

Clinical Modelling of RVHF Using Pre-Operative Variables: A Direct and Inverse Feature Extraction Technique
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Single Paradigms
2.1.1. Gaussian Process Regression (GPR)
2.1.2. Adaptive Neuro-Fuzzy Inference System (ANFIS)
2.1.3. Generalised Regression Neural Network (GRNN)
2.1.4. Interaction Linear Regression (ILR)
2.2. Hybrid-Based Paradigms
2.3. Grading Metrics of the Models Employed in the Current Study
2.4. Study Description and Validation Strategy for the Models Used
2.5. Model Conceptualisation
3. Results
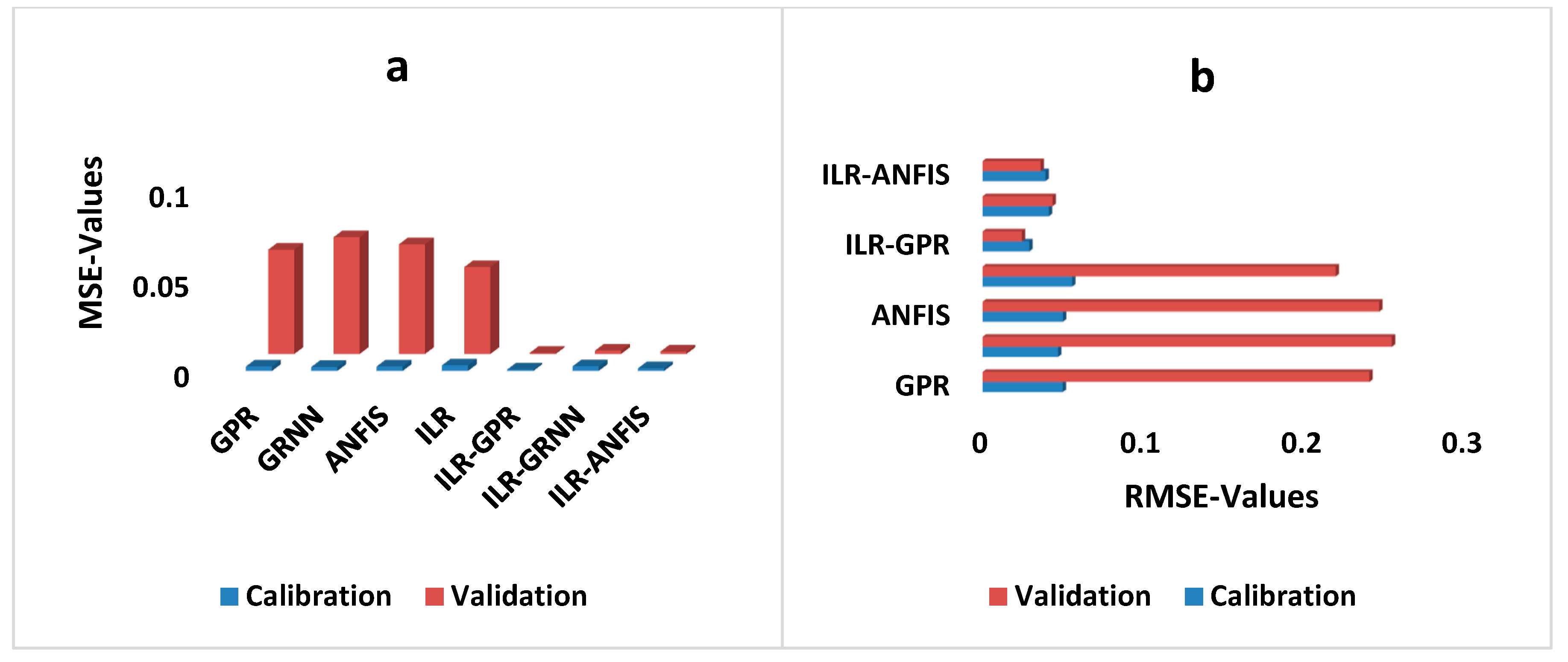
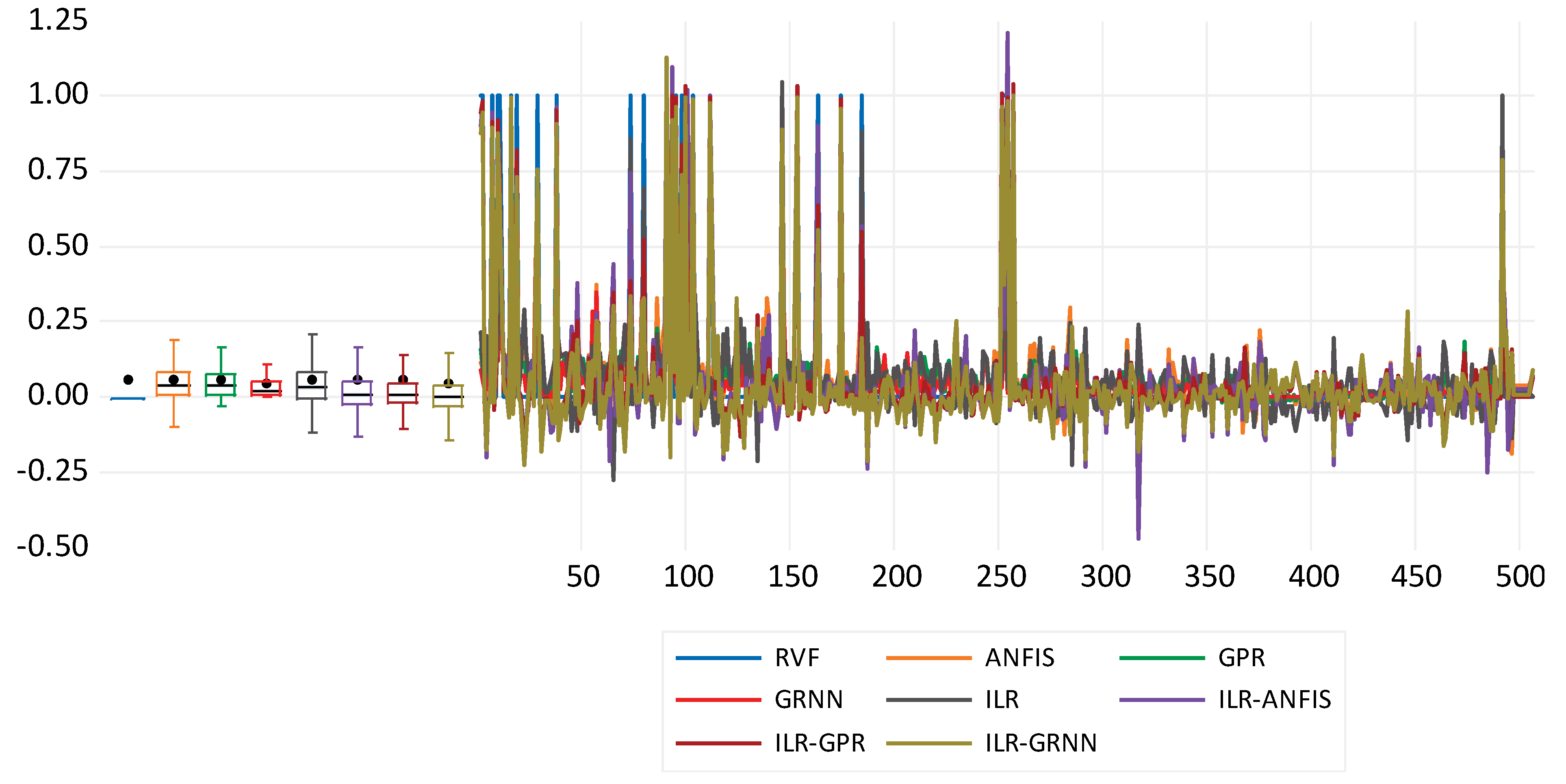
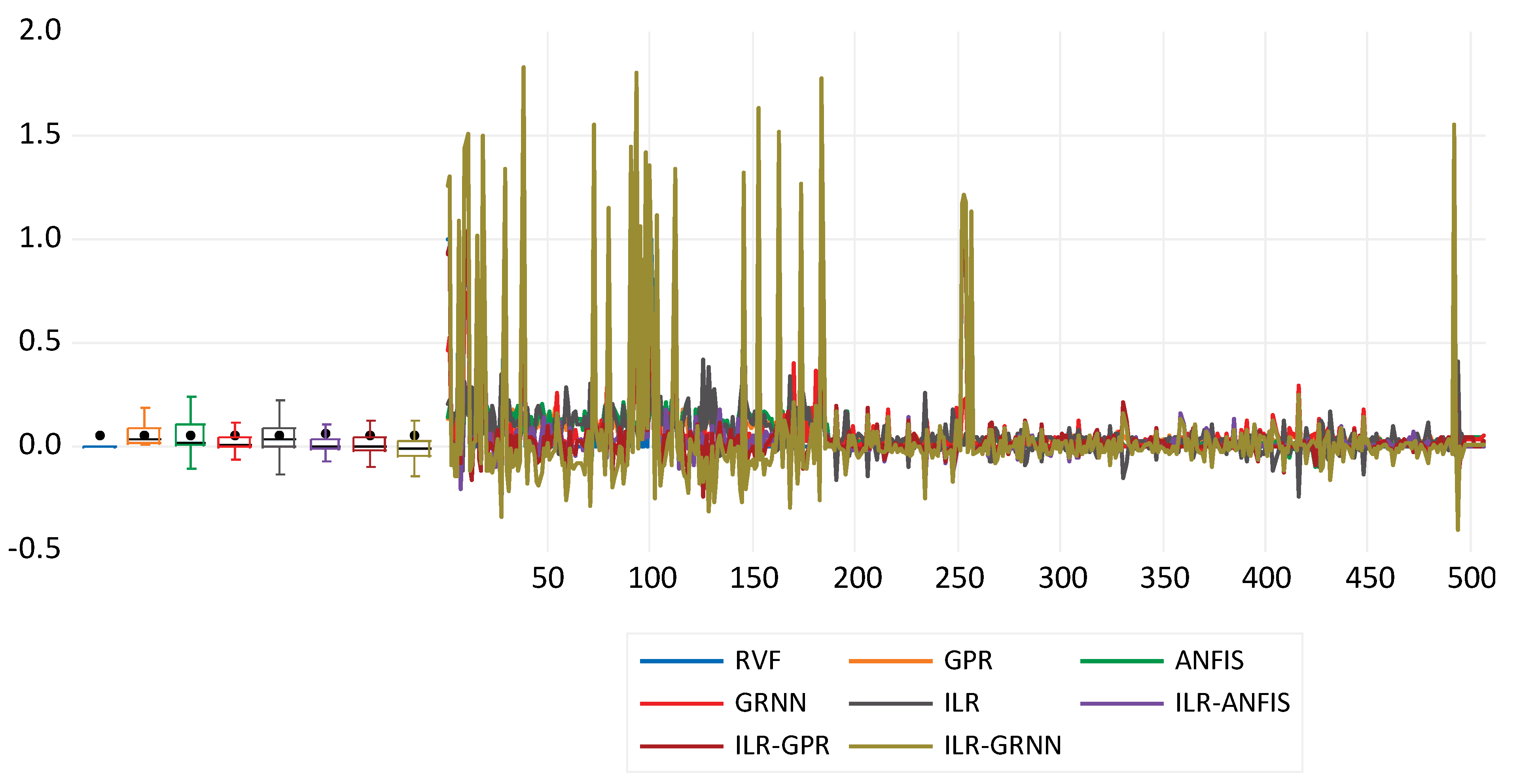
Performance of the Single and Hybrid Paradigms for Modelling RVHF Using Pre-Operative Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sztrymf, B.; Vuillard, C.; Boucly, A.; Artaud-Macari, E.; Sattler, C.; Amar, D.; Jaïs, X.; Sitbon, O.; Humbert, M.; Savale, L.; et al. Right heart failure. ERS Monogr. 2022, 2016, 32–47. [Google Scholar] [CrossRef]
- Andrade, L.; Carazo, M.; Wu, F.; Kim, Y.; Wilson, W. Mechanisms for heart failure in systemic right ventricle. Heart Fail. Rev. 2019, 25, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.M.; Rai, R.; Carrasco, M.; Sam-Odusina, T.; Salandy, S.; Gielecki, J.; Zurada, A.; Loukas, M. An anatomical review of the right ventricle. Transl. Res. Anat. 2020, 17, 100049. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Shah, A.M.; Borlaug, B. Heart Failure With Preserved Ejection Fraction In Perspective. Circ. Res. 2019, 124, 1598–1617. [Google Scholar] [CrossRef] [PubMed]
