
Deep Learning Assisted Automated Assessment of Thalassaemia from Haemoglobin Electrophoresis Images

 , ,
, ,  and
and
Abstract
:1. Introduction
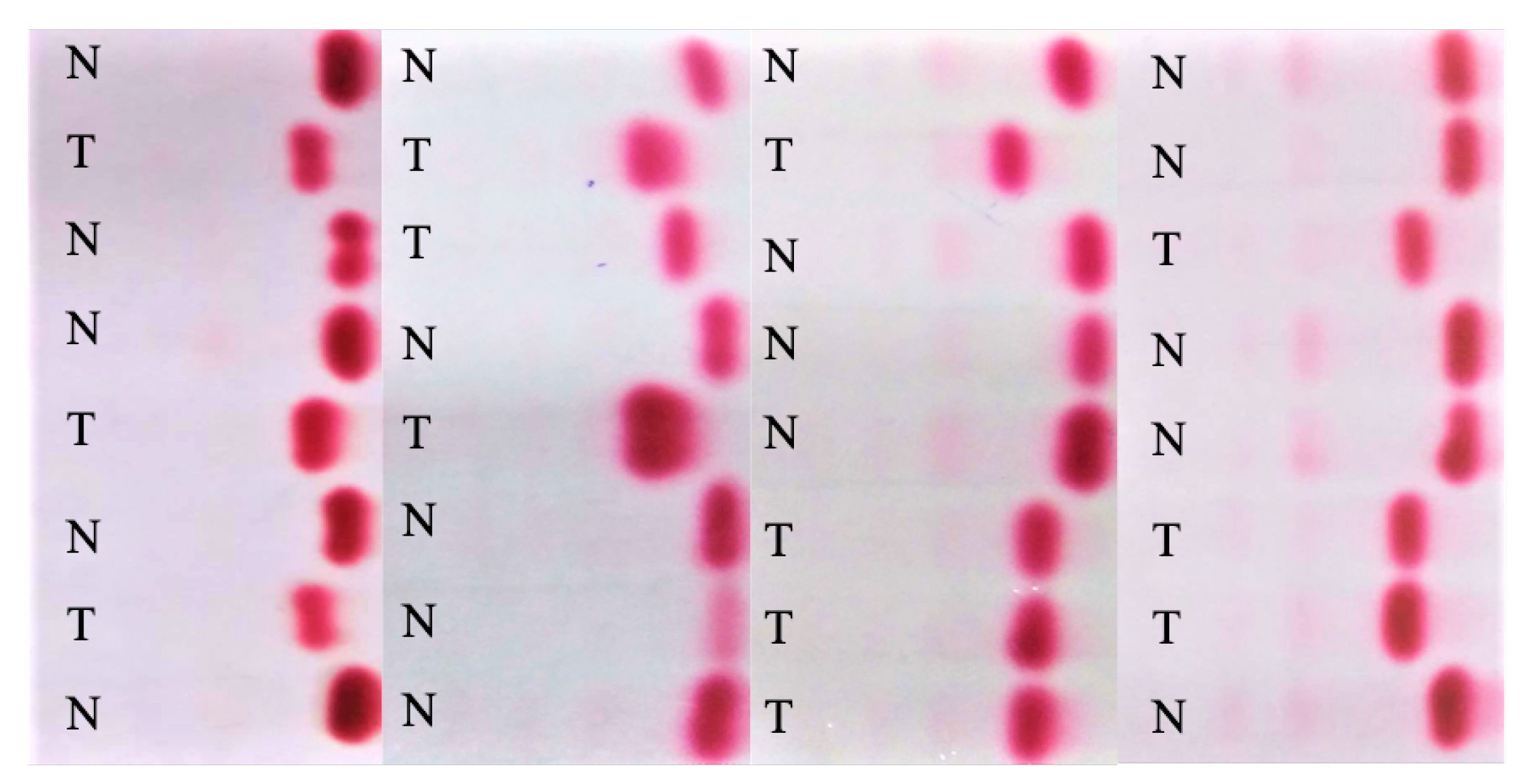
- A relatively large electrophoresis image dataset was created from 824 patients (normal and thalassaemia);
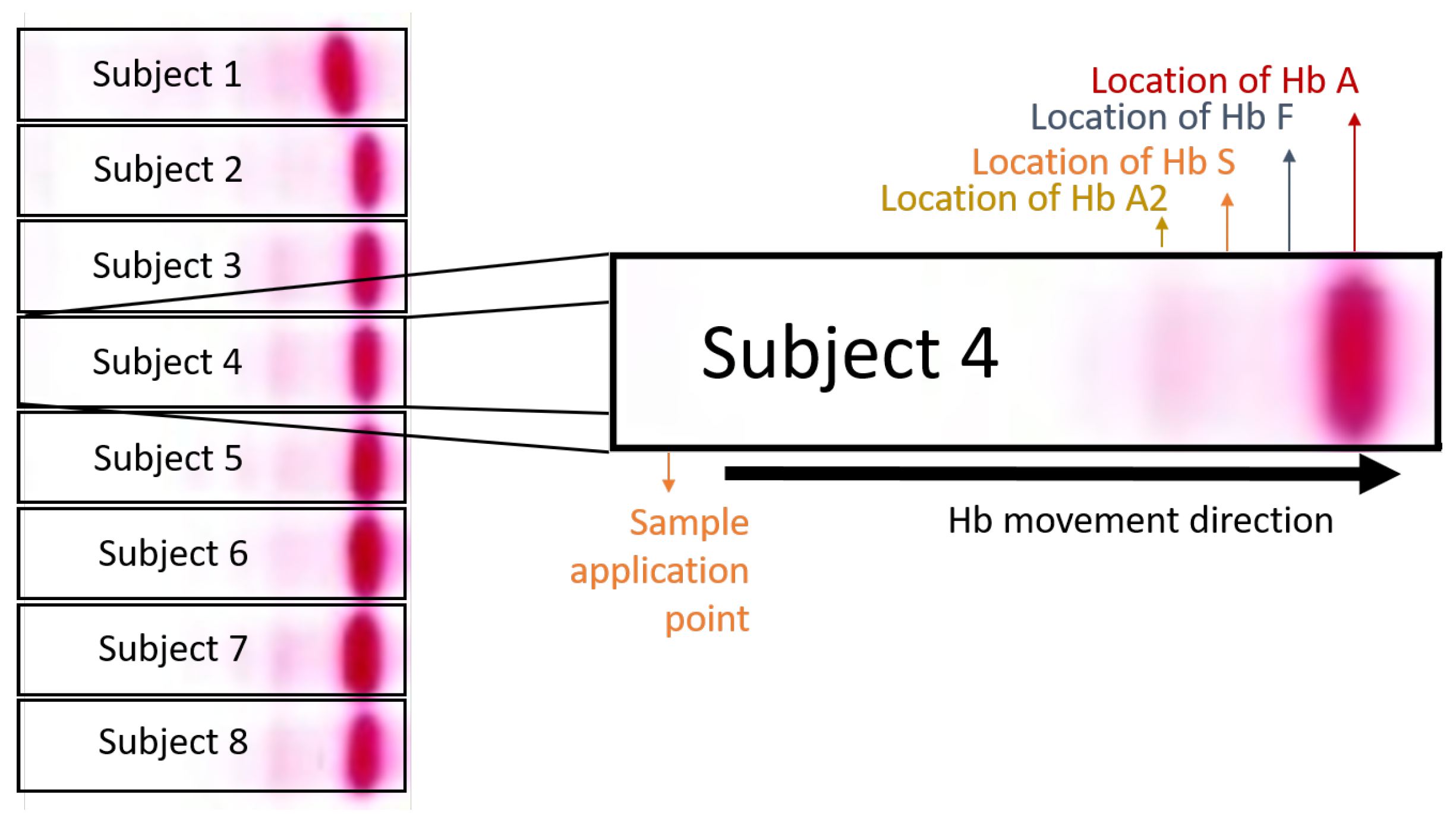
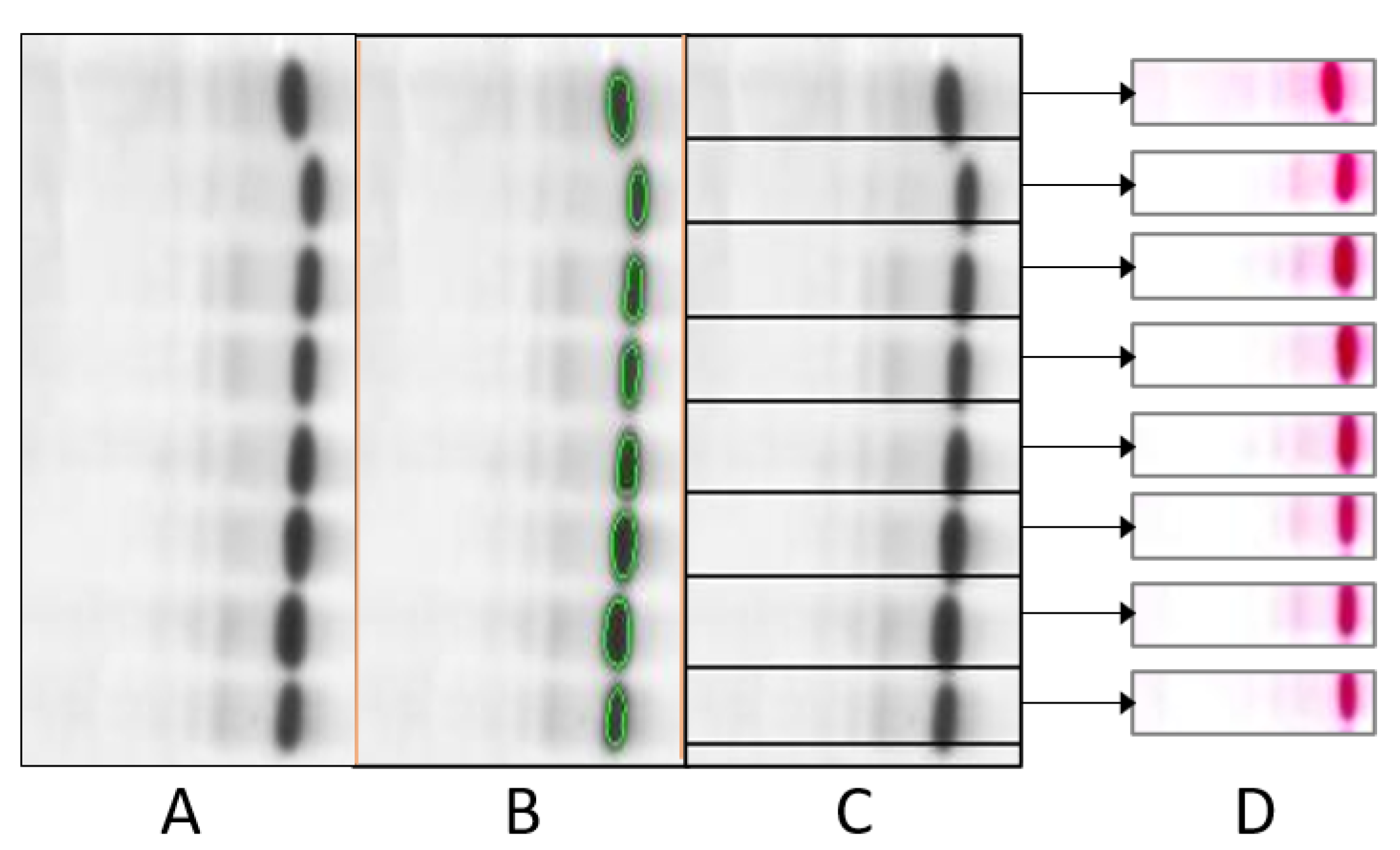
- An automatic lane extraction technique has been proposed, which efficiently detects and extracts lanes from the given cellulose sheet and extract a single patient’s electrophoresis image;
- Seven different pre-trained CNN models were investigated for the classification of electrophoresis images; and
- Image visualization techniques have proposed to investigate where the CNN model is learning from.
