
Deep Learning Applications in Computed Tomography Images for Pulmonary Nodule Detection and Diagnosis: A Review


Abstract
:1. Introduction
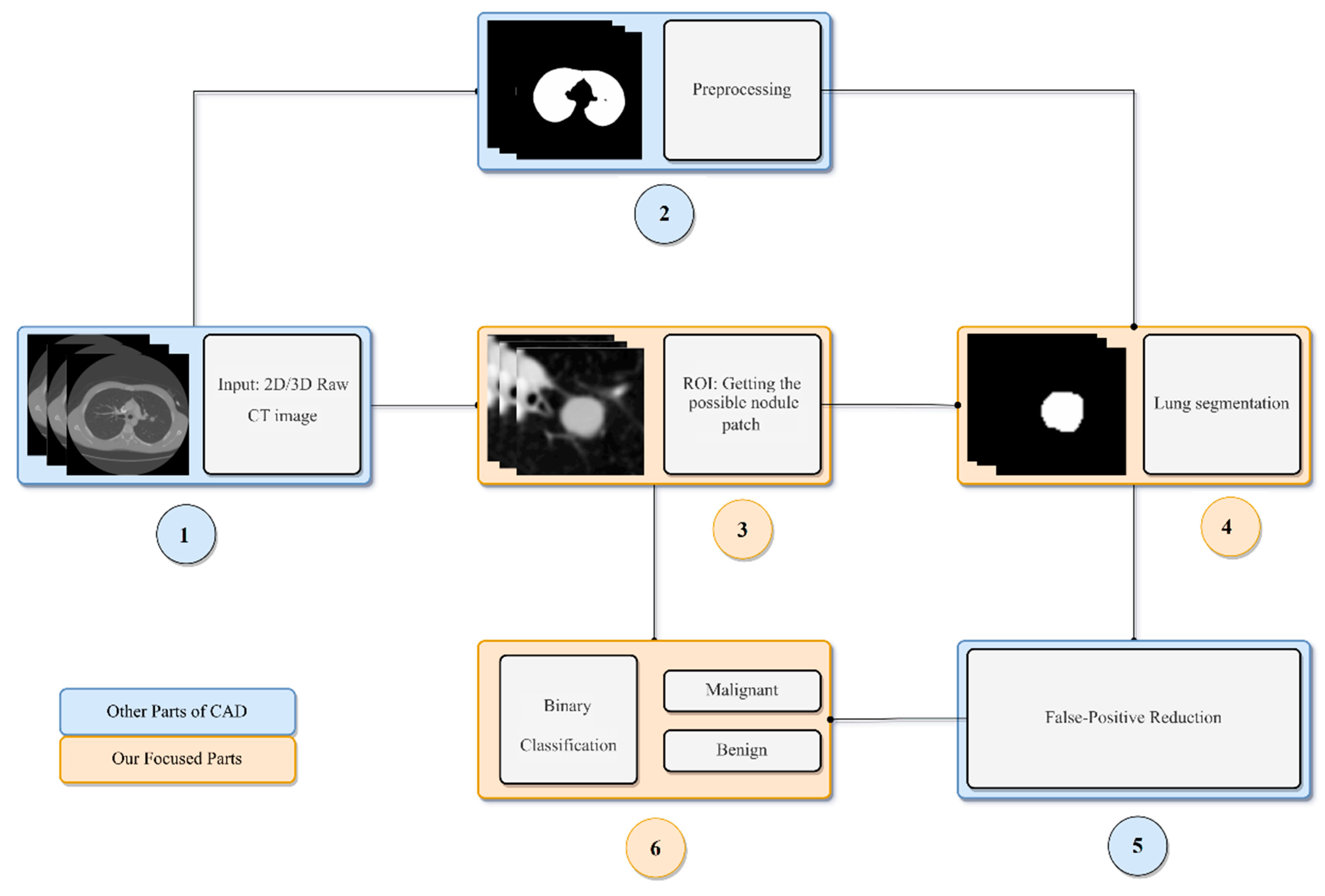
2. General CAD Framework for Detection and Diagnosis of Pulmonary Nodules
3. Datasets
4. Lung Nodule Evaluation Metrics
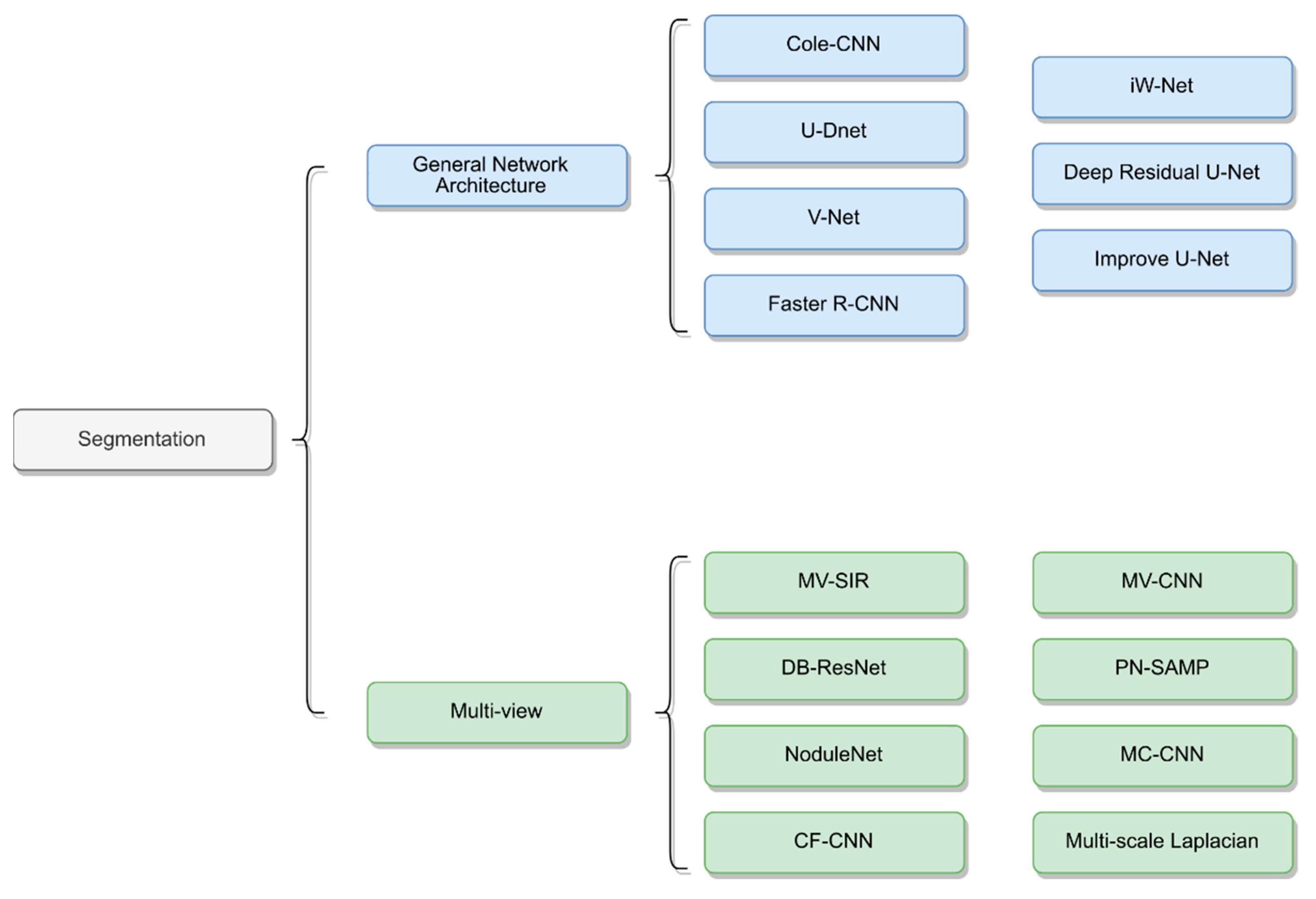
5. Lung Nodule Segmentation
5.1. General Neural Network Architecture
5.2. Multiview CNN Architecture
5.3. Segmentation Based on Lung Nodule Type

{kind=link}
{kind=link}
| Study | Year | Architecture | Dataset | Approach | Performance |
|---|---|---|---|---|---|
| Pezzano et al. [65] | 2021 | CoLe-CNN | LIDC-IDRI | 2D Based U-Net Inception-v4 architecture Mean Square Error function | F1 = 86.1 IoU = 76.6 |
| Dong et al. [67] | 2020 | MV-SIR | LIDC-IDRI | 2D/3D Residual block Secondary input Multi views Voxel heterogeneity (VH) Shape heterogeneity (SH) | ASD = 7.2 ± 3.3 HSD = 129.3 ± 53.3 DSC = 92.6 ± 3.5 PPV = 93.6 ± 2.2 SEN = 98.1 ± 11.3 |
| Keetha et al. [54] | 2020 | U-DNet | LUNA16 | 2D Based U-Net Bi-FPN Efficient-Det Mish activity function | DSC = 82.82 ± 11.71 SEN = 92.24 ± 14.14 PPV = 78.92 ± 17.52 |
| Cao et al. [72] | 2020 | DB-ResNet | LIDC-IDRI | 2D/3D ResNet CIP Multiview Multiscale Central Intensity-Pooling | DSC = 82.74 ± 10.19 ASD = 19 ± 21 SEN = 89.35 ± 11.79 PPV = 79.64 ± 13.34 |
| Kumar el al. [55] | 2020 | V-Net | LUNA16 | 3D V-Net PReLU Only fully convolutional lays | DSC = 96.15 |
| Usman et al. [56] | 2020 | Adaptive ROI with Multi-view Residual Learning | LIDC-IDRI | 2D/3D the Deep Residual U-Net Adaptive ROI Multiview | SEN = 91.62 PPV = 88.24 DSC = 87.55 |
| Tang et al. [74] | 2019 | NoduleNet | LIDC-IDRI | 3D Multitask Residual-block Detection, FPR, segmentation Different loss function | DSC = 83.10 CPM = 87.27 |
| Huang et al. [57] | 2019 | Faster R-CNN | LUNA16 | 2D Faster RCNN Merge overlap FP reduction Based FCN | ACC = 91.4 DSC = 79.3 |
| Aresta et al. [58] | 2019 | iW-Net | LIDC-IDRI | 3D Based U-Net two points in the nodule boundary none heavy pre-processing steps augmentation | IoU = 55 |
| Hesamian et al. [75] | 2019 | Atrous convolution | LIDC-IDRI | 2D Atrous convolution Residual Network Weight loss Normalize to 0, 255 | DSC = 81.24 Precision = 79.75 |
| Liu et al. [76] | 2018 | Mask R-CNN | LIDC-IDRI | 2D Backbone: ResNet101, FPN transfer learning RPN FCN | 73.34 mAP 79.65 mAP |
| Khosravan et al. [77] | 2018 | Semi-supervised multitask learning | LUNA16 | 3D Data augmentation Semi-supervised FP reduction | SEN = 98 DSC = 91 |
| Wu et al. [53] | 2018 | PN-SAMP | LIDC-IDRI | 3D 3D U-Net WW/WC Dice coefficient loss Segmentation, classification | DSC = 73.98 |
| Tong et al. [59] | 2018 | Improved U-NET network | LUNA16 | 2D U-Net Modify residual block Obtain lung parenchyma | DSC = 73.6 |
| Zhao et al. [60] | 2018 | 3D U-Net and Contextual Convolutional Neural Network | LIDC-IDRI | 3D 3D U-Net GAN Morphological methods Residual block Inception structure | None |
| Wang et al. [66] | 2017 | MV-CNN | LIDC-IDRI | 2D/3D Mutilview A multiscale patch strategy | SEN = 83.72 PPV = 77.59 DSC = 77.67 |
| Wang et al. [69] | 2017 | CF-CNN | LIDC-IDRI/GDGH | 2D/3D Central pooling 3D patch 2D views A sampling method Two datasets | LIDC: DSC = 82.15 ± 10.76 SEN = 92.75 ± 12.83 PPV = 75.84 ± 13.14 GDGH: DSC = 80.02 ± 11.09 SEN = 83.19 ± 15.22 PPV = 79.30 ± 12.09 |
6. Classification
6.1. Classification as Nodule or Non-Nodule
6.2. Classification as Benign or Malignant
| Year | Author | Method | Performance |
|---|---|---|---|
| 2021 | Ge Zhang [94] |
| ACC = 92.4% SEN = 87.0% SPEC = 96.0% |
| 2020 | Akila Agnes [92] |
| SEN = 81% SPEC = 91.9% Precision = 87.8% ACC = 87.26% AUC = 0.944 |
| 2020 | Rekka Mastouri [81] |
| ACC = 91.99% SEN = 91.85% SPEC = 92.27% F1-score = 93.76% FPR = 7.72% |
| 2020 | Hong Liu [98] |
| SEN = 0.837% SPC = 0.939% ACC = 0.906% AUC = 0.939% |
| 2020 | Kai Xia [99] |
| ACC = 91.9% SEN = 91.3% FP rate = 8.0% F1-score = 91.0% |
| 2020 | Wu et al. [78] |