- Grünig, E.; Eichstaedt, C.A.; Seeger, R.; Benjamin, N. Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis. Diagnostics 2020, 10, 1110. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Wu, W.; He, L.; Gao, L.; Zhang, Y.; Lin, Y.; Qian, M.; Wang, J.; Zhang, L.; Xie, M.; et al. Right Ventricular Longitudinal Strain in Patients with Heart Failure. Diagnostics 2022, 12, 445. [Google Scholar] [CrossRef]
- Zhang, X.; Ruan, B.; Qiao, Z.; Yang, M.; Zhuang, Q.; Wang, J.; Wang, W.; Zheng, Y.; Zhao, H.; Shen, X.; et al. The Balance between the Left and Right Ventricular Deformation Evaluated by Speckle Tracking Echocardiography Is a Great Predictor of the Major Adverse Cardiac Event in Patients with Pulmonary Hypertension. Diagnostics 2022, 12, 2266. [Google Scholar] [CrossRef] [PubMed]
- Manca, P.; Cannatà, A.; Nuzzi, V.; Bromage, D.I.; Varrà, G.G.; Rossi, M.; Ferro, M.D.; Paldino, A.; Gigli, M.; Barbati, G.; et al. Prevalence and Evolution of Right Ventricular Dysfunction Among Different Genetic Backgrounds in Dilated Cardiomyopathy. Can. J. Cardiol. 2021, 37, 1743–1750. [Google Scholar] [CrossRef]
