
Accuracy of Noninvasive Diagnostic Tests for the Detection of Significant and Advanced Fibrosis Stages in Nonalcoholic Fatty Liver Disease: A Systematic Literature Review of the US Studies
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
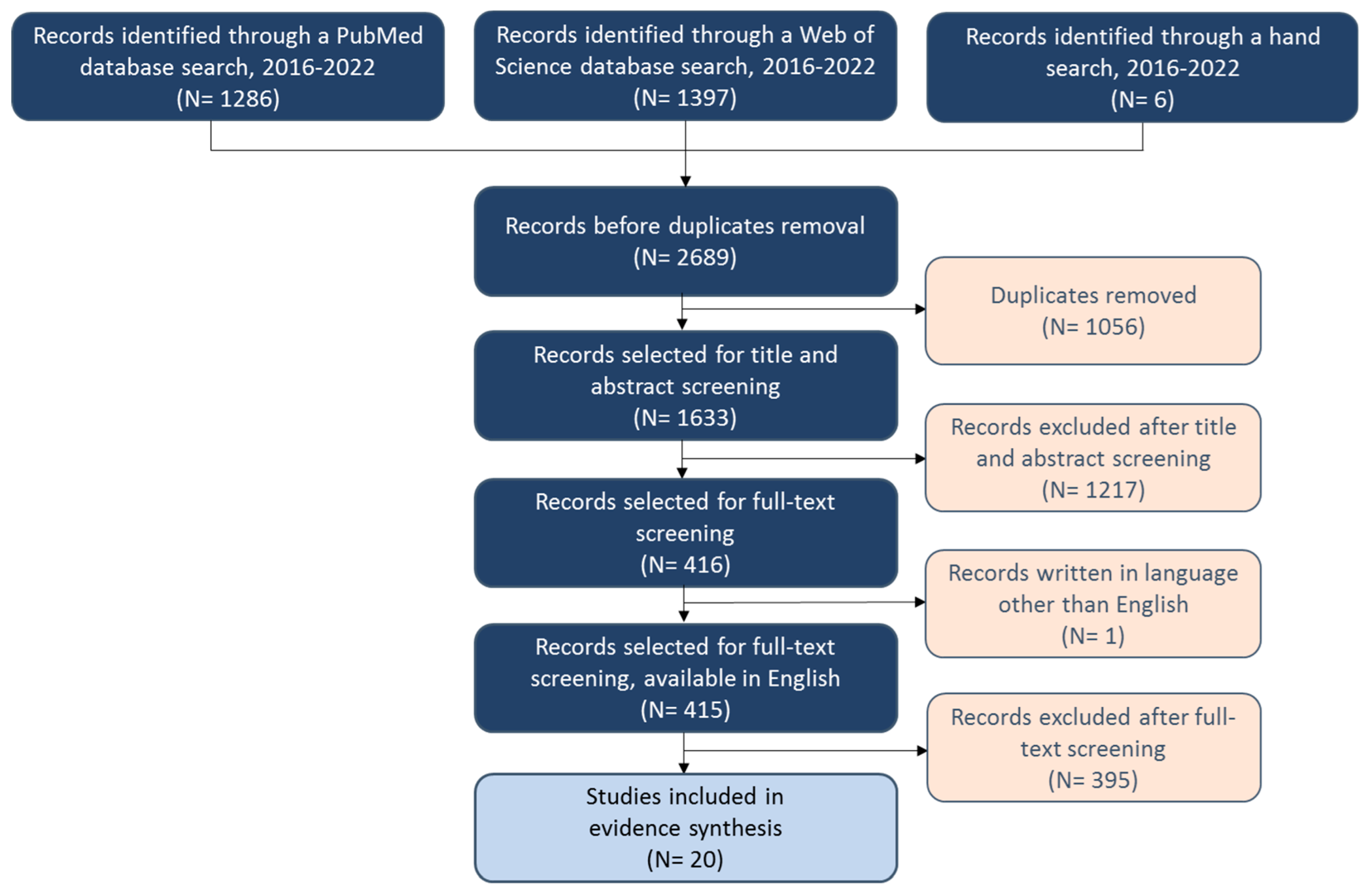
2.1. Data Sources and Selection Criteria
2.2. Search Strategy
2.3. Data Review and Extraction
3. Results
3.1. Imaging Techniques
3.1.1. Vibration-Controlled Transient Elastography (VCTE)
3.1.2. Shear Wave Elastography (SWE)
3.1.3. Magnetic Resonance Elastography (MRE)
3.1.4. Magnetic Resonance Imaging-Derived Liver Surface Nodularity (MRI-Derived LSN) Score
3.2. Established Fibrosis Scores and Biomarkers
3.2.1. NAFLD Fibrosis Score (NFS)
3.2.2. Fibrosis-4 (FIB-4) Index
3.2.3. AST to Platelet Ratio Index (APRI)
3.2.4. BARD Score
3.2.5. Enhanced Liver Fibrosis (ELF) Test
3.2.6. FibroTest
3.2.7. Gamma-Glutamyl Transferase (GGT) Levels
3.2.8. Aspartate Aminotransferase/Alanine Aminotransferase Ratio (AST/ALT Ratio)
3.2.9. AST and ALT Levels
3.3. Novel Biomarkers
3.3.1. Cytokeratine-18 (CK-18) Fragments M30 and M65
3.3.2. Procollagen Type-III N-Terminal Peptide (PRO-C3)
3.3.3. Monocyte Chemoattractant Protein 1 (MCP-1)
3.3.4. NAFLD Fibrosis Protein Panel (NFPP) and a Disintegrin and Metalloproteinase with Thrombospondin Motifs like 2 (ADAMTSL2)
3.3.5. Kulkarni Model
3.3.6. ADAPT Score
3.3.7. MEFIB Index
3.3.8. FAST Score
3.3.9. Cohort-Specific Model and Combination of 6 Biomarkers
3.3.10. Prognostic Factor Model
3.3.11. Top 10 Metabolite Panel
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yu, J.; Marsh, S.; Hu, J.; Feng, W.; Wu, C. The Pathogenesis of Nonalcoholic Fatty Liver Disease: Interplay between Diet, Gut Microbiota, and Genetic Background. Gastroenterol. Res. Pract. 2016, 2016, 2862173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadiparthi, C.; Spatz, M.; Greenberg, S.; Iqbal, U.; Kanna, S.; Satapathy, S.K.; Broder, A.; Ahmed, A. NAFLD Epidemiology, Emerging Pharmacotherapy, Liver Transplantation Implications and the Trends in the United States. J. Clin. Transl. Hepatol. 2020, 8, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Zou, B.; Yeo, Y.H.; Nguyen, V.H.; Cheung, R.; Ingelsson, E.; Nguyen, M.H. Prevalence, characteristics and mortality outcomes of obese, nonobese and lean NAFLD in the United States, 1999–2016. J. Intern. Med. 2020, 288, 139–151. [Google Scholar] [CrossRef]
- Caldwell, S.; Ikura, Y.; Dias, D.; Isomoto, K.; Yabu, A.; Moskaluk, C.; Pramoonjago, P.; Simmons, W.; Scruggs, H.; Rosenbaum, N.; et al. Hepatocellular ballooning in NASH. J. Hepatol. 2010, 53, 719–723. [Google Scholar] [CrossRef] [Green Version]
- Carr, R.M.; Oranu, A.; Khungar, V. Nonalcoholic Fatty Liver Disease: Pathophysiology and Management. Gastroenterol. Clin. N. Am. 2016, 45, 639–652. [Google Scholar] [CrossRef] [Green Version]
- Parthasarathy, G.; Revelo, X.; Malhi, H. Pathogenesis of Nonalcoholic Steatohepatitis: An Overview. Hepatol. Commun. 2020, 4, 478–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Dufour, J.-F.; Scherer, R.; Balp, M.-M.; McKenna, S.J.; Janssens, N.; Lopez, P.; Pedrosa, M. The global epidemiology of nonalcoholic steatohepatitis (NASH) and associated risk factors—A targeted literature review. Endocr. Metab. Sci. 2021, 3, 100089. [Google Scholar] [CrossRef]
- Hayashi, T.; Saitoh, S.; Fukuzawa, K.; Tsuji, Y.; Takahashi, J.; Kawamura, Y.; Akuta, N.; Kobayashi, M.; Ikeda, K.; Fujii, T.; et al. Noninvasive Assessment of Advanced Fibrosis Based on Hepatic Volume in Patients with Nonalcoholic Fatty Liver Disease. Gut Liver 2017, 11, 674–683. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Loomba, R.; Anstee, Q.M.; Rinella, M.E.; Bugianesi, E.; Marchesini, G.; Neuschwander-Tetri, B.A.; Serfaty, L.; Negro, F.; Caldwell, S.H.; et al. Diagnostic modalities for nonalcoholic fatty liver disease, nonalcoholic steatohepatitis, and associated fibrosis. Hepatology 2018, 68, 349–360. [Google Scholar] [CrossRef]
- Lee, T.H.; Peters, J.J. Hepatic Fibrosis: MSD Manual Professional Version. 2022. Available online: https://www.msdmanuals.com/professional/hepatic-and-biliary-disorders/fibrosis-and-cirrhosis/hepatic-fibrosis?query=hepatic%20fibrosis (accessed on 25 July 2022).