| ACC = 98.23% SEN = 97.7% SPEC = 98.35% F1 = 98.06% Precision = 98.64% FPR = 1.65% |
| 2020 | Ali et al. [83] |
| ACC = 96.69% ± 0.72% Error rate = 3.3% ± 0.72% AUC = 99.11% ± 0.45% SEN = 97.19% ± 0.57% |
| 2019 | Yang An [96] |
| ACC = 89.6% |
| 2019 | Zhang Li [97] |
| ACC = 93.68% SEN = 95.17% SPEC = 93.92% |
| 2019 | Tran et al. [79] |
| ACC = 97.2% SEN = 96.0% SPEC = 97.3% |
| 2019 | Al-Shabi et al. [73] |
| AUC = 95.62% ACC = 88.46% Precision = 87.38% SEN = 88.66% |
| 2019 | Al-Shabi et al. [84] |
| AUC = 93.15% ACC = 92.57% Precision = 91.85% SEN = 92.21% |
| 2019 | Guobin Zhang [95] |
| AUC = 0.9563 ACC = 91.67% |
| 2018 | Shiwen Shen [93] |
| AUC = 0.856 ACC = 0.842 SEN = 0.705 SPEC = 0.889 |
| 2018 | Dey et al. [85] |
| TPR = 90.47% TNR = 90.33% PPV = 90.55% AUC = 95.48% ACC = 90.40% |
| 2018 | Wu et al. [53] |
| ACC = 97.58% |
| 2018 | Zhao et al. [60] |
| None |
| 2017 | Nibali et al. [86] |
| SEN = 91.07% SPEC = 88.64 Precision = 89.35% AUC = 94.59% ACC = 89.90% |
| 2017 | Liu et al. [87] |
| SEN = 90.18% SPEC = 100% Error rate = 5.41% AUC = 0.981 |
| 2016 | Li et al. [80] |
| ACC = 86.4% SEN = 89.0% |
| 2016 | Shen et al. [70] |
| ACC = 87.14% AUC = 0.93 SEN = 0.77 SPEC = 0.93 |
| 2015 | Kumar et al. [88] |
| ACC = 75.01% SEN = 83.35% FP = 0.39 FP/patient |
7. Challenges and Future Perspectives
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bankier, A.A.; MacMahon, H.; Goo, J.M.; Rubin, G.; Schaefer-Prokop, C.M.; Naidich, D. Recommendations for Measuring Pulmonary Nodules at CT: A Statement from the Fleischner Society. Radiology 2017, 285, 584–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ELCAP Public Lung Image Database. Available online: http://www.via.cornell.edu/lungdb.html (accessed on 21 January 2022).
- Choi, W.J.; Choi, T.S. Automated pulmonary nodule detection based on three-dimensional shape-based feature descriptor. Comput. Methods Programs Biomed. 2014, 113, 37–54. [Google Scholar] [CrossRef] [PubMed]
- Peloschek, P.; Sailer, J.; Weber, M.; Herold, C.J.; Prokop, M.; Schaefer-Prokop, C. Pulmonary Nodules: Sensitivity of Maximum Intensity Projection versus That of Volume Rendering of 3D Multidetector CT Data. Radiology 2007, 243, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Park, C.M.; Koh, J.M.; Lee, S.M.; Goo, J.M. Pulmonary subsolid nodules: What radiologists need to know about the imaging features and management strategy. Diagn. Interv. Radiol. 2013, 20, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Radiopedia, Pulmonary Nodule. 2020. Available online: https://radiopaedia.org/articles/pulmonary-nodule-1 (accessed on 21 January 2022).
- Revel, M.P.; Bissery, A.; Bienvenu, M.; Aycard, L.; Lefort, C.; Frija, G. Are two-dimensional CT measurements of small noncalcified pulmonary nodules reliable? Radiology 2004, 231, 453–458. [Google Scholar] [CrossRef]
- Han, D.; Heuvelmans, M.A.; Oudkerk, M. Volume versus diameter assessment of small pulmonary nodules in CT lung cancer screening. Transl. Lung Cancer Res. 2017, 6, 52. [Google Scholar] [CrossRef] [Green Version]
- Henschke, C.I.; McCauley, D.I.; Yankelevitz, D.F.; Naidich, D.P.; McGuinness, G.; Miettinen, O.S.; Libby, D.M.; Pasmantier, M.W.; Koizumi, J.; Altorki, N.K.; et al. Early Lung Cancer Action Project: Overall design and findings from baseline screening. Lancet 1999, 354, 99–105. [Google Scholar] [CrossRef]
- Castellino, R.A. Computer aided detection (CAD): An overview. Cancer Imaging 2005, 5, 17–19. [Google Scholar] [CrossRef] [Green Version]
- McCarville, M.B.; Lederman, H.M.; Santana, V.M.; Daw, N.C.; Shochat, S.J.; Li, C.-S.; Kaufman, R.A. Distinguishing benign from malignant pulmonary nodules with helical chest CT in children with malignant solid tumors. Radiology 2006, 239, 514–520. [Google Scholar] [CrossRef]
