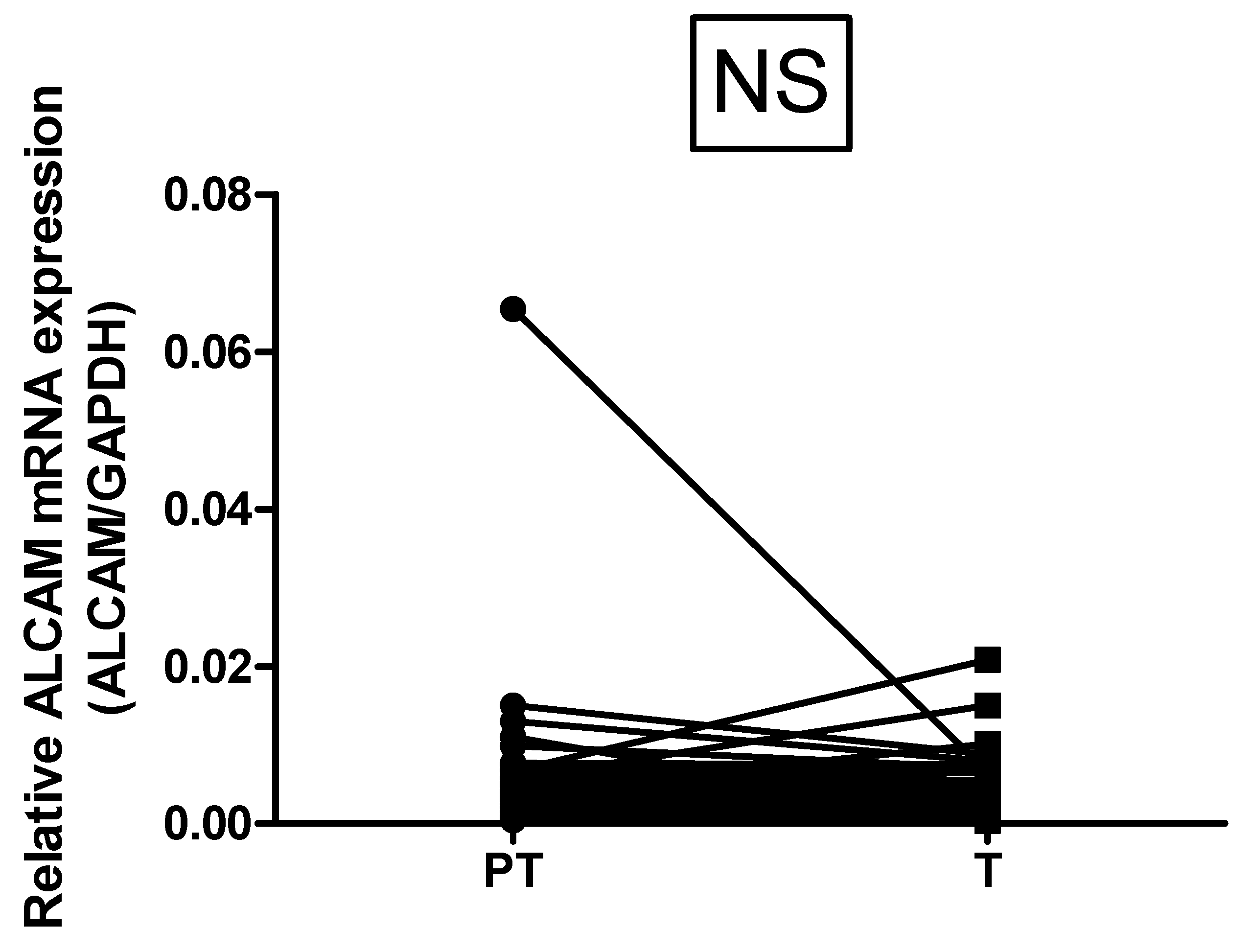
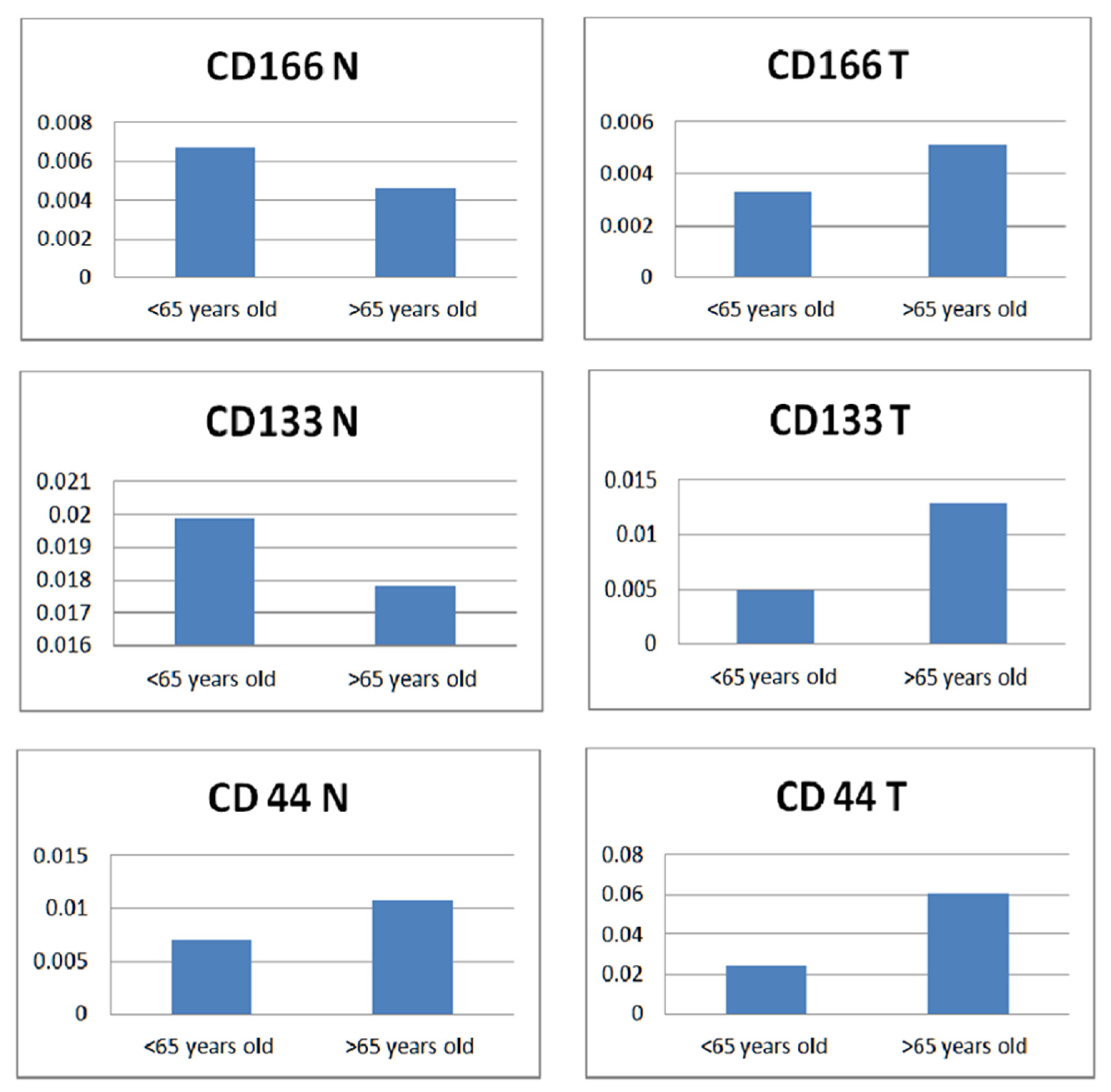
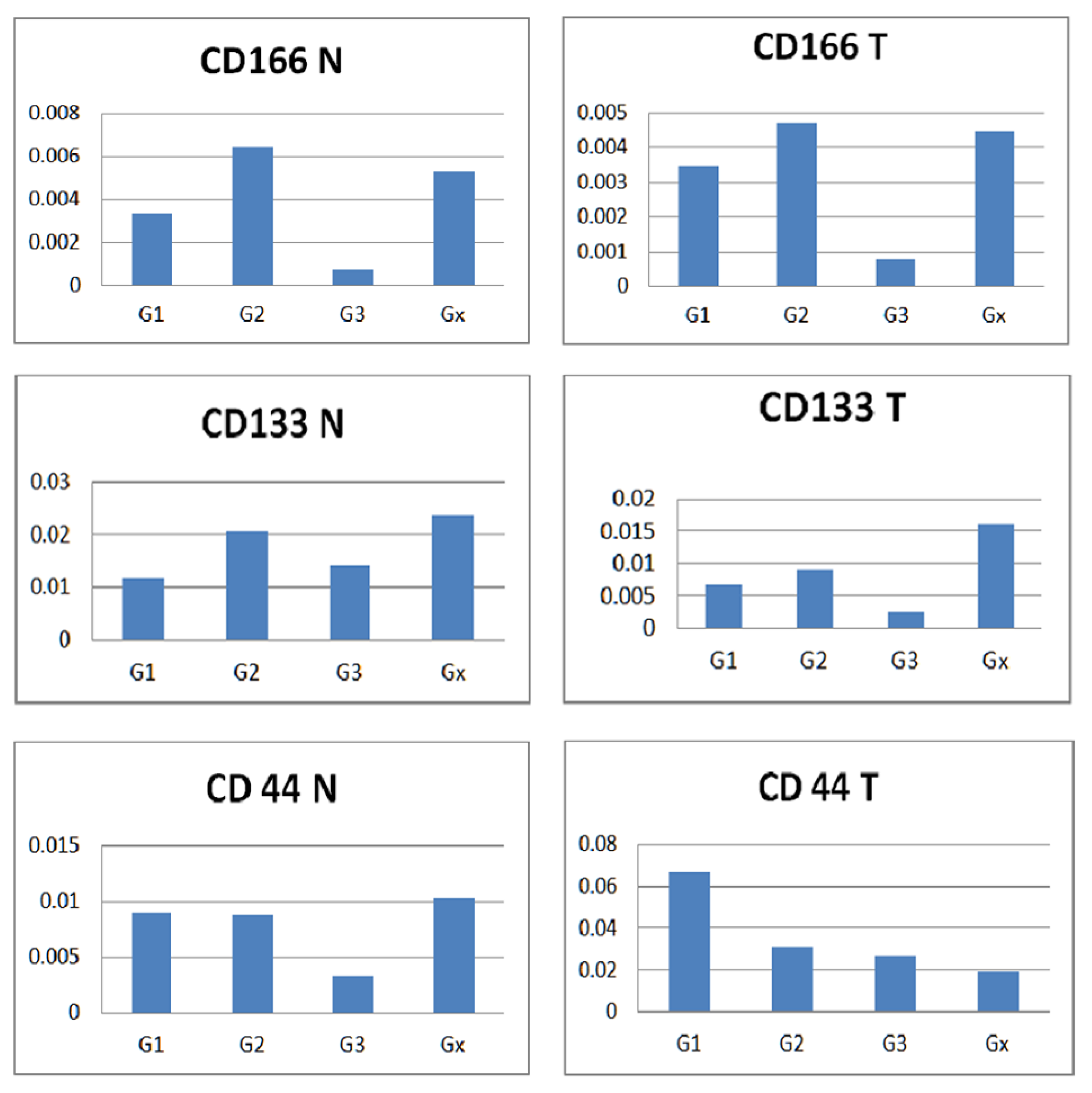
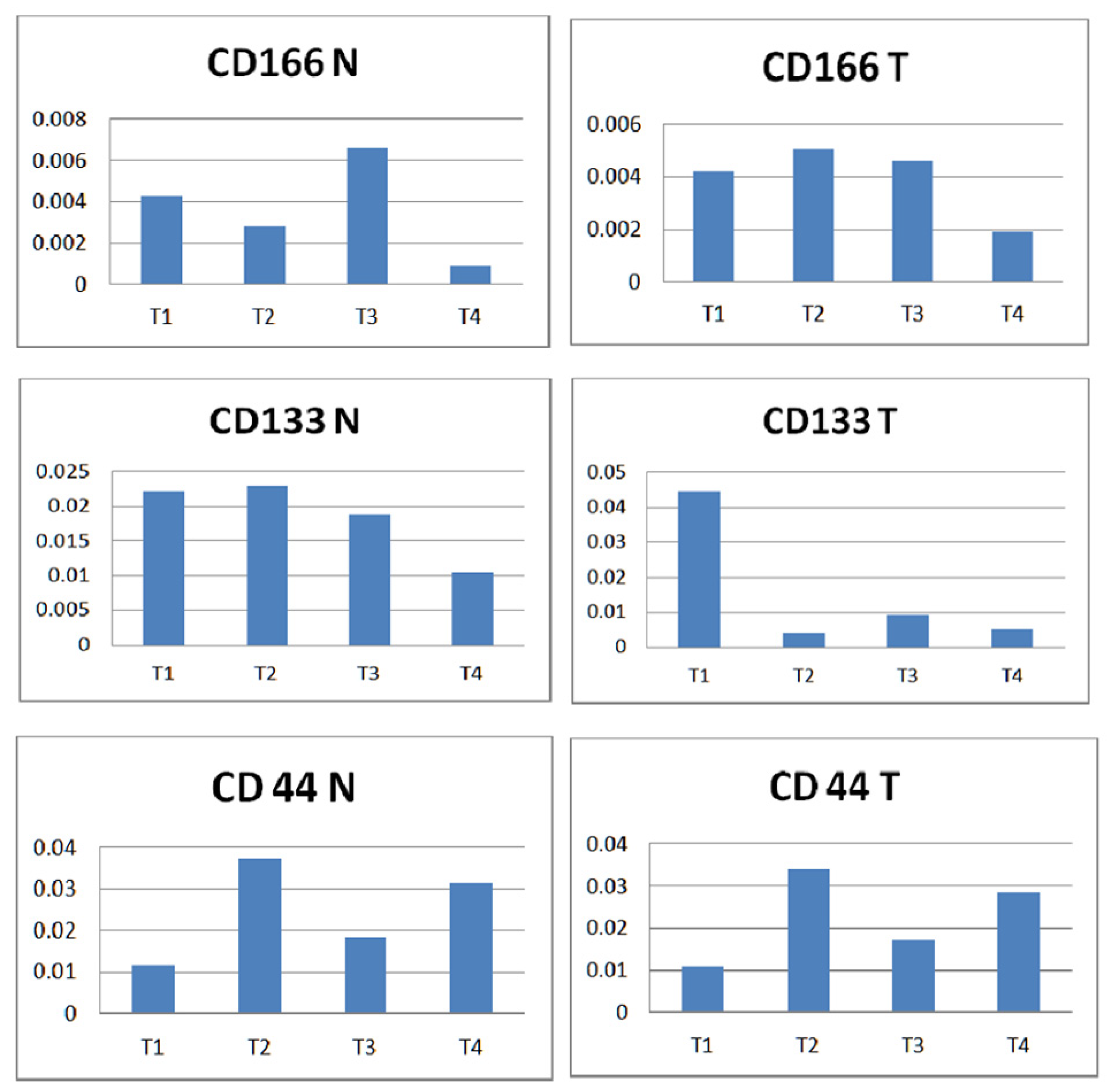
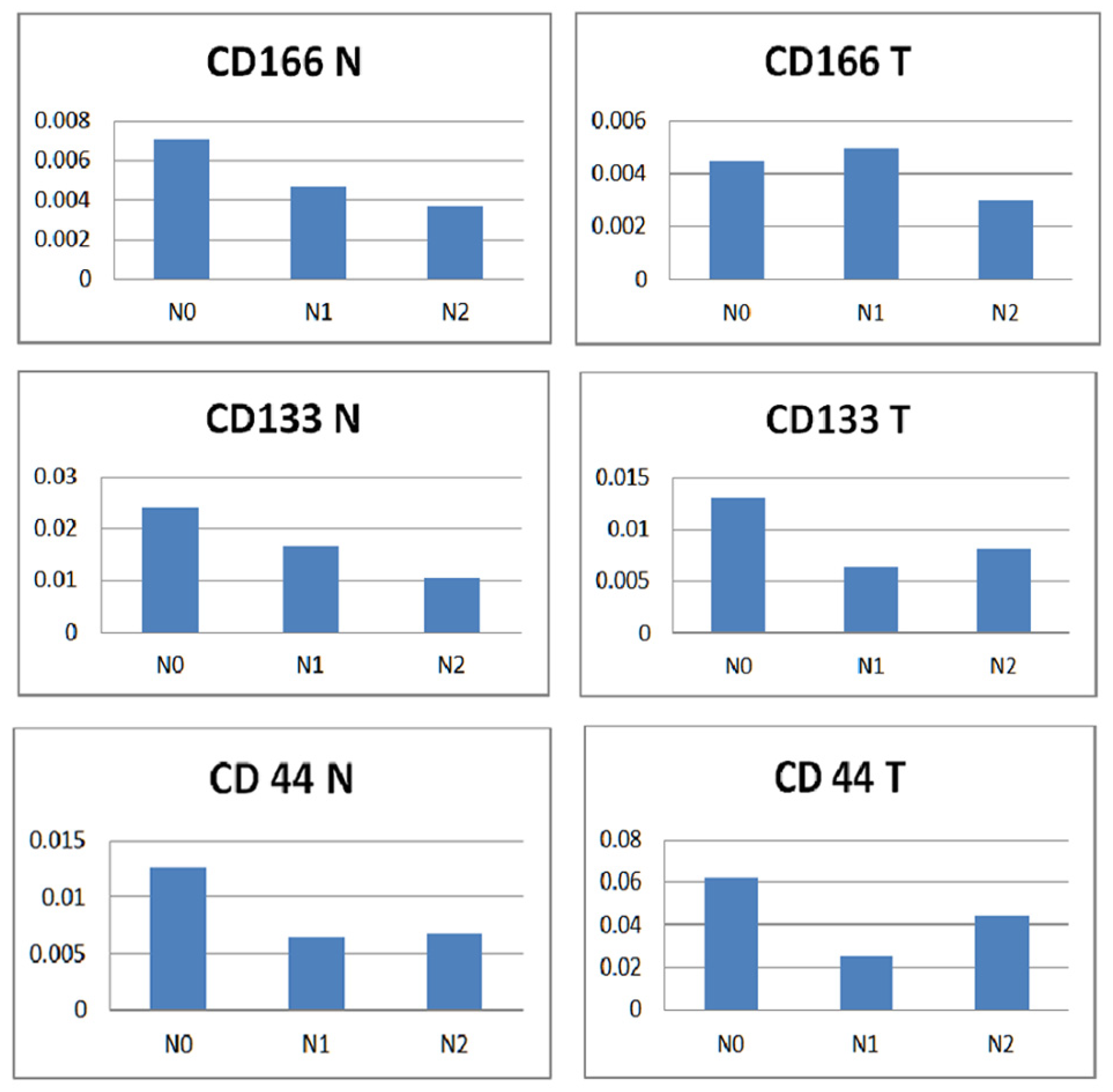
3. Results
4. Discussion
Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guo, M.; Dou, J. Advances and perspectives of colorectal cancer stem cell vaccine. Biomed. Pharmacother. 2015, 76, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Caglar, H.O.; Avci, C.B. Alterations of cell cycle genes in cancer: Unmasking the role of cancer stem cells. Mol. Biol. Rep. 2020, 47, 3065–3076. [Google Scholar] [CrossRef] [PubMed]
- Todaro, M.; Francipane, M.G.; Medema, J.P.; Stassi, G. Colon Cancer Stem Cells: Promise of Targeted Therapy. Gastroenterology 2010, 138, 2151–2162. [Google Scholar] [CrossRef]
- Chen, S.; Huang, E.H. The colon cancer stem cell microenvironment holds keys to future cancer therapy. J. Gastrointest. Surg. 2014, 18, 1040–1048. [Google Scholar] [CrossRef]
- Gangemi, R.; Paleari, L.; Orengo, A.M.; Cesario, A.; Chessa, L.; Ferrini, S.; Russo, P. Cancer stem cells: A new paradigm for understanding tumor growth and progression and drug resistance. Curr. Med. Chem. 2009, 16, 1688–1703. [Google Scholar] [CrossRef]
- Botchkina, G.I.; Zuniga, E.S.; Das, M.; Wang, Y.; Wang, H.; Zhu, S.; Savitt, A.G.; Rowehl, R.A.; Leyfman, Y.; Ju, J.; et al. New-generation taxoid SB-T-1214 inhibits stem cell-related gene expression in 3D cancer spheroids induced by purified colon tumor-initiating cells. Mol. Cancer 2010, 9, 192. [Google Scholar] [CrossRef]
- Ribeiro, K.B.; da Silva Zanetti, J.; Ribeiro-Silva, A.; Rapatoni, L.; de Oliveira, H.F.; da Cunha Tirapelli, D.P.; Garcia, S.B.; Feres, O.; da Rocha, J.J.R.; Peria, F.M. KRAS mutation associated with CD44/CD166 immunoexpression as predictors of worse outcome in metastatic colon cancer. Cancer Biomark. 2016, 16, 513–521. [Google Scholar] [CrossRef]