- García-Compeán, D.; Villarreal-Pérez, J.Z.; Cavazos, M.E.O.; Lavalle-Gonzalez, F.J.; Borjas-Almaguer, O.D.; Del Cueto-Aguilera, A.N.; González-González, J.A.; Treviño-Garza, C.; Huerta-Pérez, L.; Maldonado-Garza, H.J. Prevalence of liver fibrosis in an unselected general population with high prevalence of obesity and diabetes mellitus. Time for screening? Ann. Hepatol. 2020, 19, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Arab, J.P.; Barrera, F.; Gallego, C.; Valderas, J.P.; Uribe, S.; Tejos, C.; Serrano, C.; Serrano, C.; Huete, Á.; Liberona, J.; et al. High prevalence of undiagnosed liver cirrhosis and advanced fibrosis in type 2 diabetic patients. Ann. Hepatol. 2016, 15, 721–728. [Google Scholar] [PubMed]
- Dvorak, K.; Stritesky, J.; Petrtyl, J.; Vitek, L.; Sroubkova, R.; Lenicek, M.; Smid, V.; Haluzik, M.; Bruha, R. Use of non-invasive parameters of non-alcoholic steatohepatitis and liver fibrosis in daily practice—An exploratory case-control study. PLoS ONE 2014, 9, e111551. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Perseghin, G. Prevalence of NAFLD, MAFLD and associated advanced fibrosis in the contemporary United States population. Liver Int. 2021, 41, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Rockey, D.C.; Bissell, D.M. Noninvasive measures of liver fibrosis. Hepatology 2006, 43 (Suppl. S1), S113–S120. [Google Scholar] [CrossRef]
- Catania, R.; Furlan, A.; Smith, A.D.; Behari, J.; Tublin, M.E.; Borhani, A.A. Diagnostic value of MRI-derived liver surface nodularity score for the non-invasive quantification of hepatic fibrosis in non-alcoholic fatty liver disease. Eur. Radiol. 2021, 31, 256–263. [Google Scholar] [CrossRef]
- Harrison, S.A.; Calanna, S.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.; Sejling, A.S.; Newsome, P.N. Semaglutide for the treatment of non-alcoholic steatohepatitis: Trial design and comparison of non-invasive biomarkers. Contemp. Clin. Trials 2020, 97, 106174. [Google Scholar] [CrossRef]
- Jayakumar, S.; Middleton, M.S.; Lawitz, E.J.; Mantry, P.S.; Caldwell, S.H.; Arnold, H.; Mae Diehl, A.; Ghalib, R.; Elkhashab, M.; Abdelmalek, M.F.; et al. Longitudinal correlations between MRE, MRI-PDFF, and liver histology in patients with non-alcoholic steatohepatitis: Analysis of data from a phase II trial of selonsertib. J. Hepatol. 2019, 70, 133–141. [Google Scholar] [CrossRef]
- Ozturk, A.; Mohammadi, R.; Pierce, T.T.; Kamarthi, S.; Dhyani, M.; Grajo, J.R.; Corey, K.E.; Chung, R.T.; Bhan, A.K.; Chhatwal, J.; et al. Diagnostic Accuracy of Shear Wave Elastography as a Non-Invasive Biomarker of High-Risk Non-Alcoholic Steatohepatitis in Patients with Non-Alcoholic Fatty Liver Disease. Ultrasound Med. Biol. 2020, 46, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.S.; Idowu, M.O.; Stromberg, K.; Sima, A.; Lee, E.; Patel, S.; Ghaus, S.; Driscoll, C.; Sterling, R.K.; John, B.; et al. Diagnostic Performance of Vibration-Controlled Transient Elastography in Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2021, 19, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Dzyubak, B.; Yin, M.; Schlein, A.; Henderson, W.C.; Hooker, J.C.; Delgado, T.I.; Middleton, M.S.; Zheng, L.; Wolfson, T.; et al. MR elastography in nonalcoholic fatty liver disease: Inter-center and inter-analysis-method measurement reproducibility and accuracy at 3T. Eur. Radiol. 2022, 32, 2937–2948. [Google Scholar] [CrossRef] [PubMed]
- Trowell, J.; Alukal, J.; Zhang, T.; Liu, L.; Maheshwari, A.; Yoo, H.Y.; Thuluvath, P.J. How Good Are Controlled Attenuation Parameter Scores from Fibroscan to Assess Steatosis, NASH, and Fibrosis? Dig. Dis. Sci. 2021, 66, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.N.; Fowler, K.J.; Boehringer, A.S.; Montes, V.; Schlein, A.N.; Covarrubias, Y.; Wolfson, T.; Hong, C.W.; Valasek, M.A.; Andre, M.P.; et al. Comparative diagnostic performance of ultrasound shear wave elastography and magnetic resonance elastography for classifying fibrosis stage in adults with biopsy-proven nonalcoholic fatty liver disease. Eur. Radiol. 2022, 32, 2457–2469. [Google Scholar] [CrossRef]
- Balakrishnan, M.; Seth, A.; Cortes-Santiago, N.; Jain, S.; Sood, G.K.; El-Serag, H.B.; Thrift, A.P. External Validation of Four Point-of-Care Noninvasive Scores for Predicting Advanced Hepatic Fibrosis in a Predominantly Hispanic NAFLD Population. Dig. Dis. Sci. 2021, 66, 2387–2393. [Google Scholar] [CrossRef]
- Bril, F.; McPhaul, M.J.; Caulfield, M.P.; Clark, V.C.; Soldevilla-Pico, C.; Firpi-Morell, R.J.; Lai, J.; Shiffman, D.; Rowland, C.M.; Cusi, K. Performance of Plasma Biomarkers and Diagnostic Panels for Nonalcoholic Steatohepatitis and Advanced Fibrosis in Patients with Type 2 Diabetes. Diabetes Care 2020, 43, 290–297. [Google Scholar] [CrossRef]