2. Deep Convolutional Neural Networks
3. Visualization Techniques
4. Methodology
4.1. Database Development
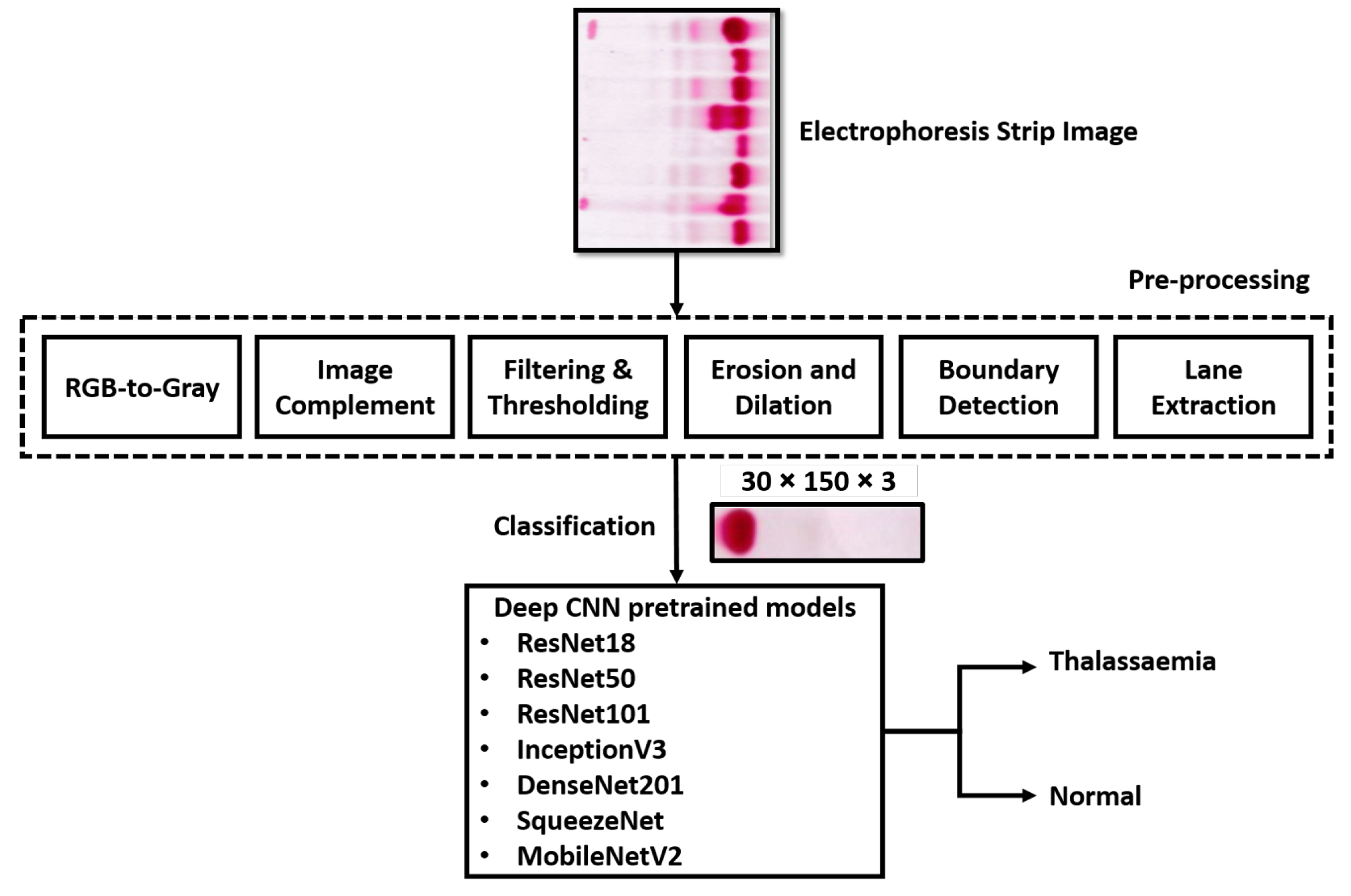
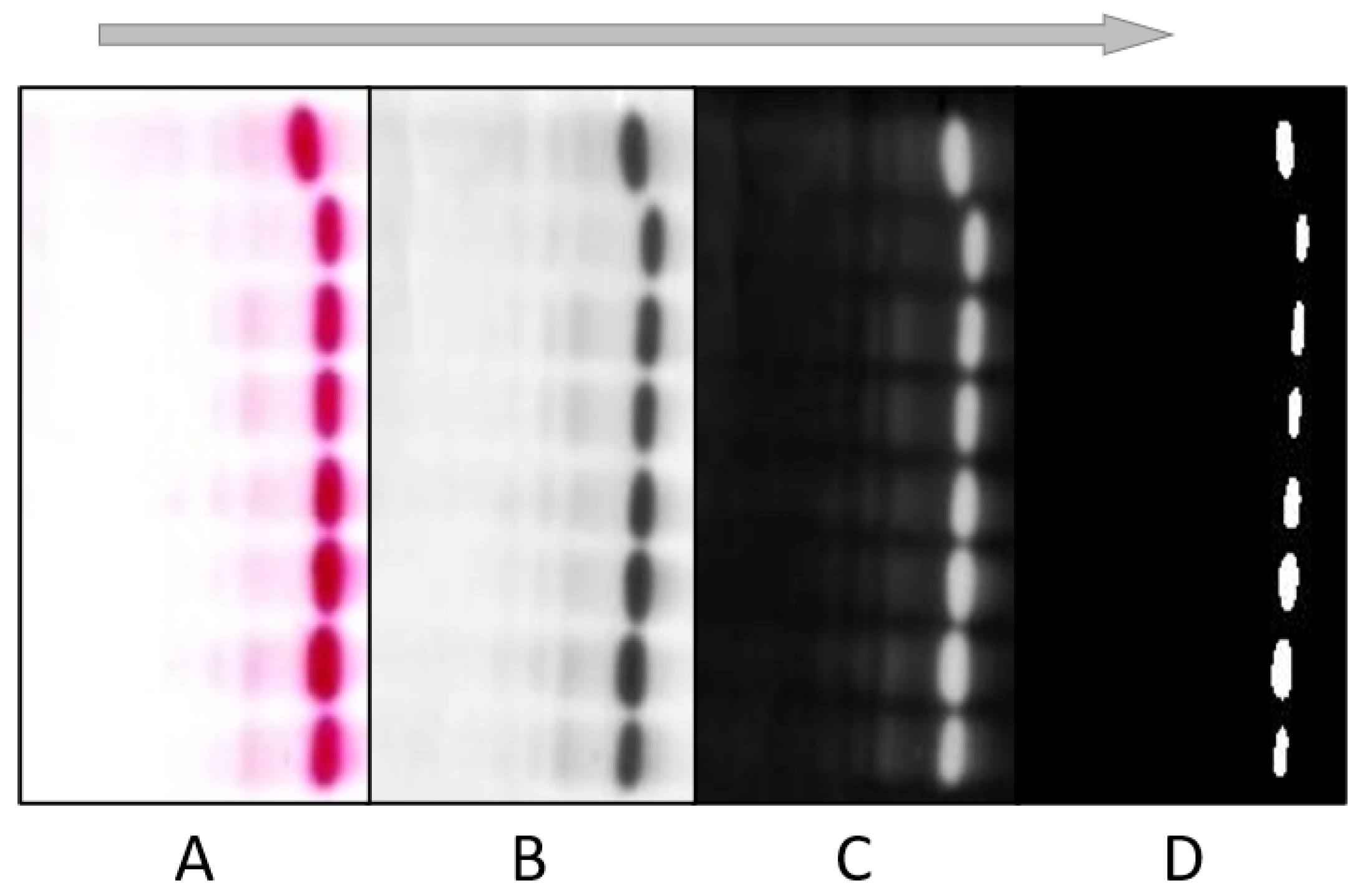
4.2. Pre-Processing
4.2.1. Filtering and Thresholding
4.2.2. Object Detection
4.2.3. Erosion and Dilation
4.2.4. Boundary Detection
4.2.5. Lane Extraction
4.3. Thalassaemia Detection
4.4. Performance Matrix
5. Results and Discussion
- The presence and concentration of HbA2 and HBF determines the severity of the disease. This classifier only classifies beta thalassaemia minor, which involves a specific concentration of Hb. In Southeast Asia, this affects about 15% of cases. These individuals normally do not have any clinically significant issues as long as they maintain Hb levels between 9 and 12 g/dL. There is no need for therapy. Moreover, since this is the first computer-aided diagnosis technique for electrophoresis images, this study is limited to binary classification.