- Singh, S.; Maxwell, J.; Baker, J.A.; Nicholas, J.L.; Lo, J.Y. Computer-aided Classification of Breast Masses: Performance and Interobserver Variability of Expert Radiologists versus Residents. Radiology 2011, 258, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Giger, M.L.; Karssemeijer, N.; Schnabel, J.A. Breast image analysis for risk assessment, detection, diagnosis, and treatment of cancer. Annu. Rev. Biomed. Eng. 2013, 15, 327–357. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.; Yang, Y.S.; Moon, W.K.; Kim, H.C. Computer-aided diagnosis of solid breast nodules: Use of an artificial neural network based on multiple sonographic features. IEEE Trans. Med. Imaging 2004, 23, 1292–1300. [Google Scholar] [CrossRef]
- Way, T.W.; Sahiner, B.; Chan, H.-P.; Hadjiiski, L.; Cascade, P.N.; Chughtai, A.; Bogot, N.; Kazerooni, E. Computer-aided diagnosis of pulmonary nodules on CT scans: Improvement of classification performance with nodule surface features. Med. Phys. 2009, 36, 3086–3098. [Google Scholar] [CrossRef] [Green Version]
- Way, T.W.; Hadjiiski, L.M.; Sahiner, B.; Chan, H.P.; Cascade, P.N.; Kazerooni, E.A.; Zhou, C.; Bogot, N. Computer-aided diagnosis of pulmonary nodules on CT scans: Segmentation and classification using 3D active contours. Med. Phys. 2006, 33, 2323–2337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giger, M.L.; Ahn, N.; Doi, K.; MacMahon, H.; Metz, C.E. Computerized detection of pulmonary nodules in digital chest images: Use of morphological filters in reducing false-positive detections. Med. Phys. 1990, 17, 861–865. [Google Scholar] [CrossRef]
- Ying, W.; Cunxi, C.; Tong, J.; Xinhe, X. Segmentation of regions of interest in lung CT images based on 2-D OTSU optimized by genetic algorithm. In Proceedings of the 2009 Chinese Control and Decision Conference, Guilin, China, 17–19 June 2009; pp. 5185–5189. [Google Scholar]
- Helen, R.; Kamaraj, N.; Selvi, K.; Raman, V.R. Segmentation of pulmonary parenchyma in CT lung images based on 2D Otsu optimized by PSO. In Proceedings of the International Conference on Emerging Trends in Electrical and Computer Technology, Nagercoil, India, 23–24 March 2011; pp. 536–541. [Google Scholar]
- Liu, Y.; Wang, Z.; Guo, M.; Li, P. Hidden conditional random field for lung nodule detection. In Proceedings of the 2014 IEEE International Conference on Image Processing (ICIP), Paris, France, 27–30 October 2014; pp. 3518–3521. [Google Scholar]
- John, J.; Mini, M. Multilevel Thresholding Based Segmentation and Feature Extraction for Pulmonary Nodule Detection. Procedia Technol. 2016, 24, 957–963. [Google Scholar] [CrossRef] [Green Version]
- Teramoto, A.; Fujita, H.; Yamamuro, O.; Tamaki, T. Automated detection of pulmonary nodules in PET/CT images: Ensemble false-positive reduction using a convolutional neural network technique. Med. Phys. 2016, 43, 2821–2827. [Google Scholar] [CrossRef] [PubMed]
- Mastouri, R.; Neji, H.; Hantous-Zannad, S.; Khlifa, N. A morphological operation-based approach for Sub-pleural lung nodule detection from CT images. In Proceedings of the 2018 IEEE 4th Middle East Conference on Biomedical Engineering (MECBME), Tunis, Tunisia, 28–30 March 2018; pp. 84–89. [Google Scholar]
- Santos, A.M.; Filho, A.O.D.C.; Silva, A.C.; de Paiva, A.C.; Nunes, R.A.; Gattass, M. Automatic detection of small lung nodules in 3D CT data using Gaussian mixture models, Tsallis entropy and SVM. Eng. Appl. Artif. Intell. 2014, 36, 27–39. [Google Scholar] [CrossRef]
- Orozco, H.M.; Villegas, O.O.V.; Sánchez, V.G.C.; Domínguez, H.D.J.O.; Alfaro, M.D.J.N. Automated system for lung nodules classification based on wavelet feature descriptor and support vector machine. Biomed. Eng. Online 2015, 14, 9. [Google Scholar] [CrossRef] [Green Version]
- Lu, L.; Tan, Y.; Schwartz, L.H.; Zhao, B. Hybrid detection of lung nodules on CT scan images. Med. Phys. 2015, 42, 5042–5054. [Google Scholar] [CrossRef] [PubMed]
- Farahani, F.V.; Ahmadi, A.; Zarandi, M.F. Lung nodule diagnosis from CT images based on ensemble learning. In Proceedings of the 2015 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Niagara Falls, ON, Canada, 12–15 August 2015; pp. 1–7. [Google Scholar]