- Galizia, G.; Gemei, M.; Del Vecchio, L.; Zamboli, A.; Di Noto, R.; Mirabelli, P.; Salvatore, F.; Castellano, P.; Orditura, M.; De Vita, F.; et al. Combined CD133/CD44 expression as a prognostic indicator of disease-free survival in patients with colorectal cancer. Arch. Surg. 2012, 147, 18–24. [Google Scholar] [CrossRef]
- Lugli, A.; Iezzi, G.; Hostettler, I.; Muraro, M.G.; Mele, V.; Tornillo, L.; Carafa, V.; Spagnoli, G.; Terracciano, L.; Zlobec, I. Prognostic impact of the expression of putative cancer stem cell markers CD133, CD166, CD44s, EpCAM, and ALDH1 in colorectal cancer. Br. J. Cancer 2010, 103, 382–390. [Google Scholar] [CrossRef]
- Cherciu, I.; Bărbălan, A.; Pirici, D.; Mărgăritescu, C.; Săftoiu, A. Stem cells, colorectal cancer and cancer stem cell markers correlations. Curr. Health Sci. J. 2014, 40, 153–161. [Google Scholar]
- Hayat, M.A. (Ed.) Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury: Volume 2; Springer: Dordrecht, The Netherlands, 2012. [Google Scholar]
- Sprenger, T.; Conradi, L.-C.; Beißbarth, T.; Ermert, H.; Homayounfar, K.; Middel, P.; Rüschoff, J.; Wolff, H.A.; Schüler, P.; Ghadimi, B.M.; et al. Enrichment of CD133-expressing cells in rectal cancers treated with preoperative radiochemotherapy is an independent marker for metastasis and survival. Cancer 2012, 119, 26–35. [Google Scholar] [CrossRef]
- Abbasian, M.; Mousavi, E.; Arab-Bafrani, Z.; Sahebkar, A. The most reliable surface marker for the identification of colorectal cancer stem-like cells: A systematic review and meta-analysis. J. Cell. Physiol. 2018, 234, 8192–8202. [Google Scholar] [CrossRef] [PubMed]
- Jao, S.-W.; Chen, S.-F.; Lin, Y.-S.; Chang, Y.-C.; Lee, T.-Y.; Wu, C.-C.; Jin, J.-S.; Nieh, S. Cytoplasmic CD133 Expression is a Reliable Prognostic Indicator of Tumor Regression After Neoadjuvant Concurrent Chemoradiotherapy in Patients with Rectal Cancer. Ann. Surg. Oncol. 2012, 19, 3432–3440. [Google Scholar] [CrossRef] [PubMed]
- Ren, F. CD133: A cancer stem cells marker, is used in colorectal cancers. World J. Gastroenterol. 2013, 19, 2603–2611. [Google Scholar] [CrossRef]