- Caussy, C.; Ajmera, V.H.; Puri, P.; Hsu, C.L.; Bassirian, S.; Mgdsyan, M.; Singh, S.; Faulkner, C.; Valasek, M.A.; Rizo, E.; et al. Serum metabolites detect the presence of advanced fibrosis in derivation and validation cohorts of patients with non-alcoholic fatty liver disease. Gut 2019, 68, 1884–1892. [Google Scholar] [CrossRef] [Green Version]
- Corey, K.E.; Pitts, R.; Lai, M.; Loureiro, J.; Masia, R.; Osganian, S.A.; Gustafson, J.L.; Hutter, M.M.; Gee, D.W.; Meireles, O.R.; et al. ADAMTSL2 protein and a soluble biomarker signature identify at-risk non-alcoholic steatohepatitis and fibrosis in adults with NAFLD. J. Hepatol. 2022, 76, 25–33. [Google Scholar] [CrossRef]
- Kulkarni, S.; Naz, N.; Gu, H.; Stoll, J.M.; Thompson, M.D.; DeBosch, B.J. A clinical model to predict fibrosis on liver biopsy in paediatric subjects with nonalcoholic fatty liver disease. Clin. Obes. 2021, 11, e12472. [Google Scholar] [CrossRef]
- Marella, H.K.; Reddy, Y.K.; Jiang, Y.; Ganguli, S.; Podila, P.S.B.; Snell, P.D.; Kovalic, A.J.; Cholankeril, G.; Singal, A.K.; Nair, S.; et al. Accuracy of Noninvasive Fibrosis Scoring Systems in African American and White Patients with Nonalcoholic Fatty Liver Disease. Clin. Transl. Gastroenterol. 2020, 11, e00165. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.J.; Leeming, D.J.; Goodman, Z.; Friedman, S.; Frederiksen, P.; Rasmussen, D.G.K.; Vig, P.; Seyedkazemi, S.; Fischer, L.; Torstenson, R.; et al. Comparison of ADAPT, FIB-4 and APRI as non-invasive predictors of liver fibrosis and NASH within the CENTAUR screening population. J. Hepatol. 2021, 75, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Gosai, F.; Siddiqui, M.T.; Gupta, M.; Lopez, R.; Lawitz, E.; Poordad, F.; Carey, W.; McCullough, A.; Alkhouri, N. Accuracy of Noninvasive Fibrosis Scores to Detect Advanced Fibrosis in Patients with Type-2 Diabetes with Biopsy-Proven Nonalcoholic Fatty Liver Disease. J. Clin. Gastroenterol. 2020, 54, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Udelsman, B.V.; Corey, K.; Hutter, M.M.; Chang, D.C.; Witkowski, E.R. Use of noninvasive scores for advanced liver fibrosis can guide the need for hepatic biopsy during bariatric procedures. Surg. Obes. Relat. Dis. 2021, 17, 292–298. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Felix, S.; Jeffers, T.; Younossi, E.; Nader, F.; Pham, H.; Afendy, A.; Cable, R.; Racila, A.; Younoszai, Z.; et al. Performance of the Enhanced Liver Fibrosis Test to Estimate Advanced Fibrosis among Patients with Nonalcoholic Fatty Liver Disease. JAMA Netw. Open 2021, 4, e2123923. [Google Scholar] [CrossRef]
- Jung, J.; Loomba, R.R.; Imajo, K.; Madamba, E.; Gandhi, S.; Bettencourt, R.; Singh, S.; Hernandez, C.; Valasek, M.A.; Behling, C.; et al. MRE combined with FIB-4 (MEFIB) index in detection of candidates for pharmacological treatment of NASH-related fibrosis. Gut 2021, 70, 1946–1953. [Google Scholar] [CrossRef]
- Woreta, T.A.; Van Natta, M.L.; Lazo, M.; Krishnan, A.; Neuschwander-Tetri, B.A.; Loomba, R.; Mae Diehl, A.; Abdelmalek, M.F.; Chalasani, N.; Gawrieh, S.; et al. Validation of the accuracy of the FAST™ score for detecting patients with at-risk nonalcoholic steatohepatitis (NASH) in a North American cohort and comparison to other non-invasive algorithms. PLoS ONE 2022, 17, e0266859. [Google Scholar] [CrossRef]
- Costa-Silva, L.; Ferolla, S.M.; Lima, A.S.; Vidigal, P.V.T.; Ferrari, T.C.A. MR elastography is effective for the non-invasive evaluation of fibrosis and necroinflammatory activity in patients with nonalcoholic fatty liver disease. Eur. J. Radiol. 2018, 98, 82–89. [Google Scholar] [CrossRef]
- Dyvorne, H.A.; Jajamovich, G.H.; Bane, O.; Fiel, M.I.; Chou, H.; Schiano, T.D.; Dieterich, D.; Babb, J.S.; Friedman, S.L.; Taouli, B. Prospective comparison of magnetic resonance imaging to transient elastography and serum markers for liver fibrosis detection. Liver Int. 2016, 36, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Giannini, E.G.; Testa, R.; Savarino, V. Liver enzyme alteration: A guide for clinicians. Can. Med. Assoc. J. 2005, 172, 367–379. [Google Scholar] [CrossRef]