- The populations may not be the same between different studies (e.g., different countries with different levels of healthcare). High confidence intervals were obtained, and the results for the proposed approach were the best among nine other methods, and thus there was probably a slight over-evaluation. The ground truth used was an expert evaluation, and this may not have been the case for the other methods. The fact that the processing of Hb electrophoresis images with deep learning was the best among other techniques has to be confirmed through a blind study designed for this purpose, in which the techniques are applied to the same patients.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tanveer, T.; Masud, H.; Butt, Z.A. Are people getting quality thalassemia care in twin cities of Pakistan? A comparison with international standards. Int. J. Qual. Health Care 2018, 30, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Galanello, R.; Origa, R. Beta-thalassemia. Orphanet J. Rare Dis. 2010, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, A.; Galanello, R. Beta-thalassemia. Genet. Med. 2010, 12, 61–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taher, A.T.; Weatherall, D.J.; Cappellini, M.D. Thalassaemia. Lancet 2018, 391, 155–167. [Google Scholar] [CrossRef]
- Weatherall, D.; Clegg, J.B. Inherited haemoglobin disorders: An increasing global health problem. Bull. World Health Organ. 2001, 79, 704–712. [Google Scholar]
- Angastiniotis, M.; Modell, B. Global epidemiology of hemoglobin disorders. Ann. N. Y. Acad. Sci. 1998, 850, 251–269. [Google Scholar] [CrossRef]
- Ahmed, S.; Saleem, M.; Modell, B.; Petrou, M. Screening extended families for genetic hemoglobin disorders in Pakistan. N. Engl. J. Med. 2002, 347, 1162–1168. [Google Scholar] [CrossRef] [Green Version]
- Bozkurt, G. Results from the north cyprus thalassemia prevention program. Hemoglobin 2007, 31, 257–264. [Google Scholar] [CrossRef]
- Shaikh, A.; Khurshid, M. Prevalence of thalassemia minor trait in Pakistani population presented at Akuh for complete blood count estimation (CBC). J. Pak. Med Assoc. 1993, 43, 98. [Google Scholar]
- Elshami, E.H.; Alhalees, A.M. Automated diagnosis of thalassemia based on datamining classifiers. In Proceedings of the International Conference on Informatics and Applications (ICIA2012), Kuala Terengganu, Malaysia, 3–5 June 2012; pp. 440–445. [Google Scholar]
- Purwar, S.; Tripathi, R.K.; Ranjan, R.; Saxena, R. Detection of microcytic hypochromia using cbc and blood film features extracted from convolution neural network by different classifiers. Multimed. Tools Appl. 2020, 79, 4573–4595. [Google Scholar] [CrossRef]
- Kan, Y.W.; Nathan, D.G. Mild thalassemia: The result of interactions of alpha and beta thalassemia genes. J. Clin. Investig. 1970, 49, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Galanello, R.; Barella, S.; Gasperini, D.; Perseu, L.; Paglietti, E.; Sollaino, C.; Paderi, L.; Pirroni, M.; Maccioni, L.; Mosca, A. Evaluation of an automatic HPLC analyser for thalassemia and haemoglobin variants screening. J. Autom. Chem. 1995, 17, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Kazazian, H.H. Use of PCR in the diagnosis of monogenic disease. In PCR Technology; Springer: Berlin/Heidelberg, Germany, 1989; pp. 153–169. [Google Scholar]
- Bajla, I.; Holländer, I.; Burg, K. Improvement of electrophoretic Gel image analysis. Meas. Sci. Rev. 2001, 1, 5–10. [Google Scholar]
- Skutkova, H.; Vitek, M.; Krizkova, S.; Kizek, R.; Provaznik, I. Preprocessing and classification of electrophoresis gel images using dynamic time warping. Int. J. Electrochem. Sci. 2013, 8, 1609–1622. [Google Scholar]
- Abeykoon, A.; Dhanapala, M.; Yapa, R.; Sooriyapathirana, S. An automated system for analyzing agarose and polyacrylamide gel images. Ceylon. J. Sci. (Biol. Sci.) 2015, 44, 45–54. [Google Scholar] [CrossRef]
- Khodabakhshi, S.; Hassanpour, H. Automatic lane extraction in hemoglobin and serum protein electrophoresis using image processing. J. Adv. Comput. Res. 2012, 3, 25–31. [Google Scholar]
- Park, S.C.; Na, I.S.; Han, T.H.; Kim, S.H.; Lee, G.S. Lane detection and tracking in PCR gel electrophoresis images. Comput. Electron. Agric. 2012, 83, 85–91. [Google Scholar] [CrossRef]
- Akay, A.; Dragomir, A.; Yardimci, A.; Canatan, D.; Yesilipek, A.; Pogue, B.W. A data-mining approach for investigating social and economic geographical dynamics of β-thalassemia’s spread. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Christodoulidis, S.; Anthimopoulos, M.; Ebner, L.; Christe, A.; Mougiakakou, S. Multisource transfer learning with convolutional neural networks for lung pattern analysis. IEEE J. Biomed. Health Inform. 2016, 21, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akçay, S.; Kundegorski, M.E.; Devereux, M.; Breckon, T.P. Transfer learning using convolutional neural networks for object classification within x-ray baggage security imagery. In Proceedings of the 2016 IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, 25–28 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1057–1061. [Google Scholar]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional neural networks for medical image analysis: Full training or fine tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2009, 22, 1345–1359. [Google Scholar] [CrossRef]
- Rahman, T.; Chowdhury, M.E.; Khandakar, A.; Islam, K.R.; Islam, K.F.; Mahbub, Z.B.; Kadir, M.A.; Kashem, S. Transfer Learning with Deep Convolutional Neural Network (CNN) for Pneumonia Detection using Chest X-ray. Appl. Sci. 2020, 10, 3233. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- LeCun, Y.; Kavukcuoglu, K.; Farabet, C. Convolutional networks and applications in vision. In Proceedings of the 2010 IEEE International Symposium on Circuits and Systems, Paris, France, 30 May–2 June 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 253–256. [Google Scholar]
- Smilkov, D.; Thorat, N.; Kim, B.; Viégas, F.; Wattenberg, M. Smoothgrad: Removing noise by adding noise. arXiv 2017, arXiv:1706.03825. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Chattopadhay, A.; Sarkar, A.; Howlader, P.; Balasubramanian, V.N. Grad-cam++: Generalized gradient-based visual explanations for deep convolutional networks. In Proceedings of the 2018 IEEE Winter Conference on Applications of Computer Vision (WACV), Lake Tahoe, NV, USA, 12–15 March 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 839–847. [Google Scholar]
- Wang, H.; Wang, Z.; Du, M.; Yang, F.; Zhang, Z.; Ding, S.; Mardziel, P.; Hu, X. Score-CAM: Score-weighted visual explanations for convolutional neural networks. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Seattle, WA, USA, 14–19 June 2020; pp. 24–25. [Google Scholar]
- Gedraite, E.S.; Hadad, M. Investigation on the effect of a Gaussian Blur in image filtering and segmentation. In Proceedings of the ELMAR-2011, Zadar, Croatia, 14–16 September 2011; pp. 393–396. [Google Scholar]
- Yildiz, Z. A New Approach for Counting and Sizing the Objects: Image Weight Signal. Doctoral Dissertation, Ankara Yildirim Beyazit Universitesi Fen Bilimleri Enstitusu, Ankara, Turkey, 2016. [Google Scholar]
- Jawas, N.; Suciati, N. Image inpainting using erosion and dilation Operation. Int. J. Adv. Sci. Technol. 2013, 51, 127–134. [Google Scholar]
- Pera, M. Explorando redes Neuronales Convolucionales para Reconocimiento de Objetos en Imágenes RGB. 2020. Available online: https://repositorio.unican.es/xmlui/handle/10902/19259 (accessed on 22 July 2022).