- Horst, D.; Kriegl, L.; Engel, J.; Kirchner, T.; Jung, A. Prognostic significance of the cancer stem cell markers CD133, CD44, and CD166 in colorectal cancer. Cancer Investig. 2009, 27, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Jin, X.; Lan, X.; Lang, J.; Wen, Q.; An, R. SPECT imaging of colorectal cancer by targeting CD 133 receptor with 99mTc-labeled monoclonal antibody. Q. J. Nucl. Med. Mol. Imaging 2019, 63, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Jannie, K.M. Activated Leukocyte Cell Adhesion Molecule (ALCAM) Regulation of Tumor Cell Behavior and Neuronal Targeting. Ph.D. Thesis, University of Iowa, Iowa City, IA, USA, 2012. [Google Scholar]
- Wahab, S.R.; Islam, F.; Gopalan, V.; Lam, A.K.-Y. The Identifications and Clinical Implications of Cancer Stem Cells in Colorectal Cancer. Clin. Color. Cancer 2017, 16, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Kalantari, E.; Taheri, T.; Fata, S.; Abolhasani, M.; Mehrazma, M.; Madjd, Z.; Asgari, M. Significant co-expression of putative cancer stem cell markers, EpCAM and CD166, correlates with tumor stage and invasive behavior in colorectal cancer. World J. Surg. Oncol. 2022, 20, 15. [Google Scholar] [CrossRef]
- Márquez-González, R.M.; Saucedo-Sariñana, A.M.; Barros-Núñez, P.; Gallegos-Arreola, M.P.; Pineda-Razo, T.D.; Marin-Contreras, M.E.; Flores-Martínez, S.E.; Sánchez-Corona, J.; Rosales-Reynoso, M.A. CD44 Genotypes Are Associated with Susceptibility and Tumor Characteristics in Colorectal Cancer Patients. Tohoku J. Exp. Med. 2020, 250, 109–119. [Google Scholar] [CrossRef]
- Wang, Z.; Tang, Y.; Xie, L.; Huang, A.; Xue, C.; Gu, Z.; Wang, K.; Zong, S. The Prognostic and Clinical Value of CD44 in Colorectal Cancer: A Meta-Analysis. Front. Oncol. 2019, 9, 309. [Google Scholar] [CrossRef]
- Basakran, N.S. CD44 as a potential diagnostic tumor marker. Saudi Med. J. 2015, 36, 273–279. [Google Scholar] [CrossRef]