- Decraecker, M.; Dutartre, D.; Hiriart, J.B.; Irles-Depé, M.; Chermak, F.; Foucher, J.; de Lédinghen, V. Long-term prognosis of patients with metabolic (dysfunction)-associated fatty liver disease by non-invasive methods. Aliment. Pharmacol. Ther. 2022, 55, 580–592. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anstee, Q.M.; Lawitz, E.J.; Alkhouri, N.; Wong, V.W.; Romero-Gomez, M.; Okanoue, T.; Trauner, M.; Kersey, K.; Li, G.; Han, L.; et al. Noninvasive Tests Accurately Identify Advanced Fibrosis due to NASH: Baseline Data from the STELLAR Trials. Hepatology 2019, 70, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.; Caussy, C.; Imajo, K.; Chen, J.; Singh, S.; Kaulback, K.; Le, M.D.; Hooker, J.; Tu, X.; Bettencourt, R.; et al. Magnetic Resonance vs. Transient Elastography Analysis of Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin. Gastroenterol. Hepatol. 2019, 17, 630–637.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.D.; Porter, K.K.; Elkassem, A.A.; Sanyal, R.; Lockhart, M.E. Current Imaging Techniques for Noninvasive Staging of Hepatic Fibrosis. AJR Am. J. Roentgenol. 2019, 213, 77–89. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Chalasani, N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Shankar, S.S.; Yates, K.; Daly, E.; Bolognese, J.A.; Neuschwander-Tetri, B.A.; Kowdley, K.V.; Vuppalanchi, R.; Guy, C.A.; Tonascia, J.; et al. Primary Results of the NIMBLE Stage 1-NASH CRN Study of Circulating Biomarkers for Nonalcoholic Steatohepatitis and Its Activity and Fibrosis Stage; American Association for the Study of Liver Diseases: Washington, DC, USA, 2021. [Google Scholar]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Hydes, T.; Brown, E.; Hamid, A.; Bateman, A.C.; Cuthbertson, D.J. Current and Emerging Biomarkers and Imaging Modalities for Nonalcoholic Fatty Liver Disease: Clinical and Research Applications. Clin. Ther. 2021, 43, 1505–1522. [Google Scholar] [CrossRef]
- Monelli, F.; Venturelli, F.; Bonilauri, L.; Manicardi, E.; Manicardi, V.; Rossi, P.G.; Massari, M.; Ligabue, G.; Riva, N.; Schianchi, S.; et al. Systematic review of existing guidelines for NAFLD assessment. Hepatoma Res. 2021, 7, 25. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Younossi, Y.; Golabi, P.; Mishra, A.; Rafiq, N.; Henry, L. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 2020, 69, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Rowe, I.A. Too much medicine: Overdiagnosis and overtreatment of non-alcoholic fatty liver disease. Lancet Gastroenterol. Hepatol. 2018, 3, 66–72. [Google Scholar] [CrossRef]
- Lee, J.; Vali, Y.; Boursier, J.; Spijker, R.; Anstee, Q.M.; Bossuyt, P.M.; Zafarmand, M.H. Prognostic accuracy of FIB-4, NAFLD fibrosis score and APRI for NAFLD-related events: A systematic review. Liver Int. 2021, 41, 261–270. [Google Scholar] [CrossRef]
- Ratziu, V.; Charlotte, F.; Heurtier, A.; Gombert, S.; Giral, P.; Bruckert, E.; Grimaldi, A.; Capron, F.; Poynard, T. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology 2005, 128, 1898–1906. [Google Scholar] [CrossRef]
- Byrne, C.D.; Patel, J.; Scorletti, E.; Targher, G. Tests for diagnosing and monitoring non-alcoholic fatty liver disease in adults. Bmj 2018, 362, k2734. [Google Scholar] [CrossRef] [Green Version]
- Jensen, T.; Wieland, A.; Cree-Green, M.; Nadeau, K.; Sullivan, S. Clinical workup of fatty liver for the primary care provider. Postgrad. Med. 2019, 131, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, N.; Kimura, T.; Tanaka, N.; Yamazaki, T.; Okumura, T.; Kobayashi, H.; Wakabayashi, S.I.; Yamashita, Y.; Sugiura, A.; Pham, J.; et al. 2-Step PLT16-AST44 method: Simplified liver fibrosis detection system in patients with non-alcoholic fatty liver disease. Hepatol. Res. 2022, 52, 352–363. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Published between January 2016 and May 2022 2. Written in English 3. Human studies 4. Original research | 1. Studies with irrelevant outcomes 2. No full-text studies 3. In vitro studies 4. Molecular and genetic studies 5. Editorials, comments, replies, and letters to the author |
| PICO | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | 1. Patients diagnosed with NAFLD 2. Patients diagnosed with NASH 3. Patients diagnosed with significant or advanced liver fibrosis 4. Patients diagnosed with significant or severe liver steatosis 5. Patients diagnosed with liver cirrhosis | 1. Nonhuman population |
| Interventions | 1. Any treatment or management 2. No treatment or management | NA |
| Comparators | 1. Any treatment or management 2. No treatment or management | NA |
| Outcomes | 1. Sensitivity 2. Specificity 3. Positive predictive value 4. Negative predictive value 5. Area under the receiver operating characteristic curve | NA |