- Kabootarizadeh, L.; Jamshidnezhad, A.; Koohmareh, Z. Differential diagnosis of iron-deficiency anemia from β-thalassemia trait using an intelligent model in comparison with discriminant indexes. Acta Inform. Med. 2019, 27, 78. [Google Scholar] [CrossRef]
- Das, R.; Datta, S.; Kaviraj, A.; Sanyal, S.N.; Nielsen, P.; Nielsen, I.; Sharma, P.; Sanyal, T.; Dey, K.; Saha, S. A decision support scheme for beta thalassemia and HbE carrier screening. J. Adv. Res. 2020, 24, 183–190. [Google Scholar] [CrossRef]
- Wongseree, W.; Chaiyaratana, N.; Vichittumaros, K.; Winichagoon, P.; Fucharoen, S. Thalassaemia classification by neural networks and genetic programming. Inf. Sci. 2007, 177, 771–786. [Google Scholar] [CrossRef]
- Setsirichok, D.; Piroonratana, T.; Wongseree, W.; Usavanarong, T.; Paulkhaolarn, N.; Kanjanakorn, C.; Sirikong, M.; Limwongse, C.; Chaiyaratana, N. Classification of complete blood count and haemoglobin typing data by a C4. 5 decision tree, a naïve Bayes classifier and a multilayer perceptron for thalassaemia screening. Biomed. Signal Process. Control 2012, 7, 202–212. [Google Scholar] [CrossRef]
- Paokanta, P.; Ceccarelli, M.; Srichairatanakool, S. The effeciency of data types for classification performance of Machine Learning Techniques for screening β-Thalassemia. In Proceedings of the 2010 3rd International Symposium on Applied Sciences in Biomedical and Communication Technologies (ISABEL 2010), Roma, Italy, 7–10 November 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 1–4. [Google Scholar]
- Amendolia, S.R.; Brunetti, A.; Carta, P.; Cossu, G.; Ganadu, M.; Golosio, B.; Mura, G.M.; Pirastru, M.G. A real-time classification system of thalassemic pathologies based on artificial neural networks. Med. Decis. Mak. 2002, 22, 18–26. [Google Scholar] [CrossRef]
- HosseiniEshpala, R.; Langarizadeh, M.; KamkarHaghighi, M.; Banafsheh, T. Designing an expert system for differential diagnosis of β-Thalassemia minor and Iron-Deficiency anemia using neural network. Hormozgan Med. J. 2016, 20, 1–9. [Google Scholar]