- Dalerba, P.; Dylla, S.J.; Park, I.K.; Liu, R.; Wang, X.; Cho, R.W.; Hoey, T.; Gurney, A.; Huang, E.H.; Simeone, D.M.; et al. Phenotypic characterization of human colorectal cancer stem cells. Proc. Natl. Acad. Sci. USA 2012, 104, 10158–10163. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.L.; Oshi, M.; Endo, I.; Takabe, K. Clinical relevance of stem cell surface markers CD133, CD24, and CD44 in colorectal cancer. Am. J. Cancer Res. 2021, 11, 5141–5154. [Google Scholar] [PubMed]
- Huang, T.; Song, X.; Xu, D.; Tiek, D.; Goenka, A.; Wu, B.; Sastry, N.; Hu, B.; Cheng, S.-Y. Stem cell programs in cancer initiation, progression, and therapy resistance. Theranostics 2020, 10, 8721–8743. [Google Scholar] [CrossRef] [PubMed]
- Johari, B.; Rezaeejam, H.; Moradi, M.; Taghipour, Z.; Saltanatpour, Z.; Mortazavi, Y.; Nasehi, L. Increasing the colon cancer cells sensitivity toward radiation therapy via application of Oct4–Sox2 complex decoy oligodeoxynucleotides. Mol. Biol. Rep. 2020, 47, 6793–6805. [Google Scholar] [CrossRef]
- Bigdelou, Z.; Mortazavi, Y.; Saltanatpour, Z.; Asadi, Z.; Kadivar, M.; Johari, B. Role of Oct4–Sox2 complex decoy oligodeoxynucleotides strategy on reverse epithelial to mesenchymal transition (EMT) induction in HT29-ShE encompassing enriched cancer stem-like cells. Mol. Biol. Rep. 2020, 47, 1859–1869. [Google Scholar] [CrossRef]
- Binefa, G.; Rodríguez-Moranta, F.; Teule, À.; Medina-Hayas, M. Colorectal cancer: From prevention to personalized medicine. World J. Gastroenterol. WJG 2014, 20, 6786–6808. [Google Scholar] [CrossRef]
- De Angelis, M.L.; Francescangeli, F.; Zeuner, A.; Baiocchi, M. Colorectal Cancer Stem Cells: An Overview of Evolving Methods and Concepts. Cancers 2021, 13, 5910. [Google Scholar] [CrossRef]
- Yan, X.; Ma, L.; Yi, D.; Yoon, J.-G.; Diercks, A.; Foltz, G.; Price, N.D.; Hood, L.E.; Tian, Q. A CD133-related gene expression signature identifies an aggressive glioblastoma subtype with excessive mutations. Proc. Natl. Acad. Sci. USA 2011, 108, 1591–1596. [Google Scholar] [CrossRef]