| Restrictions | 1. English language 2. Year limitation: 2016–2022 | 1. Genetic studies 2. Editorials 3. Letters and comments to the authors 4. Case reports 5. SLRs, meta-analyses, narrative reviews, guidelines |
| Studies That Evaluated Accuracy of Imaging Techniques | ||||||
| Author | Year | Study Type | Population | Baseline Fibrosis | Imaging Technique | Detection Capabilities |
| Catania et al. [19] | 2021 | Prospective study | 47 NAFLD patients | Fibrosis stage 2: 39% Fibrosis stage 3: 25% Fibrosis stage 4: 19% | MRI-derived LSN score | Significant fibrosis Advanced fibrosis |
| Harrison et al. [20] | 2020 | Prospective study | 288 NASH patients with F1-F3 fibrosis | FIB-4 score, mean (SD): 1.4 (59.3) | VCTE | Significant fibrosis Advanced fibrosis |
| Jayakumar et al. [21] | 2019 | Prospective study | 54 NASH patients with F2-F3 fibrosis | Fibrosis stage 2: 37%Fibrosis stage 3: 67% | MRE | Significant fibrosis Advanced fibrosis (progression and improvement) |
| Ozturk et al. [22] | 2020 | Retrospective study | 116 NAFLD patients | Fibrosis stage 2: 9.4%Fibrosis stage 3: 13.7%Fibrosis stage 4: 2.5% | SWE | Significant fibrosis Advanced fibrosis |
| Siddiqui et al. [23] | 2021 | Prospective study | 99 patients with liver transplantation history | Fibrosis stage 2: 4.0% Fibrosis stage 3: 10.1% Fibrosis stage 4: 7.1% | VCTE | Significant fibrosis Advanced fibrosis |
| Tang et al. [24] | 2022 | Retrospective study | 91 NAFLD patients | Fibrosis stage 2: 7.7% Fibrosis stage 3: 11% Fibrosis stage 4: 5.5% | MRE | Advanced fibrosis |
| Trowell et al. [25] | 2021 | Retrospective study | 217 NAFLD and non-NAFLD patients | Fibrosis stage 2: 24% Fibrosis stage 3: 13% Fibrosis stage 4: 18% | VCTE | Advanced fibrosis |
| Zhang et al. [26] | 2022 | Cross-sectional study | 100 NAFLD patients | Fibrosis stage 2: 5% Fibrosis stage 3: 10% Fibrosis stage 4: 6% | SWE, MRE | Significant fibrosis Advanced fibrosis |
| Studies that evaluated accuracy of established fibrosis scores and biomarkers | ||||||
| Author | Year | Study Type | Population | Baseline Fibrosis | Biomarker | Detection Capabilities |
| Balakrishnan et al. [27] | 2021 | Retrospective cross-sectional study | 99 NAFLD patients | Fibrosis stage 0–2: 62.6% Fibrosis stage 3–4: 37.4% FIB-4 score, mean (SD): In fibrosis stage 0–2: 0.99 (0.55) In fibrosis stage 3–4: 2.23 (1.52) | NFS, FIB-4 index, APRI, BARD score | Significant fibrosis |
| Bril et al. [28] | 2020 | Cross-sectional study | 213 T2DM patients | Fibrosis stage, mean (SD): In no NASH: 0.6 (0.9) In definite NASH: 1.8 (1.0) | NFS, FIB-4 index, APRI, Plasma AST levels FibroTest | Advanced fibrosis |
| Caussy et al. [29] | 2019 | Cross-sectional study | 156 NAFLD patients | FIB-4 score, mean (SD): 1.35 (1.24) | NFS, FIB-4 index | Advanced fibrosis |
| Corey et al. [30] | 2022 | Retrospective chart review | 84 NAFLD patients | Fibrosis stage 2: 25% Fibrosis stage 3: 14% Fibrosis stage 4: 10% | NFS, FIB-4 index | Significant fibrosis |
| Harrison et al. [20] | 2020 | Prospective study | 288 NASH patients | FIB-4 score, mean (SD): 1.4 (59.3) | NFS, FIB-4 index, Plasma AST levels, Plasma ALT levels, GGT levels ELF test | Significant fibrosisAdvanced fibrosis |
| Kulkarni et al. [31] | 2021 | Retrospective study | 55 NAFLD patients | Fibrosis stage 2: 20% Fibrosis stage 3: 7.3% Fibrosis stage 4: 3.6% | GGT levels | Significant fibrosis |
| Marella et al. [32] | 2020 | Retrospective chart review | 907 NAFLD patients | Fibrosis stage 2: 17.9% Advanced fibrosis: 12.8% Fibrosis score, mean (SD): 1.16 (1.13) FIB-4 score, mean (SD): 1.28 (1.75) | NFS, FIB-4 index, APRI | Advanced fibrosis |
| Nielsen et al. [33] | 2021 | Retrospective database study | 517 patients with NASH and fibrosis | Fibrosis stage 2: 21% Fibrosis stage 3: 24% Fibrosis stage 4: 5% | FIB-4 index, APRI, AST/ALT ratio | Significant fibrosisAdvanced fibrosis |
| Singh et al. [34] | 2020 | Retrospective chart review | 1157 adult diabetics with NAFLD | Fibrosis stage 0–2: 68% Fibrosis stage 3–4: 32% | NFS, FIB-4 index, APRI, AST/ALT ratio | Advanced fibrosis |
| Udelsman et al. [35] | 2021 | Retrospective chart review | 2465 patients | Fibrosis stage 3+: 3.4% | NFS, FIB-4 index, APRI | Advanced fibrosis |
| Younossi et al. [36] | 2021 | Retrospective cross-sectional study | 829 NAFLD patients | FIB-4 score, mean (SD): 1.34 (0.97) | ELF test | Advanced fibrosis |
| Studies that evaluated accuracy of novel biomarkers | ||||||
| Author | Year | Study Type | Population | Baseline Fibrosis | Diagnostic Technique | Detection Capabilities |