- Patil, S.; Albogami, S.; Hosmani, J.; Mujoo, S.; Kamil, M.A.; Mansour, M.A.; Abdul, H.N.; Bhandi, S.; Ahmed, S.S.S.J. Artificial Intelligence in the Diagnosis of Oral Diseases: Applications and Pitfalls. Diagnostics 2022, 12, 1029. [Google Scholar] [CrossRef]
- Lv, J.; Bin Dong, B.; Lei, H.; Shi, G.; Wang, H.; Zhu, F.; Wen, C.; Zhang, Q.; Fu, L.; Gu, X.; et al. Artificial intelligence-assisted auscultation in detecting congenital heart disease. Eur. Heart J.-Digit. Health 2021, 2, 119–124. [Google Scholar] [CrossRef]
- Romiti, S.; Vinciguerra, M.; Saade, W.; Cortajarena, I.A.; Greco, E. Artificial Intelligence (AI) and Cardiovascular Diseases: An Unexpected Alliance. Cardiol. Res. Pract. 2020, 2020, 4972346. [Google Scholar] [CrossRef]
- Omran, B.A.; Chen, Q.; Jin, R. Comparison of Data Mining Techniques for Predicting Compressive Strength of Environmentally Friendly Concrete. J. Comput. Civ. Eng. 2016, 30, 4016029. [Google Scholar] [CrossRef] [Green Version]
- Cheng, M.-Y.; Huang, C.-C.; Van Roy, A.F. Predicting project success in construction using an evolutionary gaussian process inference model. J. Civ. Eng. Manag. 2013, 19, S202–S211. [Google Scholar] [CrossRef] [Green Version]
- Pal, M.; Deswal, S. Modelling pile capacity using Gaussian process regression. Comput. Geotech. 2010, 37, 942–947. [Google Scholar] [CrossRef]
- Elkiran, G.; Nourani, V.; Abba, S. Multi-step ahead modelling of river water quality parameters using ensemble artificial intelligence-based approach. J. Hydrol. 2019, 577, 123962. [Google Scholar] [CrossRef]