- Aramini, B.; Masciale, V.; Grisendi, G.; Bertolini, F.; Maur, M.; Guaitoli, G.; Chrystel, I.; Morandi, U.; Stella, F.; Dominici, M.; et al. Dissecting Tumor Growth: The Role of Cancer Stem Cells in Drug Resistance and Recurrence. Cancers 2022, 14, 976. [Google Scholar] [CrossRef]
- Bisht, S.; Nigam, M.; Kunjwal, S.S.; Sergey, P.; Mishra, A.P.; Sharifi-Rad, J. Cancer Stem Cells: From an Insight into the Basics to Recent Advances and Therapeutic Targeting. Stem Cells Int. 2022, 2022, 9653244. [Google Scholar] [CrossRef] [PubMed]
- Fidelle, M.; Yonekura, S.; Picard, M.; Cogdill, A.; Hollebecque, A.; Roberti, M.P.; Zitvogel, L. Resolving the Paradox of Colon Cancer Through the Integration of Genetics, Immunology, and the Microbiota. Front. Immunol. 2020, 11, 600886. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-L.; Pan, F.; Jiang, H.; Chen, J.-F.; Pei, L.; Xie, F.-W.; Liang, H.-J. Highly enriched CD133+CD44+ stem-like cells with CD133+CD44high metastatic subset in HCT116 colon cancer cells. Clin. Exp. Metastasis 2011, 28, 751–763. [Google Scholar] [CrossRef] [PubMed]
- Jing, F.; Kim, H.J.; Kim, C.H.; Kim, Y.J.; Lee, J.H.; Kim, H.R. Colon cancer stem cell markers CD44 and CD133 in patients with colorectal cancer and synchronous hepatic metastases. Int. J. Oncol. 2015, 46, 1582–1588. [Google Scholar] [CrossRef] [PubMed]
- Giampieri, R.; Scartozzi, M.; Loretelli, C.; Piva, F.; Mandolesi, A.; Lezoche, G.; Del Prete, M.; Bittoni, A.; Faloppi, L.; Bianconi, M.; et al. Cancer Stem Cell Gene Profile as Predictor of Relapse in High Risk Stage II and Stage III, Radically Resected Colon Cancer Patients. PLoS ONE 2013, 8, e72843. [Google Scholar] [CrossRef]
- Artells, R.; Moreno, I.; Díaz, T.; Martínez, F.; Gel, B.; Navarro, A.; Ibeas, R.; Moreno, J.; Monzó, M. Tumour CD133 mRNA expression and clinical outcome in surgically resected colorectal cancer patients. Eur. J. Cancer 2010, 46, 642–649. [Google Scholar] [CrossRef]
- Huang, X.; Sheng, Y.; Guan, M. Co-expression of stem cell genes CD133 and CD44 in colorectal cancers with early liver metastasis. Surg. Oncol. 2012, 21, 103–107. [Google Scholar] [CrossRef]