- Klik MA, J.; v Rikxoort, E.M.; Peters, J.F.; Gietema, H.A.; Prokop, M.; v Ginneken, B. Improved classification of pulmonary nodules by automated detection of benign subpleural lymph nodes. In Proceedings of the 3rd IEEE International Symposium on Biomedical Imaging: Nano to Macro; IEEE: Arlington, VA, USA, 6–9 April 2006; pp. 494–497. [Google Scholar]
- Froz, B.R.; Filho, A.O.D.C.; Silva, A.C.; Paiva, A.; Nunes, R.A.; Gattass, M. Lung nodule classification using artificial crawlers, directional texture and support vector machine. Expert Syst. Appl. 2017, 69, 176–188. [Google Scholar] [CrossRef]
- Wu, J.; Qian, T. A survey of pulmonary nodule detection, segmentation and classification in computed tomography with deep learning techniques. J. Med. Artif. Intell. 2019, 2, 1–12. [Google Scholar] [CrossRef]
- Liu, K.; Li, Q.; Ma, J.; Zhou, Z.; Sun, M.; Deng, Y.; Tu, W.; Wang, Y.; Fan, L.; Liu, S.; et al. Evaluating a fully automated pulmonary nodule detection approach and its impact on radiologist performance. Radiol. Artif. Intell. 2019, 1, e180084. [Google Scholar] [CrossRef]
- Shen, W.; Zhou, M.; Yang, F.; Yang, C.; Tian, J. Multiscale convolutional neural networks for lung nodule classification. In Proceedings of the International Conference on Information Processing in Medical Imaging 2014, Isle of Skye, UK, 28 June–3 July 2014; Springer: Cham, Switzerland, 2015; pp. 588–599. [Google Scholar]
- Ciompi, F.; Chung, K.; Van Riel, S.J.; Setio, A.A.A.; Gerke, P.K.; Jacobs, C. Towards automatic pulmonary nodule management in lung cancer screening with deep learning. Sci. Rep. 2017, 7, 46479. [Google Scholar] [CrossRef] [PubMed]
- Causey, J.; Zhang, J.; Ma, S.; Jiang, B.; Qualls, J.A.; Politte, D.G.; Prior, F.W.; Zhang, S.; Huang, X. Highly accurate model for prediction of lung nodule malignancy with CT scans. Sci. Rep. 2018, 8, 9286. [Google Scholar] [CrossRef]
- Hua, K.L.; Hsu, C.H.; Hidayati, S.C.; Cheng, W.H.; Chen, Y.J. Computer-aided classification of lung nodules on computed tomography images via deep learning technique. OncoTargets Ther. 2015, 8, 2015–2022. [Google Scholar]
- Dhara, A.K.; Mukhopadhyay, S.; Khandelwal, N. Computer-aided detection and analysis of pulmonary nodule from CT images: A survey. IETE Tech. Rev. 2012, 29, 265. [Google Scholar] [CrossRef]
- Sluimer, I.; Schilham, A.; Prokop, M.; Van Ginneken, B. Computer analysis of computed tomography scans of the lung: A survey. IEEE Trans. Med. Imaging 2006, 25, 385–405. [Google Scholar] [CrossRef] [PubMed]
- Valente, I.R.S.; Cortez, P.C.; Neto, E.C.; Soares, J.M.; Albuquerque, V.H.C.; Tavares, J.M.R. Automatic 3D pulmonary nodule detection in CT images: A survey. Comput. Methods Programs Biomed. 2015, 124, 91–107. [Google Scholar] [CrossRef] [Green Version]
- Halder, A.; Dey, D.; Sadhu, A.K. Lung Nodule Detection from Feature Engineering to Deep Learning in Thoracic CT Images: A Comprehensive Review. J. Digit. Imaging 2020, 33, 655–677. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Jiang, S.; Yang, Z.; Gong, L.; Ma, X.; Zhou, Z.; Bao, C.; Liu, Q. Automatic nodule detection for lung cancer in CT images: A review. Comput. Biol. Med. 2018, 103, 287–300. [Google Scholar] [CrossRef]
- Gu, Y.; Chi, J.; Liu, J.; Yang, L.; Zhang, B.; Yu, D.; Zhao, Y.; Lu, X. A survey of computer-aided diagnosis of lung nodules from CT scans using deep learning. Comput. Biol. Med. 2021, 137, 104806. [Google Scholar] [CrossRef] [PubMed]
- Monkam, P.; Qi, S.; Ma, H.; Gao, W.; Yao, Y.; Qian, W. Detection and classification of pulmonary nodules using convolutional neural networks: A survey. IEEE Access 2019, 7, 78075–78091. [Google Scholar] [CrossRef]
- El-Regaily, S.A.; Salem MA, M.; Aziz MH, A.; Roushdy, M.I. Lung nodule segmentation and detection in computed tomography. In Proceedings of the 2017 Eighth International Conference on Intelligent Computing and Information Systems (ICICIS), Cairo, Egypt, 5–7 December 2017; pp. 72–78. [Google Scholar]
- Nithila, E.E.; Kumar, S.S. Segmentation of lung nodule in CT data using active contour model and Fuzzy C-mean clustering. Alex. Eng. J. 2016, 55, 2583–2588. [Google Scholar] [CrossRef] [Green Version]