- Wiangkham, A.; Ariyarit, A.; Aengchuan, P. Prediction of the influence of loading rate and sugarcane leaves concentration on fracture toughness of sugarcane leaves and epoxy composite using artificial intelligence. Theor. Appl. Fract. Mech. 2022, 117, 103188. [Google Scholar] [CrossRef]
- Ardejanii, F.D.; Rooki, R.; Shokri, B.J.; Kish, T.E.; Aryafar, A.; Tourani, P. Prediction of Rare Earth Elements in Neutral Alkaline Mine Drainage from Razi Coal Mine, Golestan Province, Northeast Iran, Using General Regression Neural Network. J. Environ. Eng. 2013, 139, 896–907. [Google Scholar] [CrossRef]
- Usman, A.G.; Işik, S.; Abba, S.I. Hybrid data-intelligence algorithms for the simulation of thymoquinone in HPLC method development. J. Iran. Chem. Soc. 2021, 18, 1537–1549. [Google Scholar] [CrossRef]
- Abba, S.I.; Abdulkadir, R.A.; Sammen, S.S.; Usman, A.G.; Meshram, S.G.; Malik, A.; Shahid, S. Comparative implementation between neuro-emotional genetic algorithm and novel ensemble computing techniques for modelling dissolved oxygen concentration. Hydrol. Sci. J. 2021, 66, 1584–1596. [Google Scholar] [CrossRef]
- Ghali, U.M.; Usman, A.G.; Chellube, Z.M.; Degm, M.A.A.; Hoti, K.; Umar, H.; Abba, S.I. Advanced chromatographic technique for performance simulation of anti-Alzheimer agent: An ensemble machine learning approach. SN Appl. Sci. 2020, 2, 1–12. [Google Scholar] [CrossRef]