- Olejniczak, A.; Szaryńska, M.; Kmieć, Z. In vitro characterization of spheres derived from colorectal cancer cell lines. Int. J. Oncol. 2017, 52, 599–612. [Google Scholar] [CrossRef]
- Patel, B.B.; Yu, Y.; Du, J.; Levi, E.; Phillip, P.A.; Majumdar, A.P. Age-related increase in colorectal cancer stem cells in macroscopically normal mucosa of patients with adenomas: A risk factor for colon cancer. Biochem. Biophys. Res. Commun. 2009, 378, 344–347. [Google Scholar] [CrossRef]
- Kim, W.-T.; Ryu, A.C.J. Cancer stem cell surface markers on normal stem cells. BMB Rep. 2017, 50, 285–298. [Google Scholar] [CrossRef]
- Walcher, L.; Kistenmacher, A.-K.; Suo, H.; Kitte, R.; Dluczek, S.; Strauß, A.; Blaudszun, A.-R.; Yevsa, T.; Fricke, S.; Kossatz-Boehlert, U. Cancer Stem Cells—Origins and Biomarkers: Perspectives for Targeted Personalized Therapies. Front. Immunol. 2020, 11, 1280. [Google Scholar] [CrossRef] [PubMed]
- Doak, S.H.; Zaïr, Z.M. Real-Time Reverse-Transcription Polymerase Chain Reaction: Technical Considerations for Gene Expression Analysis. Genet. Toxicol. 2011, 817, 251–270. [Google Scholar] [CrossRef]
- Mărgaritescu, C.; Pirici, D.; Cherciu, I.; Bărbălan, A.; Cârtână, T.; Săftoiu, A. CD133/CD166/Ki-67 triple immunofluorescence assessment for putative cancer stem cells in colon carcinoma. J. Gastrointest. Liver Dis. 2014, 23, 161–170. [Google Scholar] [CrossRef]
- Bărbălan, A.; Nicolaescu, A.C.; Măgăran, A.V.; Mercuţ, R.; Bălăşoiu, M.; Băncescu, G.; Şerbănescu, M.S.; Lazăr, O.F.; Săftoiu, A. Immunohistochemistry predictive markers for primary colorectal cancer tumors: Where are we and where are we going? Rom. J. Morphol. Embryol. 2018, 59, 29–42. [Google Scholar] [PubMed]
- Quasar Collaborative Group. Adjuvant chemotherapy versus observation in patients with colorectal cancer: A randomised study. Lancet 2007, 370, 2020–2029. [Google Scholar] [CrossRef]