- Mansoor, A.; Bagci, U.; Foster, B.; Xu, Z.; Papadakis, G.Z.; Folio, L.R.; Udupa, J.K.; Mollura, D.J. Segmentation and Image Analysis of Abnormal Lungs at CT: Current Approaches, Challenges, and Future Trends. RadioGraphics 2015, 35, 1056–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Xia, Y.; Cui, H.; Zhang, Y. Pulmonary nodule detection in medical images: A survey. Biomed. Signal Process. Control 2018, 43, 138–147. [Google Scholar] [CrossRef]
- Armato, S.G., 3rd; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; McNitt-Gray, M.F.; Reeves, A.P.; Reeves, A.P.; Aberle, D.R.; Zhao, B.; Henschke, C.I. The lung image database consortium (LIDC) and image database resource initiative (IDRI): A completed reference database of lung nodules on CT scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Setio AA, A.; Traverso, A.; De Bel, T.; Berens, M.S.; Van Den Bogaard, C.; Cerello, P. Validation, comparison, and combination of algorithms for automatic detection of pulmonary nodules in computed tomography images: The LUNA16 challenge. Med. Image Anal. 2017, 42, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Zarogoulidis, K.; Zarogoulidis, P.; Darwiche, K.; Boutsikou, E.; Machairiotis, N.; Tsakiridis, K. Treatment of non-small cell lung cancer (NSCLC). J. Thorac. Dis. 2013, 5, S389. [Google Scholar] [PubMed]
- Van Ginneken, B.; Armato, S.G., III; de Hoop, B.; van Amelsvoort-van de Vorst, S.; Duindam, T.; Niemeijer, M. Comparing and combining algorithms for computer-aided detection of pulmonary nodules in computed tomography scans: The ANODE09 study. Med. Image Anal. 2010, 14, 707–722. [Google Scholar] [CrossRef] [Green Version]
- Riquelme, D.; Akhloufi, M.A. Deep Learning for Lung Cancer Nodules Detection and Classification in CT Scans. AI 2020, 1, 28–67. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Zhou, Z.; Wang, J.; Wang, Y. Joint learning for pulmonary nodule segmentation, attributes and malignancy prediction. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 1109–1113. [Google Scholar]
- Keetha, N.V.; Annavarapu, C.S.R. U-Det: A Modified U-Net architecture with bidirectional feature network for lung nodule segmentation. arXiv 2020, arXiv:2003.09293. [Google Scholar]
- Kumar, S.; Raman, S. Lung Nodule Segmentation Using 3-Dimensional Convolutional Neural Networks[M]//Soft Computing for Problem Solving; Springer: Singapore, 2020; pp. 585–596. [Google Scholar]
- Usman, M.; Lee, B.-D.; Byon, S.-S.; Kim, S.-H.; Lee, B.-I.; Shin, Y.-G. Volumetric lung nodule segmentation using adaptive ROI with multi-view residual learning. Sci. Rep. 2020, 10, 2839. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Sun, W.; Tseng, T.-L.; Li, C.; Qian, W. Fast and fully-automated detection and segmentation of pulmonary nodules in thoracic CT scans using deep convolutional neural networks. Comput. Med. Imaging Graph. 2019, 74, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Aresta, G.; Jacobs, C.; Araújo, T.; Cunha, A.; Ramos, I.; van Ginneken, B.; Campilho, A. iW-Net: An automatic and minimalistic interactive lung nodule segmentation deep network. Sci. Rep. 2019, 9, 1591. [Google Scholar] [CrossRef] [Green Version]
- Tong, G.; Li, Y.; Chen, H.; Zhang, Q.; Jiang, H. Improved U-NET network for pulmonary nodules segmentation. Optik 2018, 174, 460–469. [Google Scholar] [CrossRef]
- Zhao, C.; Han, J.; Jia, Y.; Gou, F. Lung nodule detection via 3D U-Net and contextual convolutional neural network. In Proceedings of the 2018 International Conference on Networking and Network Applications (NaNA), Xi’an, China, 12–15 October 2015; pp. 356–361. [Google Scholar]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2015; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S. Generative adversarial nets. Adv. Neural Inf. Process. Syst. 2014, 27. Available online: https://proceedings.neurips.cc/paper/2014/file/5ca3e9b122f61f8f06494c97b1afccf3-Paper.pdf (accessed on 21 January 2022).