- Usman, A.G.; Işik, S.; Abba, S.I.; Meriçli, F. Chemometrics-based models hyphenated with ensemble machine learning for retention time simulation of isoquercitrin in Coriander sativum L. using high-performance liquid chromatography. J. Sep. Sci. 2021, 44, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Asadisaghandi, J.; Tahmasebi, P. Comparative evaluation of back-propagation neural network learning algorithms and empirical correlations for prediction of oil PVT properties in Iran oilfields. J. Pet. Sci. Eng. 2011, 78, 464–475. [Google Scholar] [CrossRef]
- Abba, S.; Usman, A.; Işik, S. Simulation for response surface in the HPLC optimization method development using artificial intelligence models: A data-driven approach. Chemom. Intell. Lab. Syst. 2020, 201, 104007. [Google Scholar] [CrossRef]
- Nemati, S.; Fazelifard, M.H.; Terzi, Ö.; Ghorbani, M.A. Estimation of dissolved oxygen using data-driven techniques in the Tai Po River, Hong Kong. Environ. Earth Sci. 2015, 74, 4065–4073. [Google Scholar] [CrossRef]
- Garba Usman, A.; Alhosen, M.; Alsharksi, A.; Muhammed Naibi, A. Applications of Artificial Intelligence-Based Models and Multi-Linear Regression for the Prediction of Thyroid Stimulating Hormone Level in the Human Body Artificial Intelligent Techniques for Stream Flow Modeling View Project Global Platform to Showcase Your Research View project. Available online: https://www.researchgate.net/publication/342571024 (accessed on 3 September 2022).