| Corey et al. [30] | 2022 | Retrospective chart review | 84 NAFLD patients | Fibrosis stage 2: 25% Fibrosis stage 3: 14% Fibrosis stage 4: 10% | NFPP, ADAMTSL2, and these in combination with general clinical features, FIB-4 index, or NFS | Significant fibrosis |
| Bril et al. [28] | 2020 | Cross-sectional study | 213 T2DM patients | Fibrosis stage, mean (SD): In no NASH: 0.6 (0.9) In definite NASH: 1.8 (1.0) | PRO-C3, Cohort-specific model, Combination of 6 biomarkers | Advanced fibrosis |
| Caussy et al. [29] | 2019 | Cross-sectional study | 156 NAFLD patients | FIB-4 score, mean (SD): 1.35 (1.24) | Prognostic factor model, Top 10 metabolite panel | Advanced fibrosis |
| Harrison et al. [20] | 2020 | Prospective study | 288 NASH patients | FIB-4 score, mean (SD): 1.4 (59.3) | CK-18 fragment M30, CK-18 fragment M65, MCP-1 | Significant fibrosisAdvanced fibrosis |
| Kulkarni et al. [31] | 2021 | Retrospective study | 55 NAFLD patients | Fibrosis stage 2: 20% Fibrosis stage 3: 7.3% Fibrosis stage 4: 3.6% | Scoring system | Significant fibrosis |
| Nielsen et al. [33] | 2021 | Retrospective database study | 517 patients with NASH and fibrosis | Fibrosis stage 2: 21% Fibrosis stage 3: 24% Fibrosis stage 4: 5% | PRO-C3, ADAPT score | Significant fibrosisAdvanced fibrosis |
| Jung et al. [37] | 2021 | Prospective study | 238 NAFLD patients | Fibrosis stage 2: 11.3% Fibrosis stage 3: 9.7% Fibrosis stage 4: 7.6% FIB-4 score, mean (SD): 1.5 (1.4) | MEFIB index | Significant fibrosis |
| Woreta et al. [38] | 2022 | Retrospective study | 585 NAFLD patients | Fibrosis stage 2: 20.6% Fibrosis stage 3: 20.7% Fibrosis stage 4: 10.4% | FAST score | Significant fibrosis |
| Vibration-Controlled Transient Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 7.3 kPa | 89.0% | 33.0% | 77.0% | 56.0% | 0.630 |
| Siddiqui et al. [23] | 7.4 kPa | 90.0% | 60.0% | 38.0% | 96.0% | 0.870 |
| 10.5 kPa | 81.0% | 83.0% | 57.0% | 94.0% | ||
| 13.5 kPa | 67.0% | 90.0% | 67.0% | 91.0% | ||
| Shear Wave Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Ozturk et al. [22] | 8.4 kPa | 77.0% | 66.0% | - | - | 0.730 |
| Zhang et al. [26] | 1.49 m/s | 90.5% | 43.0% | 29.7% | 94.4% | 0.810 |
| 1.79 m/s | 47.6% | 91.1% | 58.8% | 86.7% | ||
| Magnetic Resonance Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Zhang et al. [26] | 2.77 kPa | 90.5% | 84.8% | 61.3% | 97.1% | 0.940 |
| 3.06 kPa | 81.0% | 91.1% | 70.8% | 94.7% | ||
| Magnetic Resonance Imaging-Derived Liver Surface Nodularity Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Catania et al. [19] | 2.23 | 72.0% | 62.0% | - | - | 0.800 |
| Vibration-Controlled Transient Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 11.5 kPa | 56.0% | 71.0% | 65.0% | 63.0% | 0.650 |
| Siddiqui et al. [23] | 10.5 kPa | 94.0% | 83.0% | 53.0% | 99.0% | 0.940 |
| 10.5 kPa | 90.0% | 83.0% | 53.0% | 99.0% | ||
| 13.3 kPa | 82.0% | 90.0% | 64.0% | 96.0% | ||
| Trowell et al. [25] | 11.9 kPa 1 | 75.0% | 81.5% | 65.4% | 87.5% | 0.850 |
| 11.9 kPa 2 | 73.7% | 74.5% | 53.8% | 87.5% | 0.780 | |
| Shear Wave Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Ozturk et al. [22] | 8.4 kPa | 84.0% | 70.0% | - | - | 0.820 |
| Zhang et al. [26] | 1.46 m/s | 93.8% | 39.3% | 39.3% | 97.1% | 0.850 |
| 1.78 m/s | 62.5% | 90.5% | 55.6% | 92.7% | ||
| Magnetic Resonance Elastography | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Tang et al. [24] | 3.6 kPa 3 | 93.0% | 95.0% | 78.0% | 99.0% | 0.939 |
| 3.65 kPa 4 | 93.0% | 95.0% | 78.0% | 99.0% | 0.947 | |
| 3.65 kPa 5 | 93.0% | 93.0% | 74.0% | 99.0% | 0.940 | |
| Zhang et al. [26] | 2.77 kPa | 93.8% | 81.0% | 81.0% | 98.6% | 0.950 |
| 3.17 kPa | 81.3% | 90.5% | 61.9% | 96.2% | ||
| Magnetic Resonance Imaging-Derived Liver Surface Nodularity Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Catania et al. [19] | 2.44 | 81.0% | 88.0% | - | - | 0.860 |
| NAFLD Fibrosis Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 36% | 85% | 67% | 62% | 0.640 |
| Harrison et al. [20] | 0.9 | 66% | 52% | 77% | 38% | 0.600 |
| Fibrosis-4 index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 48% | 88% | 76% | 68% | 0.700 |
| Harrison et al. [20] | 1.3 | 64% | 70% | 84% | 44% | 0.690 |
| Nielsen et al. [33] | >1.12 | 71% | 62% | 65% | 69% | 0.710 |
| AST to Platelet Ratio Index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | >0.42 | 57% | 67% | 63% | 61% | 0.660 |