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-net: Fully convolutional neural networks for volumetric medical image segmen-tation. In Proceedings of the 2016 4th International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Pezzano, G.; Ripoll, V.R.; Radeva, P. CoLe-CNN: Context-learning convolutional neural network with adaptive loss func-tion for lung nodule segmentation. Comput. Methods Programs Biomed. 2021, 198, 105792. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhou, M.; Gevaert, O.; Tang, Z.; Dong, D.; Liu, Z.; Jie, T. A multi-view deep convolutional neural networks for lung nodule segmentation. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Glasgow, Scotland, 11–15 July 2017; pp. 1752–1755. [Google Scholar]
- Dong, X.; Xu, S.; Liu, Y.; Wang, A.; Saripan, M.I.; Li, L.; Zhang, X.; Lu, L. Multi-view secondary input collaborative deep learning for lung nodule 3D segmentation. Cancer Imaging 2020, 20, 53. [Google Scholar] [CrossRef] [PubMed]
- Ning, W.; Lei, S.; Yang, J.; Cao, Y.; Jiang, P.; Yang, Q.; Zhang, J.; Wang, X.; Chen, F.; Geng, Z.; et al. Open resource of clinical data from patients with pneumonia for the prediction of COVID-19 outcomes via deep learning. Nat. Biomed. Eng. 2020, 4, 1197–1207. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhou, M.; Liu, Z.; Liu, Z.; Gu, D.; Zang, Y.; Dong, D.; Gevaert, O.; Tian, J. Central focused convolutional neural networks: Developing a data-driven model for lung nodule segmentation. Med. Image Anal. 2017, 40, 172–183. [Google Scholar] [CrossRef]
- Shen, W.; Zhou, M.; Yang, F.; Yu, D.; Dong, D.; Yang, C.; Zang, Y.; Tian, J. Multi-crop Convolutional Neural Networks for lung nodule malignancy suspiciousness classification. Pattern Recognit. 2017, 61, 663–673. [Google Scholar] [CrossRef]
- Zhang, J.; Xia, Y.; Zeng, H.; Zhang, Y. NODULe: Combining constrained multi-scale LoG filters with densely dilated 3D deep convolutional neural network for pulmonary nodule detection. Neurocomputing 2018, 317, 159–167. [Google Scholar] [CrossRef]
- Cao, H.; Liu, H.; Song, E.; Hung, C.-C.; Ma, G.; Xu, X.; Jin, R.; Lu, J. Dual-branch residual network for lung nodule segmentation. Appl. Soft Comput. 2019, 86, 105934. [Google Scholar] [CrossRef]
- Al-Shabi, M.; Lan, B.L.; Chan, W.Y.; Ng, K.H.; Tan, M. Lung nodule classification using deep local–global networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1815–1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, H.; Zhang, C.; Xie, X. Nodulenet: Decoupled false positive reduction for pulmonary nodule detection and segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Cham, Switzerland, 2019; pp. 266–274. [Google Scholar]
- Hesamian, M.H.; Jia, W.; He, X.; Kennedy, P.J. Atrous convolution for binary semantic segmentation of lung nodule. In Proceedings of the ICASSP 2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 1015–1019. [Google Scholar]
- Liu, M.; Dong, J.; Dong, X.; Yu, H.; Qi, L. Segmentation of lung nodule in CT images based on mask R-CNN. In Proceedings of the 2018 9th International Conference on Awareness Science and Technology (iCAST), Fukuoka, Japan, 19–21 September 2018; pp. 1–6. [Google Scholar]
- Khosravan, N.; Bagci, U. Semi-supervised multi-task learning for lung cancer diagnosis. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 710–713. [Google Scholar]
- Wu, P.; Sun, X.; Zhao, Z.; Wang, H.; Pan, S.; Schuller, B. Classification of Lung Nodules Based on Deep Residual Networks and Migration Learning. Comput. Intell. Neurosci. 2020, 2020, 8975078. [Google Scholar] [CrossRef] [PubMed]
- Tran, G.S.; Nghiem, T.P.; Nguyen, V.T.; Luong, C.M.; Burie, J.-C. Improving Accuracy of Lung Nodule Classification Using Deep Learning with Focal Loss. J. Health Eng. 2019, 2019, 5156416. [Google Scholar] [CrossRef]
- Li, W.; Cao, P.; Zhao, D.; Wang, J. Pulmonary Nodule Classification with Deep Convolutional Neural Networks on Computed Tomography Images. Comput. Math. Methods Med. 2016, 2016, 6215085. [Google Scholar] [CrossRef]
- Mastouri, R.; Khlifa, N.; Neji, H.; Hantous-Zannad, S. A bilinear convolutional neural network for lung nodules classification on CT images. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 91–101. [Google Scholar] [CrossRef]
- Bhavanishankar, K.; Sudhamani, M.V. Classification of Lung Nodules into Benign or Malignant and Development of a CBIRSystem for Lung CT Scans. In Proceedings of the International Conference on Computational Vision and Bio Inspired Computing, Coimbatore, India, 25–26 September 2019; Springer: Cham, Switzerland, 2019; pp. 563–575. [Google Scholar]
- Ali, I.; Muzammil, M.; Haq, I.U.; Khaliq, A.A.; Abdullah, S. Efficient lung nodule classification using transferable texture convolutional neural network. IEEE Access 2020, 8, 175859–175870. [Google Scholar] [CrossRef]
- Al-Shabi, M.; Lee, H.K.; Tan, M. Gated-Dilated Networks for Lung Nodule Classification in CT Scans. IEEE Access 2019, 7, 178827–178838. [Google Scholar] [CrossRef]