- Usman, A.G.; Işik, S.; Abba, S.I.; Meriçli, F. Artificial intelligence–based models for the qualitative and quantitative prediction of a phytochemical compound using HPLC method. Turk. J. Chem. 2020, 44, 1339–1351. [Google Scholar] [CrossRef]
- Modeling of Water Treatment Plant Performance Using Artificial Neural Network: Case Study Tamburawa Kano-Nigeria. Available online: https://www.researchgate.net/publication/344380629_Modeling_of_Water_Treatment_Plant_Performance_using_Artificial_Neural_Network_Case_Study_Tamburawa_Kano-Nigeria (accessed on 6 October 2022).
- Gaya, M.S.; Abba, S.I.; Abdu, A.M.; Tukur, A.I.; Saleh, M.A.; Esmaili, P.; Wahab, N.A. Estimation of water quality index using artificial intelligence approaches and multi-linear regression. IAES Int. J. Artif. Intell. (IJ-AI) 2020, 9, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Marrero-Ponce, Y.; Barigye, S.J.; Jorge-Rodríguez, M.E.; Tran-Thi-Thu, T. QSRR prediction of gas chromatography retention indices of essential oil components. Chem. Pap. 2018, 72, 57–69. [Google Scholar] [CrossRef]
- Malami, S.I.; Musa, A.A.; Haruna, S.I.; Aliyu, U.U.; Usman, A.G.; Abdurrahman, M.I.; Bashir, A.; Abba, S.I. Implementation of soft-computing models for prediction of flexural strength of pervious concrete hybridized with rice husk ash and calcium carbide waste. Model. Earth Syst. Environ. 2021, 8, 1933–1947. [Google Scholar] [CrossRef]
- Alamrouni, A.; Aslanova, F.; Mati, S.; Maccido, H.S.; Jibril, A.A.; Usman, A.G.; Abba, S.I. Multi-Regional Modeling of Cumulative COVID-19 Cases Integrated with Environmental Forest Knowledge Estimation: A Deep Learning Ensemble Approach. Int. J. Environ. Res. Public Health 2022, 19, 738. [Google Scholar] [CrossRef]
- Khalid, G.M.; Usman, A.G. Application of data-intelligence algorithms for modeling the compaction performance of new pharmaceutical excipients. Future J. Pharm. Sci. 2021, 7, 1–11. [Google Scholar] [CrossRef]
- Haruna, S.I.; Malami, S.I.; Adamu, M.; Usman, A.G.; Farouk, A.; Ali, S.I.A.; Abba, S.I. Compressive Strength of Self-Compacting Concrete Modified with Rice Husk Ash and Calcium Carbide Waste Modeling: A Feasibility of Emerging Emotional Intelligent Model (EANN) Versus Traditional FFNN. Arab. J. Sci. Eng. 2021, 46, 11207–11222. [Google Scholar] [CrossRef]