- Hansen, A.G.; Freeman, T.J.; Arnold, S.A.; Starchenko, A.; Jones-Paris, C.R.; Gilger, M.A.; Washington, M.K.; Fan, K.-H.; Shyr, Y.; Beauchamp, R.D.; et al. Elevated ALCAM Shedding in Colorectal Cancer Correlates with Poor Patient Outcome. Cancer Res. 2013, 73, 2955–2964. [Google Scholar] [CrossRef]
- Berger, A.W.; Raedler, K.; Langner, C.; Ludwig, L.; Dikopoulos, N.; Becker, K.F.; Slotta-Huspenina, J.; Quante, M.; Schwerdel, D.; Perkhofer, L.; et al. Genetic Biopsy for Prediction of Surveillance Intervals after Endoscopic Resection of Colonic Polyps: Results of the GENESIS Study. United Eur. Gastroenterol. J. 2017, 6, 290–299. [Google Scholar] [CrossRef]
- Zalewski, A.; Snook, A.E.; Waldman, S.A. Stem cells as therapeutic targets in colorectal cancer. Pers. Med. 2021, 18, 171–183. [Google Scholar] [CrossRef]
- Shibata, M.; Hoque, M.O. Targeting Cancer Stem Cells: A Strategy for Effective Eradication of Cancer. Cancers 2019, 11, 732. [Google Scholar] [CrossRef]
- Desai, A.; Yan, Y.; Gerson, S.L. Concise Reviews: Cancer Stem Cell Targeted Therapies: Toward Clinical Success. Stem Cells Transl. Med. 2018, 8, 75–81. [Google Scholar] [CrossRef]
- Hasbullah, H.H.; Musa, M. Gene Therapy Targeting p53 and KRAS for Colorectal Cancer Treatment: A Myth or the Way Forward? Int. J. Mol. Sci. 2021, 22, 11941. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.R.; Santos, L.D.S.; Dias, R.B.; Quadros, C.A.; Bezerra, D.P. Emerging agents that target signaling pathways to eradicate colorectal cancer stem cells. Cancer Commun. 2021, 41, 1275–1313. [Google Scholar] [CrossRef] [PubMed]
- Patsalias, A.; Kozovska, Z. Personalized medicine: Stem cells in colorectal cancer treatment. Biomed. Pharmacother. 2021, 141, 111821. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Volume (µL) |
|---|---|
| 10X RT Buffer | 2 |
| 25X dNTP Mix (100 mM) | 0.8 |
| 10X RT Random Primers | 2 |
| MultiscribeTM Reverse Transcriptase | 1 |
| RNAase Inhibitors | 1 |
| Nuclease-Free dH2O | 3.2 |
| Total per Reaction | 10.0 |
| Step 1 | Step 2 | Step 3 | Step 4 | |
|---|---|---|---|---|
| Temperature (°C) | 25 | 37 | 85 | 4 |
| Time | 10 min | 120 min | 5 sec | ∞ |