| Enhanced Liver Fibrosis test | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | −0.2 | 62% | 68% | 83% | 42% | 0.690 |
| GGT levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 70.0 U/L | 40% | 72% | 79% | 32% | 0.560 |
| Kulkarni et al. [31] | 65 U/L | 66% | 76% | - | - | - |
| AST/ALT ratio | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | >0.56 | 90% | 25% | 54% | 71% | 0.580 |
| AST levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 42.0 U/L | 57% | 68% | 82% | 38% | 0.630 |
| ALT levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 54.0 U/L | 53% | 60% | 77% | 33% | 0.550 |
| NAFLD Fibrosis Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Balakrishnan et al. [27] | ≥−1.455 | 81.1% | 66.1% | 58.8% | 85.4% | 0.790 |
| ≥0.676 | 32.4% | 95.2% | 80.0% | 70.2% | ||
| Bril et al. [28] | <−1.455 and >0.676 | 91% | 40% | 26% | 95% | 0.640 |
| −0.053 | 68% | 55% | 21% | 90% | ||
| Caussy et al. [29] | - | 90% | 59% | 28% | 97% | 0.840 |
| Harrison et al. [20] | 0.9 | 71% | 48% | 57% | 63% | 0.580 |
| Marella et al. [32] | >0.675 | 57% | 84% | 35% | 93% | 0.810 |
| Singh et al. [34] | >0.676 | 63.7% | 70% | 49.8% | 80.5% | 0.720 |
| ≥(−1.455) | 94.6% | 16.9% | 34.7% | 87.1% | ||
| Udelsman et al. [35] | <−1.455 | 85% | 38% | 5% | 99% | 0.720 |
| >0.675 | 40% | 85% | 9% | 98% | ||
| Fibrosis-4 Index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Balakrishnan et al. [27] | ≥1.3 | 56.8% | 77.4% | 60% | 75% | 0.770 |
| ≥2.67 | 40.5% | 100% | 100% | 73.8% | ||
| Bril et al. [28] | <1.45 and >3.25 | 33% | 99% | 80% | 94% | 0.780 |
| 1.666 | 68% | 75% | 31% | 93% | ||
| Caussy et al. [29] | - | 90% | 39% | 21% | 96% | 0.780 |
| Harrison et al. [20] | 1.3 | 69% | 64% | 65% | 68% | 0.670 |
| Marella et al. [32] | > 2.67 | 29% | 98% | 66% | 90% | 0.880 |
| Nielsen et al. [33] | >1.12 | 87% | 59% | 46% | 92% | 0.790 |
| Singh et al. [34] | >2.67 | 44.1% | 93% | 74.5% | 78.3% | 0.770 |
| ≥1.45 | 72.6% | 64.4% | 48.5% | 83.6% | ||
| Udelsman et al. [35] | >1.30 | 58% | 86% | 13% | 98% | 0.790 |
| >2.67 | 21% | 99% | 55% | 97% | ||
| AST to Platelet Ratio Index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Balakrishnan et al. [27] | ≥1 | 48.7% | 88.7% | 72% | 74.3% | 0.700 |
| Bril et al. [28] | <0.5 and >1.5 | 31% | 99% | 67% | 94% | 0.860 |
| 0.423 | 84% | 75% | 36% | 96% | ||
| Marella et al. [32] | >1.5 | 14% | 98% | 47% | 89% | 0.830 |
| Nielsen et al. [33] | >0.34 | 79% | 51% | 39% | 86% | 0.680 |
| Singh et al. [34] | >1.5 | 16.5% | 97.4% | 74.7% | 71.7% | 0.740 |
| ≥1 | 27.9% | 94.7% | 70.9% | 74% | ||
| Udelsman et al. [35] | >0.98 | 24% | 99% | 65% | 97% | 0.810 |
| BARD Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Balakrishnan et al. [27] | ≥2 | 75.7% | 59.7% | 52.8% | 80.4% | 0.760 |
| Enhanced Liver Fibrosis Test | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | −0.1 | 67% | 63% | 63% | 66% | 0.680 |
| Younossi et al. [36] | 9.8 1 | 57.5% | 88.9% | 62.5% | 88.6% | 0.810 |
| 11.3 1 | 19.5% | 99.1% | 88.0% | 79.2% | ||
| 9.8 2 | 58.2% | 84.1% | 43.0% | 90.7% | 0.790 | |
| 11.3 2 | 17.7% | 99.5% | 87.5% | 85.4% | ||
| FibroTest | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Bril et al. [28] | <0.3 and >0.7 | 17.0% | 98.0% | 40.0% | 92.0% | 0.700 |
| 0.353 | 64.0% | 74.0% | 30.0% | 92.0% | ||
| GGT Levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 68.0 U/L | 49% | 72% | 63% | 59% | 0.620 |
| AST/ALT Ratio | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | >0.78 | 63% | 64% | 42% | 81% | 0.680 |
| Singh et al. [34] | >1.4 | 27.4% | 84.2% | 44.6% | 71.5% | 0.620 |
| ≥1 | 60.7% | 53.3% | 37.6% | 74.5% | ||
| AST Levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Bril et al. [28] | 40 U/L | 77% | 81% | 41% | 96% | 0.850 |
| 38 U/L | 84% | 79% | 40% | 97% | ||
| Harrison et al. [20] | 37 U/L | 73% | 52% | 60% | 67% | 0.660 |
| ALT Levels | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 68.0 U/L | 41% | 74% | 61% | 56% | 0.580 |
| Cytokeratine-18 Fragment M30 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 260 U/L | 90% | 26% | 76% | 50% | 0.560 |
| Cytokeratine-18 Fragment M65 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 545 U/L | 90% | 29% | 77% | 54% | 0.580 |
| Procollagen Type-III N-Terminal Peptide | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | 19.65 ng/mL | 45% | 86% | 76% | 61% | 0.700 |
| Monocyte Chemoattractant Protein 1 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 497.2 | 21% | 87% | 80% | 30% | 0.520 |