- Usman, A.G.; Işik, S.; Abba, S.I. A Novel Multi-model Data-Driven Ensemble Technique for the Prediction of Retention Factor in HPLC Method Development. Chromatographia 2020, 83, 933–945. [Google Scholar] [CrossRef]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Maurya, M.R.; Riyaz, N.U.S.S.; Reddy, M.S.B.; Yalcin, H.C.; Ouakad, H.M.; Bahadur, I.; Al-Maadeed, S.; Sadasivuni, K.K. A review of smart sensors coupled with Internet of Things and Artificial Intelligence approach for heart failure monitoring. Med. Biol. Eng. Comput. 2021, 59, 2185–2203. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operation | RVHF |
|---|---|
| Mean | 0.057312 |
| Median | 0 |
| Mode | 0 |
| Standard Deviation | 0.232668 |
| Kurtosis | 12.64552 |
| Skewness | 3.820412 |
| Range | 1 |
| Minimum | 0 |
| Maximum | 1 |
| Count | 506 |
| (a) Direct | ||||||||||||||
| Variables | mPAP | CVP | tpg | alt | ast | BUN | pre Bili | PT time | pre htc | pre sodium | pre ty | ECMO | preMV | RVHF |
| mPAP | 1 | |||||||||||||
| CVP | 0.42 | 1.00 | ||||||||||||
| tpg | 0.51 | 0.48 | 1.00 | |||||||||||
| alt | −0.05 | −0.04 | −0.08 | 1.00 | ||||||||||
| ast | 0.01 | 0.03 | 0.06 | 0.41 | 1.00 | |||||||||
| BUN | −0.05 | −0.03 | 0.03 | 0.10 | 0.20 | 1.00 | ||||||||
| pre Bilirubin | 0.08 | 0.32 | 0.16 | −0.03 | 0.25 | 0.07 | 1.00 | |||||||
| PT time | 0.06 | 0.02 | 0.09 | 0.11 | 0.00 | 0.07 | 0.04 | 1.00 | ||||||
| pre htc | 0.03 | −0.04 | 0.10 | 0.03 | −0.07 | 0.05 | −0.12 | 0.17 | 1.00 | |||||
| pre sodium | −0.12 | −0.09 | −0.05 | 0.09 | −0.01 | 0.05 | −0.21 | 0.20 | 0.21 | 1.00 | ||||
| pre ty | 0.06 | 0.19 | 0.13 | −0.02 | 0.21 | 0.07 | 0.56 | 0.06 | −0.07 | −0.09 | 1.00 | |||
| ECMO | −0.07 | −0.06 | 0.00 | 0.04 | 0.48 | 0.14 | 0.34 | −0.05 | −0.08 | 0.02 | 0.20 | 1.00 | ||
| preMV | −0.03 | 0.14 | −0.13 | 0.06 | 0.07 | −0.08 | 0.21 | −0.02 | −0.13 | 0.00 | 0.11 | 0.03 | 1.00 | |
| RVHF | 0.02 | 0.00 | 0.05 | 0.03 | 0.07 | 0.07 | 0.01 | 0.15 | 0.01 | 0.16 | 0.02 | 0.10 | 0.01 | 1 |
| (b) Inverse | ||||||||||||||
| Variables | pcw | creatinin | pre INR | pre lvesd | pre lvef | pre my | pre ay | pre spap | pre tapse | IABP | RVHF | |||
| pcw | 1 | |||||||||||||
| creatinin | 0.14 | 1.00 | ||||||||||||
| pre INR | 0.16 | 0.60 | 1.00 | |||||||||||
| pre lvesd | 0.11 | 0.38 | 0.79 | 1.00 | ||||||||||
| pre lvef | 0.07 | 0.09 | −0.16 | −0.33 | 1.00 | |||||||||
| pre my | 0.05 | 0.08 | 0.00 | −0.11 | 0.21 | 1.00 | ||||||||
| pre ay | 0.12 | 0.30 | 0.58 | 0.74 | −0.28 | −0.05 | 1.00 | |||||||
| pre spap | 0.16 | −0.17 | −0.27 | −0.28 | 0.20 | 0.08 | −0.20 | 1.00 | ||||||
| pre tapse | 0.01 | −0.16 | −0.28 | −0.32 | 0.24 | 0.05 | −0.22 | 0.25 | 1.00 | |||||
| IABP | 0.10 | 0.31 | 0.66 | 0.83 | −0.37 | −0.10 | 0.80 | −0.28 | −0.27 | 1.00 | ||||