- Dey, R.; Lu, Z.; Hong, Y. Diagnostic classification of lung nodules using 3D neural networks. In Proceedings of the 2018 IEEE 15th interna-tional symposium on biomedical imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 774–778. [Google Scholar]
- Nibali, A.; He, Z.; Wollersheim, D. Pulmonary nodule classification with deep residual networks. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Kang, G. Multiview convolutional neural networks for lung nodule classification. Int. J. Imaging Syst. Technol. 2017, 27, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Kumar, D.; Wong, A.; Clausi, D.A. Lung nodule classification using deep features in CT images. In Proceedings of the 2015 12th Conference on Computer and Robot Vision, Halifax, NS, Canada, 3–5 June 2015; pp. 133–138. [Google Scholar]
- Jia, T.; Zhang, H.; Bai, Y.K. Benign and Malignant Lung Nodule Classification Based on Deep Learning Feature. J. Med. Imaging Health Inform. 2015, 5, 1936–1940. [Google Scholar] [CrossRef]
- Sang, J.; Alam, M.S.; Xiang, H. Automated detection and classification for early stage lung cancer on CT images using deep learning. In Proceedings of the Pattern Recognition and Tracking XXX. International Society for Optics and Photonics, Baltimore, MA, USA, 15–16 April 2019; p. 109950S. [Google Scholar]
- Wang, W.; Li, X.; Yang, J.; Lu, T. Mixed link networks. arXiv 2018, arXiv:1802.01808. [Google Scholar]
- Agnes, S.A.; Anitha, J. Automatic 2D Lung Nodule Patch Classification using Deep Neural Networks. In Proceedings of the 2020 Fourth International Conference on Inventive Systems and Control (ICISC), Coimbatore, India, 8–10 January 2020. [Google Scholar]
- Shen, S.; Han, S.X.; Aberle, D.R.; Bui, A.A.; Hsu, W. An interpretable deep hierarchical semantic convolutional neural network for lung nodule malignancy classification. Expert Syst. Appl. 2019, 128, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Lin, L.; Wang, J. Lung Nodule Classification in CT Images Using 3D DenseNet. IOP Publishing 2021, 1827, 012155. [Google Scholar] [CrossRef]
- Zhang, G.; Yang, Z.; Gong, L.; Jiang, S.; Wang, L.; Zhang, H. Classification of lung nodules based on CT images using squeeze-and-excitation net-work and aggregated residual transformations. La Radiol. Med. 2020, 125, 374–383. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Hu, T.; Wang, J.; Lyu, J.; Banerjee, S.; Ling, S.H. Lung Nodule Classification using A Novel Two-stage Convolutional Neural Networks Structure. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6259–6262. [Google Scholar]
- Zhang, L.; Qiang, Y.; Zhang, X.; Wang, X. Classification of multi-scale lung nodules based on synchronized deep supervision. Comput. Appl. Softw. 2019, 36, 214–219. [Google Scholar] [CrossRef]
- Liu, H.; Cao, H.; Song, E.; Ma, G.; Xu, X.; Jin, R.; Liu, C.; Hung, C.-C. Multi-model Ensemble Learning Architecture Based on 3D CNN for Lung Nodule Malignancy Suspiciousness Classification. J. Digit. Imaging 2020, 33, 1242–1256. [Google Scholar] [CrossRef]
- Xia, K.; Chi, J.; Gao, Y.; Jiang, Y.; Wu, C. Adaptive Aggregated Attention Network for Pulmonary Nodule Classification. Appl. Sci. 2021, 11, 610. [Google Scholar] [CrossRef]
- Yang, Y.; Feng, X.; Chi, W.; Li, Z.; Duan, W.; Liu, H. Deep learning aided decision support for pulmonary nodules diagnosing: A review. J. Thorac. Dis. 2018, 10, S867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherstinsky, A. Fundamentals of Recurrent Neural Network (RNN) and Long Short-Term Memory (LSTM) Network. Phys. D Nonlinear Phenom. 2020, 404, 132306. [Google Scholar] [CrossRef] [Green Version]
- Hinton, G.E.; Osindero, S.; Teh, Y.W. A fast learning algorithm for deep belief nets. Neural Comput. 2006, 18, 1527–1554. [Google Scholar] [CrossRef]
- Baldi, P. Autoencoders, unsupervised learning, and deep architectures. In Proceedings of the ICML Workshop on Unsupervised and Transfer Learning, Bellevue, DC, USA, 27 June 2012; pp. 37–49. [Google Scholar]
- Navamani, T.M. Efficient deep learning approaches for health informatics. In Deep Learning and Parallel Computing Environment for Bioengineering Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 123–137. [Google Scholar]
- Liang, J.; Ye, G.; Guo, J.; Zhang, S.; Huang, Q. Reducing False-Positives in Lung Nodules Detection Using Balanced Datasets. Front. Public Health 2021, 9, 517. [Google Scholar] [CrossRef]
- Gaga, M.; Loverdos, K.; Fotiadis, A.; Kontogianni, C.; Iliopoulou, M. Lung nodules: A comprehensive review on current approach and management. Ann. Thorac. Med. 2019, 14, 226–238. [Google Scholar] [CrossRef]


| Dataset | The Number of CT Scans | The Number of Nodules | Annotation |
|---|---|---|---|
| LIDC-IDRI | 1018 | 36,378 | √ |
| LUNA16 | 888 | 13,799 | √ |
| Ali Tianchi | 1000 | 1000 | √ |
| NSCLC | 211 | - | √ |
| ELCAP | 50 | - | √ |
| ANODE09 | 55 (only 5 CT scans) | 39 | √ |
| Metric | Brief | Expression |
|---|---|---|
| Sensitivity (SEN) | Measures the proportion of positives that are correctly identified | |
| Accuracy (ACC) | Classification accuracy of the classifier | |