| Step | UDG Incubation | AmpliTaq Gold, UP Enzyme Activation | PCR | |
|---|---|---|---|---|
| HOLD | HOLD | CYCLE (50 Cycles) | ||
| Denature | Anneal/Extend | |||
| Time | 2 min | 10 min | 15 sec | 1 min |
| Temperature (°C) | 50 | 95 | 95 | 60 |
| Gene | Transcript | Exon boundary | Amplicon size | Code |
|---|---|---|---|---|
| GAPDH | NM_002046.3 | 3-3 | 122 | Hs99999905_m1 |
| CD44 | NM_001202556.1 | 7-8 | 70 | Hs01075861_m1 |
| CD166 | NM_001243280.1 | 2-3 | 103 | Hs00977641_m1 |
| CD133 | NM_001145850.1 | 6-7 | 66 | Hs01009259_m1 |
| Mean age ± SD (range) (yrs) | 63.72 ± 11.16 (25–80) |
| Gender (M/F) | 50/10 |
| Home location (Urban/Rural) | 43/17 |
| Tumor location Descending colon Sigmoid Recto-sigmoid junction Rectum | 2 6 3 49 |
| Histology Adenocarcinoma G1 G2 G3 Undetermined | 12 33 2 13 |
| T stage * T1 T2 T3 T4 | 2 6 43 9 |
| N stage * N0 N1 N2 | 24 24 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harbiyeli, I.F.C.; Burtea, D.E.; Ivan, E.T.; Streață, I.; Nicoli, E.R.; Uscatu, D.; Șerbănescu, M.-S.; Ioana, M.; Vilmann, P.; Săftoiu, A. Assessing Putative Markers of Colorectal Cancer Stem Cells: From Colonoscopy to Gene Expression Profiling. Diagnostics 2022, 12, 2280. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102280
Harbiyeli IFC, Burtea DE, Ivan ET, Streață I, Nicoli ER, Uscatu D, Șerbănescu M-S, Ioana M, Vilmann P, Săftoiu A. Assessing Putative Markers of Colorectal Cancer Stem Cells: From Colonoscopy to Gene Expression Profiling. Diagnostics. 2022; 12(10):2280. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102280
Chicago/Turabian StyleHarbiyeli, Irina Florina Cherciu, Daniela Elena Burtea, Elena Tatiana Ivan, Ioana Streață, Elena Raluca Nicoli, Daniel Uscatu, Mircea-Sebastian Șerbănescu, Mihai Ioana, Peter Vilmann, and Adrian Săftoiu. 2022. "Assessing Putative Markers of Colorectal Cancer Stem Cells: From Colonoscopy to Gene Expression Profiling" Diagnostics 12, no. 10: 2280. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102280