| NAFLD Fibrosis Protein Panel | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 64% | 86% | 78% | 76% | 0.830 |
| NAFLD Fibrosis Protein Panel with General Clinical Features | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 70% | 93% | 88% | 80% | 0.870 |
| NAFLD Fibrosis Protein Panel and FIB-4 Index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 73% | 85% | 80% | 80% | 0.870 |
| NAFLD Fibrosis Protein Panel and NFS | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 76% | 85% | 81% | 81% | 0.870 |
| A Disintegrin and Metalloproteinase with Thrombospondin Motifs like 2 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 58% | 91% | 83% | 74% | 0.830 |
| A Disintegrin and Metalloproteinase with Thrombospondin Motifs like 2 with FIB-4 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 67% | 85% | 79% | 76% | 0.830 |
| A Disintegrin and Metalloproteinase with Thrombospondin Motifs like 2 with NFS | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Corey et al. [30] | - | 58% | 90% | 83% | 73% | 0.830 |
| Kulkarni Model | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Kulkarni et al. [31] | 6.13 | 83.3% | 94.6% | - | - | 0.945 |
| ADAPT Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | >6.15 | 64.0% | 75.0% | 71.0% | 68.0% | 0.760 |
| MEFIB Index | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Jung et al. [37] | MRE ≥ 3.3 kPa and FIB-4 index ≥ 1.6 | 50.0% | 99.4% | 83.2% | 83.2% | 0.900 |
| FAST Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Woreta et al. [38] | 0.35 | 91.0% | 50.0% | 51.0% | 90.0% | 0.807 |
| 0.67 | 52.0% | 87.0% | 69.0% | 76.0% | ||
| 0.38 | 90.0% | 53.0% | 52.0% | 90.0% | ||
| 0.72 | 44.0% | 90.0% | 72.0% | 73.0% | ||
| Cytokeratine-18 Fragment M30 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 260 U/L | 94% | 23% | 55% | 80% | 0.590 |
| Cytokeratine-18 Fragment M65 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 545 U/L | 95% | 25% | 56% | 83% | 0.600 |
| Procollagen Type-III N-Terminal Peptide | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Bril et al. [28] | 20 ng/mL | 50% | 96% | 67% | 92% | 0.900 |
| 13.2 ng/mL | 88% | 80% | 43% | 97% | ||
| Nielsen et al. [33] | 13.45 ng/mL | 77% | 59% | 44% | 87% | 0.730 |
| Monocyte Chemoattractant Protein 1 | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Harrison et al. [20] | 245.1 | 93% | 14% | 52% | 67% | 0.510 |
| Cohort-Specific Model (Serum CK-18, Fasting Insulin, Platelets Count, Sex, HbA1c) | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Bril et al. [28] | <−2.613 and >1.015 | 88% | 86% | 57% | 97% | 0.860 |
| −1.369 | 80% | 83% | 45% | 96% | ||
| Prognostic Factor Model | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Caussy et al. [29] | - | 90% | 37% | 20% | 95% | 0.840 |
| Top 10 Metabolite Panel | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Caussy et al. [29] | - | 90% | 79% | 43% | 98% | 0.940 |
| ADAPT Score | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Nielsen et al. [33] | >6.16 | 78% | 69% | 50% | 88% | 0.800 |
| Combination of 6 Biomarkers | ||||||
| Source | Cutoff | Sensitivity | Specificity | PPV | NPV | AUROC |
| Bril et al. [28] | PRO-C3—13.2 ng/mL APRI—0.423 AST—38 units/L FIB-4 index—1.666 FibroTest—0.353 NFS −0.053 | 71% | 94% | 68% | 95% | 0.910 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gosalia, D.; Ratziu, V.; Stanicic, F.; Vukicevic, D.; Zah, V.; Gunn, N.; Halegoua-DeMarzio, D.; Tran, T. Accuracy of Noninvasive Diagnostic Tests for the Detection of Significant and Advanced Fibrosis Stages in Nonalcoholic Fatty Liver Disease: A Systematic Literature Review of the US Studies. Diagnostics 2022, 12, 2608. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112608
Gosalia D, Ratziu V, Stanicic F, Vukicevic D, Zah V, Gunn N, Halegoua-DeMarzio D, Tran T. Accuracy of Noninvasive Diagnostic Tests for the Detection of Significant and Advanced Fibrosis Stages in Nonalcoholic Fatty Liver Disease: A Systematic Literature Review of the US Studies. Diagnostics. 2022; 12(11):2608. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112608
Chicago/Turabian StyleGosalia, Dhaval, Vlad Ratziu, Filip Stanicic, Djurdja Vukicevic, Vladimir Zah, Nadege Gunn, Dina Halegoua-DeMarzio, and Tram Tran. 2022. "Accuracy of Noninvasive Diagnostic Tests for the Detection of Significant and Advanced Fibrosis Stages in Nonalcoholic Fatty Liver Disease: A Systematic Literature Review of the US Studies" Diagnostics 12, no. 11: 2608. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112608