| Positive predictive value (PPV) | The proportions of positive results in statistics and diagnostic tests that are truly positive | |
| Dice Similarity Coefficient (DSC) | A statistics used to gauge the similarity of two samples. | |
| Intersection over Union (IoU) | The IoU measurement gives the similarity between the predicted area and the real area of the objects present in the set of images | |
| F1-Score | Used in statistics to measure the accuracy of a binary classification model | |
| Receiver Operating Characteristic (ROC) | A curve depicting the relationship between the sensitivity and specificity (Y-axis is TP rate and X-axis is the FP rate) | - |
| Free Receiver Operating Characteristic (FROC) | Similar to the ROC curve, differing only in the X-axis. The X-axis is the FP rate per image (or per scan) | - |
| Area Under Curve (AUC) | Total area under the ROC curve | - |
| Competition Performance Metric (CPM) | Average of the Sensitivity at seven defined FP rates in the FROC curve: 1/8,1/4,1/2,1,2,4,8 FPs/scan | - |
| Mean Average Precision (mAP) | Mean Average Precision | - |
| Year | Author | Dataset | PPV (%) | SEN (%) | DSC (%) | IOU | Architecture | Approach |
|---|---|---|---|---|---|---|---|---|
| 2020 | Dong et al. [67] | LIDC-IDRI | 93.6 | 98.10 | 92.6 | - | Multiview | |
| 2020 | Cao et al. [72] | LIDC-IDRI | 79.64 | 89.35 | 82.74 | - | Multiview | |
| 2017 | Wang et al. [66] | LIDC-IDRI | 77.59 | 83.72 | 77.67 | - | Multiview | |
| 2017 | Wang et al. [69] | LIDC-IDRI/GDGH | 75.84 | 92.75 | 82.15 | - | Multiview | |
| 2017 | Shen et al. [70] | Random datasets | 87.14 | 0.77 | - | - | MC-CNN | Multiview |
| 2021 | Pezzano et al. [65] | LIDC-IDRI | - | - | - | 76.6 | Nodule type | General |
| 2020 | Keetha et al. [54] | LUNA16 | 78.92 | 92.24 | 82.82 | - | U-Net et al. | General |
| 2020 | Kumar et al. [55] | LUNA16 | - | - | 96.15 | - | U-Net et al. | General |
| 2020 | Usman et al. [56] | LIDC-IDRI | 88.24 | 91.62 | 87.55 | - | General | |
| 2019 | Huang et al. [57] | LUNA16 | - | - | 79.3 | - | U-Net et al. | General |
| 2018 | Wu et al. [53] | LIDC-IDRI | - | - | 73.98 | - | U-Net et al. | General |
| 2018 | Tong et al. [59] | LUNA16 | - | - | 73.6 | - | U-Net et al. | General |
| 2018 | Zhao et al. [60] | LIDC-IDRI | - | - | - | - | U-Net et al. | General |
| 2018 | Liu et al. [76] | LIDC-IDRI | - | - | - | - | FCN | General |
| 2019 | Aresta et al. [58] | LIDC-IDRI | - | - | - | 55 | Nodule type | |
| 2019 | Hesamian et al. [75] | LIDC-IDRI | - | - | 81.24 | - | - | |
| 2018 | Khosravan et al. [77] | LUNA16 | - | 98 | 91 | - | semi-supervised | |
| 2019 | Tang et al. [74] | LIDC-IDRI | - | - | 83.10 | - | - |
| Year | Reference | Dataset | SEN (%) | AUC (%) | ACC | Classification |
|---|---|---|---|---|---|---|
| 2021 | Ge Zhang [94] | LUNA16 | 87.00 | - | 92.40 | MOB |
| 2020 | Akila Agnes [92] | LIDC- IDRI | 81.00 | 94.40 | - | MOB |
| 2020 | Hong Liu [98] | LIDC-IDRI | 0.837 | 93.90 | 90.60 | MOB |
| 2020 | Kai Xia [99] | LIDC-IDRI | 91.30 | - | 91.90 | MOB |
| 2020 | Ali et al. [83] | LIDC-IDRI | 98.10 | 99.11 | 96.69 | MOB |
| 2019 | Zhang Li [97] | LIDC-IDRI | 95.17 | - | 93.68 | MOB |
| 2019 | Guobin Zhang [95] | LUNA16 | - | 95.63 | 91.67 | MOB |
| 2019 | Al-Shabi et al. [73] | LIDC-IDRI | 88.66 | 95.62 | 88.46 | MOB |
| 2019 | Al-Shabi et al. [84] | LIDC-IDRI | 92.21 | 93.15 | 92.57 | MOB |
| 2018 | Shiwen Shen [93] | LIDC-IDRI | 0.705 | 0.856 | 0.842 | MOB |
| 2018 | Dey et al. [85] | LIDC-IDRI/Themselves dataset | - | 95.48 | 90.40 | MOB |
| 2017 | Nibali et al. [86] | LIDC-IDRI | 91.07 | 94.59 | 89.90 | MOB |
| 2016 | Shen et al. [70] | LIDC-IDRI | 77.00 | 93.00 | 87.14 | MOB |
| 2015 | Kumar et al. [88] | LIDC-IDRI | 83.35 | - | 75.01 | MOB |
| 2020 | Wu et al. [78] | LIDC-IDRI | 97.70 | - | 98.23 | NON |
| 2019 | Yang An [96] | LIDC-IDRI | - | - | 89.60 | NON |
| 2019 | Tran et al. [79] | LIDC-IDRI | 96.00 | - | 97.20 | NON |
| 2020 | Rekka Mastouri [81] | LUNA16 | 91.85 | - | 91.99 | NON |
| 2018 | Wu et al. [53] | LIDC-IDRI | - | - | 97.58 | NON |
| 2018 | Zhao et al. [60] | LIDC-IDRI | - | - | - | NON |
| 2017 | Liu et al. [87] | LIDC-IDRI | 90.18 | 98.10 | - | others |
| 2016 | Li et al. [80] | LIDC-IDRI | 89.0 | - | 86.40 | others |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, R.; Xiao, C.; Huang, Y.; Hassan, H.; Huang, B. Deep Learning Applications in Computed Tomography Images for Pulmonary Nodule Detection and Diagnosis: A Review. Diagnostics 2022, 12, 298. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020298
Li R, Xiao C, Huang Y, Hassan H, Huang B. Deep Learning Applications in Computed Tomography Images for Pulmonary Nodule Detection and Diagnosis: A Review. Diagnostics. 2022; 12(2):298. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020298
Chicago/Turabian StyleLi, Rui, Chuda Xiao, Yongzhi Huang, Haseeb Hassan, and Bingding Huang. 2022. "Deep Learning Applications in Computed Tomography Images for Pulmonary Nodule Detection and Diagnosis: A Review" Diagnostics 12, no. 2: 298. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020298