| RVHF | −0.03 | −0.04 | −0.04 | −0.03 | −0.03 | −0.24 | −0.02 | 0.00 | −0.01 | −0.03 | 1.00 | |||
| Calibration | ||||
| Models | DC | PC | MSE | RMSE |
| GPR | 0.419 | 0.647 | 0.002 | 0.050 |
| GRNN | 0.485 | 0.697 | 0.002 | 0.047 |
| ANFIS | 0.416 | 0.645 | 0.003 | 0.050 |
| ILR | 0.275 | 0.525 | 0.003 | 0.056 |
| ILR–GPR | 0.862 | 0.928 | 0.001 | 0.029 |
| ILR–GRNN | 0.777 | 0.882 | 0.003 | 0.041 |
| ILR–ANFIS | 0.813 | 0.902 | 0.001 | 0.039 |
| Validation | ||||
| GPR | 0.201 | 0.449 | 0.058 | 0.241 |
| GRNN | 0.106 | 0.325 | 0.065 | 0.255 |
| ANFIS | 0.160 | 0.400 | 0.061 | 0.247 |
| ILR | 0.335 | 0.578 | 0.048 | 0.220 |
| ILR–GPR | 0.861 | 0.928 | 0.001 | 0.024 |
| ILR–GRNN | 0.559 | 0.748 | 0.002 | 0.044 |
| ILR–ANFIS | 0.696 | 0.834 | 0.001 | 0.036 |
| Calibration | ||||
| DC | PC | MSE | RMSE | |
| GPR | 0.103 | 0.321 | 0.065 | 0.255 |
| GRNN | 0.673 | 0.820 | 0.024 | 0.154 |
| ANFIS | 0.063 | 0.251 | 0.068 | 0.261 |
| ILR | 0.179 | 0.423 | 0.060 | 0.244 |
| ILR–GPR | 0.898 | 0.947 | 0.007 | 0.086 |
| ILR–GRNN | 0.709 | 0.842 | 0.021 | 0.146 |
| ILR–ANFIS | 0.906 | 0.952 | 0.007 | 0.082 |
| Validation | ||||
| GPR | 0.419 | 0.647 | 0.002 | 0.050 |
| GRNN | 0.673 | 0.820 | 0.001 | 0.037 |
| ANFIS | 0.537 | 0.733 | 0.002 | 0.045 |
| ILR | 0.472 | 0.687 | 0.002 | 0.048 |
| ILR–GPR | 0.802 | 0.896 | 0.001 | 0.029 |
| ILR–GRNN | 0.437 | 0.661 | 0.002 | 0.049 |
| ILR–ANFIS | 0.929 | 0.964 | 0.000 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uzun Ozsahin, D.; Balcioglu, O.; Usman, A.G.; Ikechukwu Emegano, D.; Uzun, B.; Abba, S.I.; Ozsahin, I.; Yagdi, T.; Engin, C. Clinical Modelling of RVHF Using Pre-Operative Variables: A Direct and Inverse Feature Extraction Technique. Diagnostics 2022, 12, 3061. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123061
Uzun Ozsahin D, Balcioglu O, Usman AG, Ikechukwu Emegano D, Uzun B, Abba SI, Ozsahin I, Yagdi T, Engin C. Clinical Modelling of RVHF Using Pre-Operative Variables: A Direct and Inverse Feature Extraction Technique. Diagnostics. 2022; 12(12):3061. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123061
Chicago/Turabian StyleUzun Ozsahin, Dilber, Ozlem Balcioglu, Abdullahi Garba Usman, Declan Ikechukwu Emegano, Berna Uzun, Sani Isah Abba, Ilker Ozsahin, Tahir Yagdi, and Cagatay Engin. 2022. "Clinical Modelling of RVHF Using Pre-Operative Variables: A Direct and Inverse Feature Extraction Technique" Diagnostics 12, no. 12: 3061. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123061