- Marzuki, N.I.B.C.; Bin Mahmood, N.H.; Bin Abdul Razak, M.A. Identification of thalassemia disorder using active contour. Indones. J. Electr. Eng. Comput. Sci. 2017, 6, 160–165. [Google Scholar] [CrossRef]
- Borah, M.S.; Bhuyan, B.P.; Pathak, M.S.; Bhattacharya, P. Machine learning in predicting hemoglobin variants. Int. J. Mach. Learn. Comput. 2018, 8, 140–143. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types | Total No. of Hb Electrophoresis Images/Class | Training without and with Image Augmentation | ||
|---|---|---|---|---|
| Training Set/ Fold | Validation Set/Fold | Test Set/ Fold | ||
| Normal | 262 | 189 * 15 = 2835 | 21 | 52 |
| Thalassaemia | 262 | 189 * 15 = 2835 | 21 | 52 |
| Training Parameters | |
|---|---|
| batch size | 16 |
| learning rate | 0.001 |
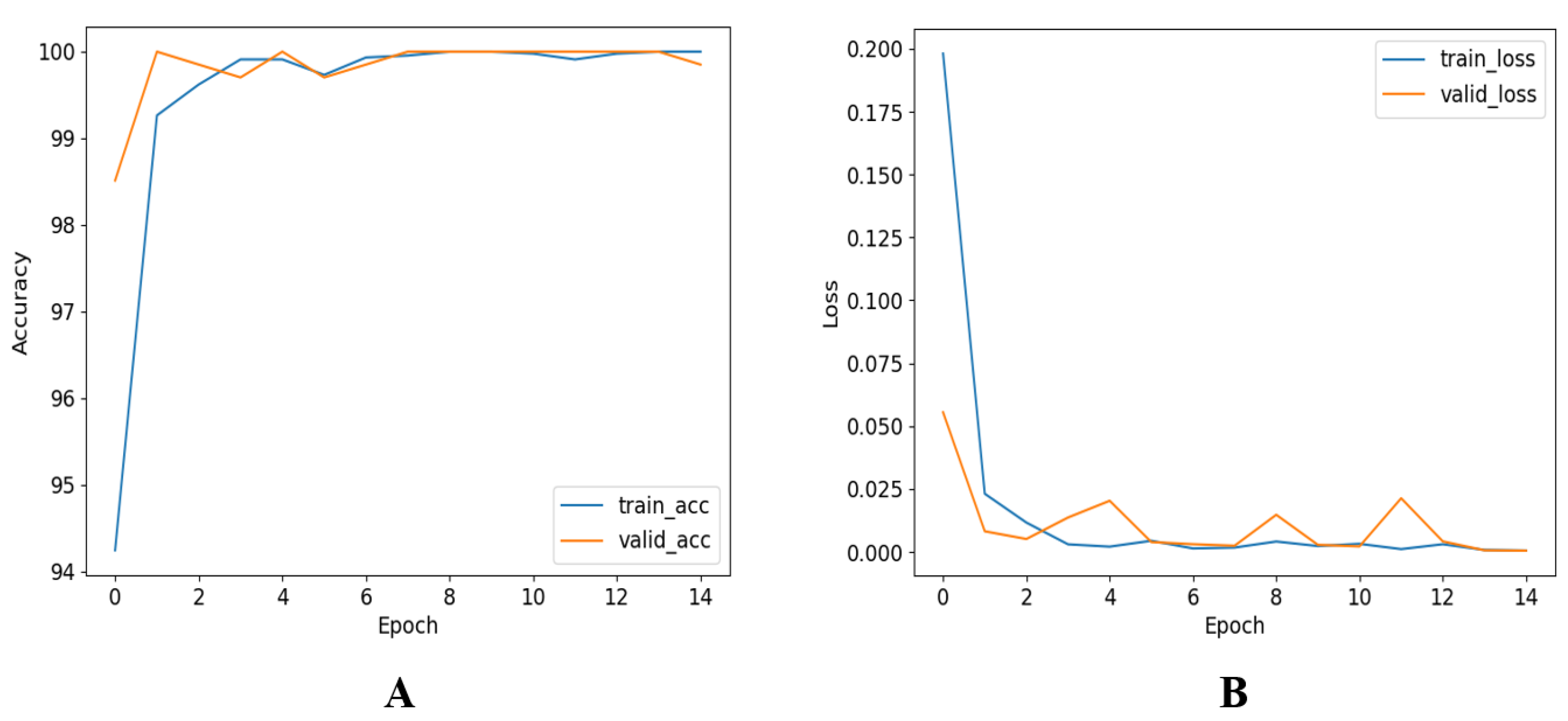
| epochs | 15 |
| epoch patience | 4 |
| stopping criteria | 5 |
| optimizer | Adam |
| Network | Accuracy (%) | Precision (%) | Recall (%) | F1-Score (%) | Specificity (%) | Elapsed Time for Testing (perImage) (te) (Seconds) | Area under the Curve (AUC) |
|---|---|---|---|---|---|---|---|
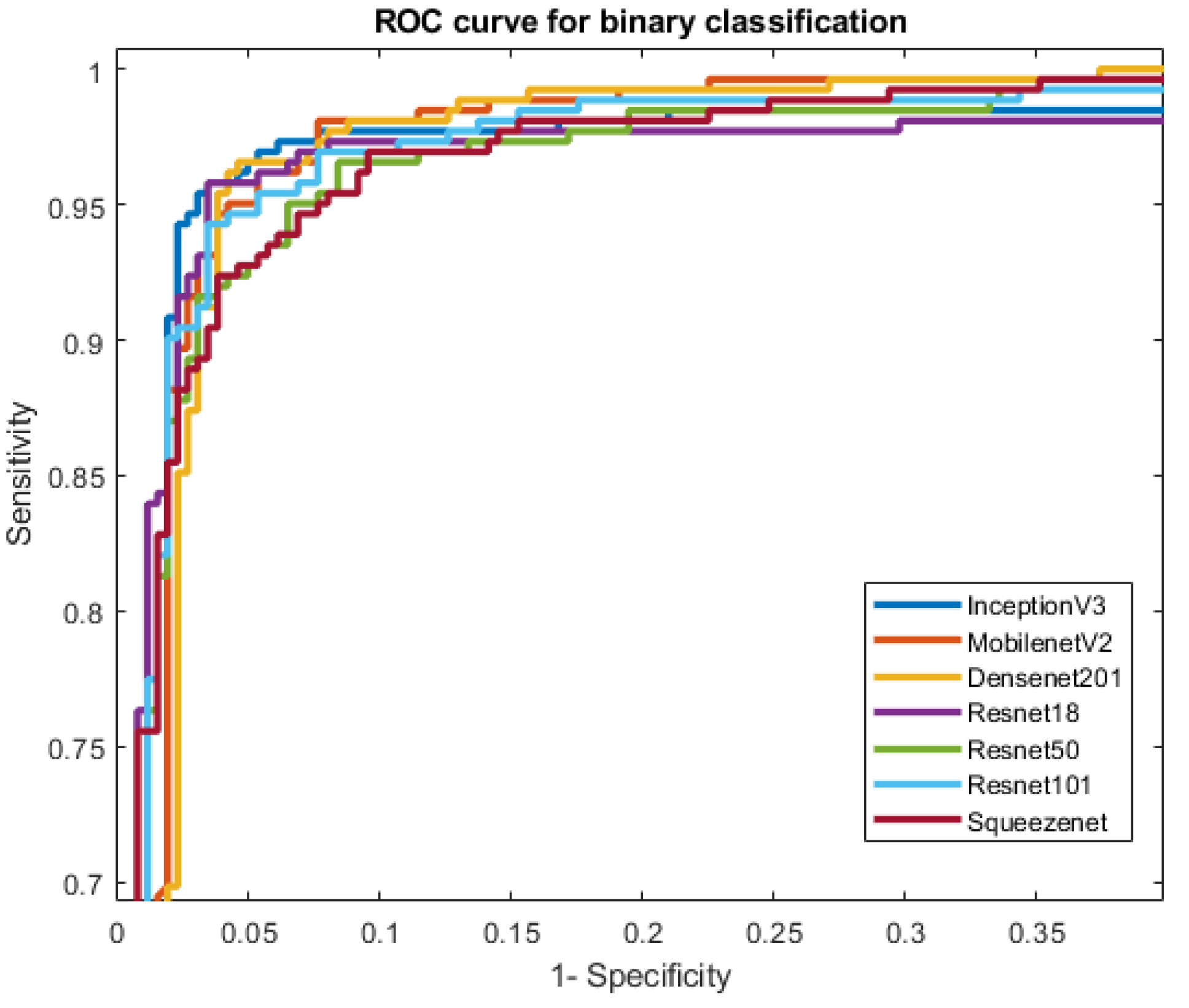
| InceptionV3 | 95.80 ± 1.72 | 95.84 ± 2.42 | 95.80 ± 2.43 | 95.80 ± 2.43 | 95.80 ± 2.43 | 0.97 | 96.88 |
| MobileNetV2 | 95.61 ± 1.75 | 95.66 ± 2.47 | 95.60 ± 2.48 | 95.63 ± 2.48 | 95.60 ± 2.48 | 0.24 | 95.60 |
| Densnet201 | 95.42 ± 1.79 | 95.44 ± 2.53 | 95.42 ± 2.53 | 95.42 ± 2.53 | 95.42 ± 2.53 | 0.68 | 96.75 |
| ResNet18 | 95.23 ± 1.82 | 95.26 ± 2.57 | 95.22 ± 2.58 | 95.22 ± 2.58 | 95.22 ± 2.58 | 0.31 | 96.65 |
| ResNet50 | 94.08 ± 2.02 | 94.12 ± 2.85 | 94.08 ± 2.86 | 94.08 ± 2.86 | 94.08 ± 2.86 | 0.44 | 95.22 |
| ResNet101 | 94.85 ± 1.89 | 94.96 ± 2.65 | 94.85 ± 2.68 | 94.84 ± 2.68 | 94.85 ± 2.68 | 0.60 | 93.85 |
| SqueezeNet | 93.89 ± 2.05 | 93.90 ± 2.90 | 93.89 ± 2.90 | 93.89 ± 2.90 | 93.89 ± 2.90 | 0.28 | 93.02 |
| Network | Parameters (Millions) |
|---|---|
| InceptionV3 | 23.9 |
| MobileNetV2 | 3.5 |
| Densnet201 | 20 |
| ResNet18 | 11.7 |
| ResNet50 | 25.6 |
| ResNet101 | 44.6 |
| SqueezeNet | 1.24 |
| Reference | Pre-Processing/Features | Classifier/Technique | Accuracy |
|---|---|---|---|
| Waranyu et al. [40] (2007) | red blood cell, a reticulocyte and platelet | ANN and genetic programming | 87.22% |
| Damrongrit et al. [41] (2007) | HPLC | C4.5 decision tree, a naive Bayes classifier and MLP | 93.23% |
| Fatemeh Yousefian et al. [42] (2010) | HbA2 | MLP | 87.40% |
| Paokanta et al. [43] (2011) | HbA2 and Genotype | MLP, KNN and naive Bayes | 86.61% |
| Elshami et al. [10] (2012) | CBC | decision tree, naive Bayes and ANN | 93.70% |
| Hosseini et al. [44] (2016) | CBC | MLP | 92% |
| Marzuki et al. [45] (2017) | CBC and haemoglobin | active contour | 90% |
| Borah et al. [46] (2018) | MCV | KNN and SVM | 95.71% |
| Leila et al. [38] (2019) | CBC, MCH | ANN | 92.50% |
| Reena et al. [39] (2020) | haematological parameters | decision tree, naive Bayes and ANN | 91.74% |
| Proposed approach | Hb electrophoresis test | CNN (InceptionV3) | 95.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salman Khan, M.; Ullah, A.; Khan, K.N.; Riaz, H.; Yousafzai, Y.M.; Rahman, T.; Chowdhury, M.E.H.; Abul Kashem, S.B. Deep Learning Assisted Automated Assessment of Thalassaemia from Haemoglobin Electrophoresis Images. Diagnostics 2022, 12, 2405. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102405
Salman Khan M, Ullah A, Khan KN, Riaz H, Yousafzai YM, Rahman T, Chowdhury MEH, Abul Kashem SB. Deep Learning Assisted Automated Assessment of Thalassaemia from Haemoglobin Electrophoresis Images. Diagnostics. 2022; 12(10):2405. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102405
Chicago/Turabian StyleSalman Khan, Muhammad, Azmat Ullah, Kaleem Nawaz Khan, Huma Riaz, Yasar Mehmood Yousafzai, Tawsifur Rahman, Muhammad E. H. Chowdhury, and Saad Bin Abul Kashem. 2022. "Deep Learning Assisted Automated Assessment of Thalassaemia from Haemoglobin Electrophoresis Images" Diagnostics 12, no. 10: 2405. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12102405