
Detection of Splenic Tissue Using 99mTc-Labelled Denatured Red Blood Cells Scintigraphy—A Quantitative Single Center Analysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Radiopharmaceutical and Imaging Protocol
2.3. Data Analysis
2.4. Data Statistics
3. Results
3.1. Patient Characteristics
3.2. Uptake Quantification
3.2.1. Sites of Physiologic Uptake
3.2.2. Suspected Splenic Lesions
3.3. Evaluation of a Potential Quantitative Cutoff for Clinical Reading
3.3.1. Definition of a Quantitative Cutoff in Relation to Physiologic Uptake in a Subgroup of Unequivocal Cases
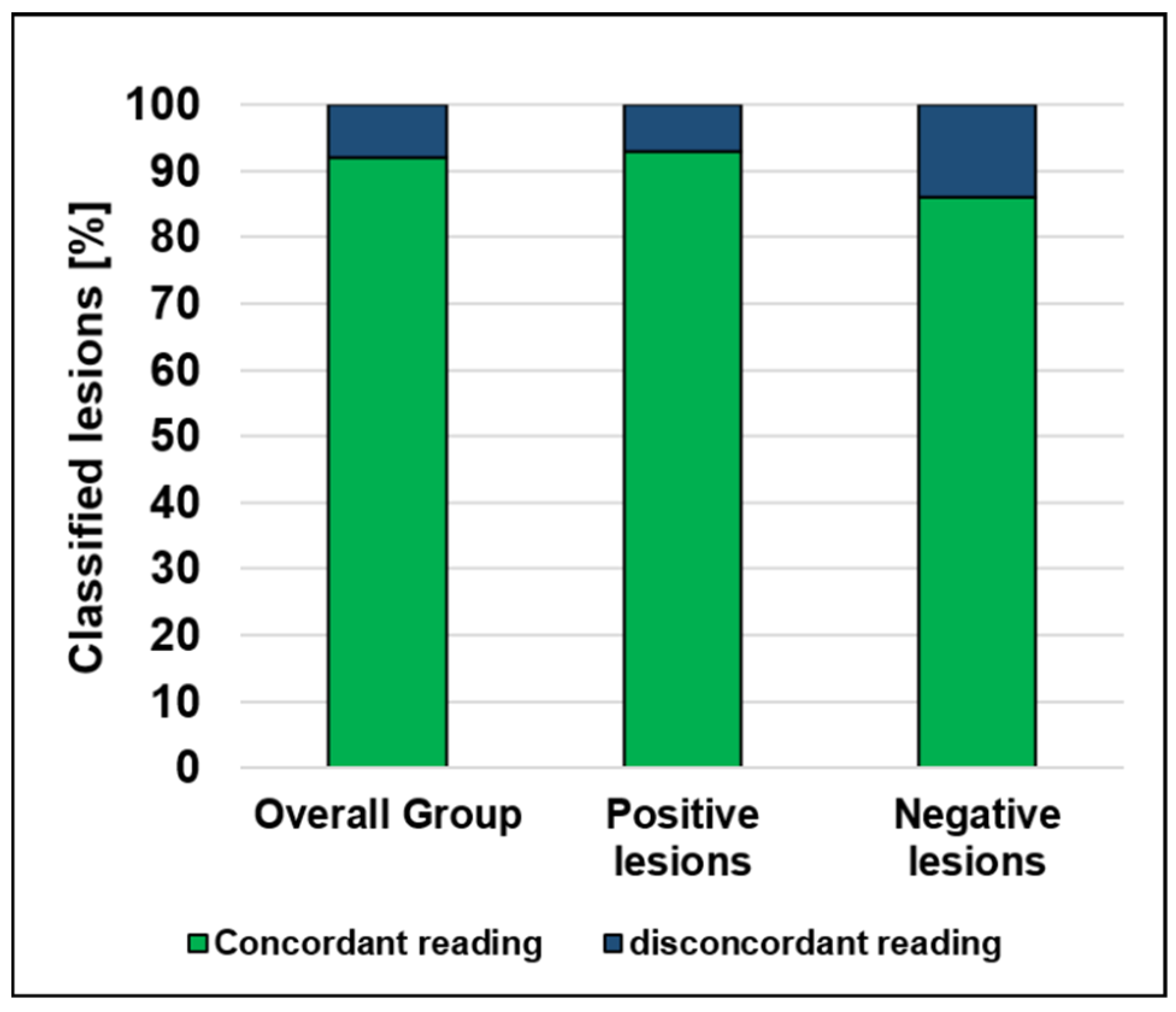
3.3.2. Proof-of-Principle Quantitative Reading in All Cases in Direct Comparison to Standard Qualitative Clinical Reading
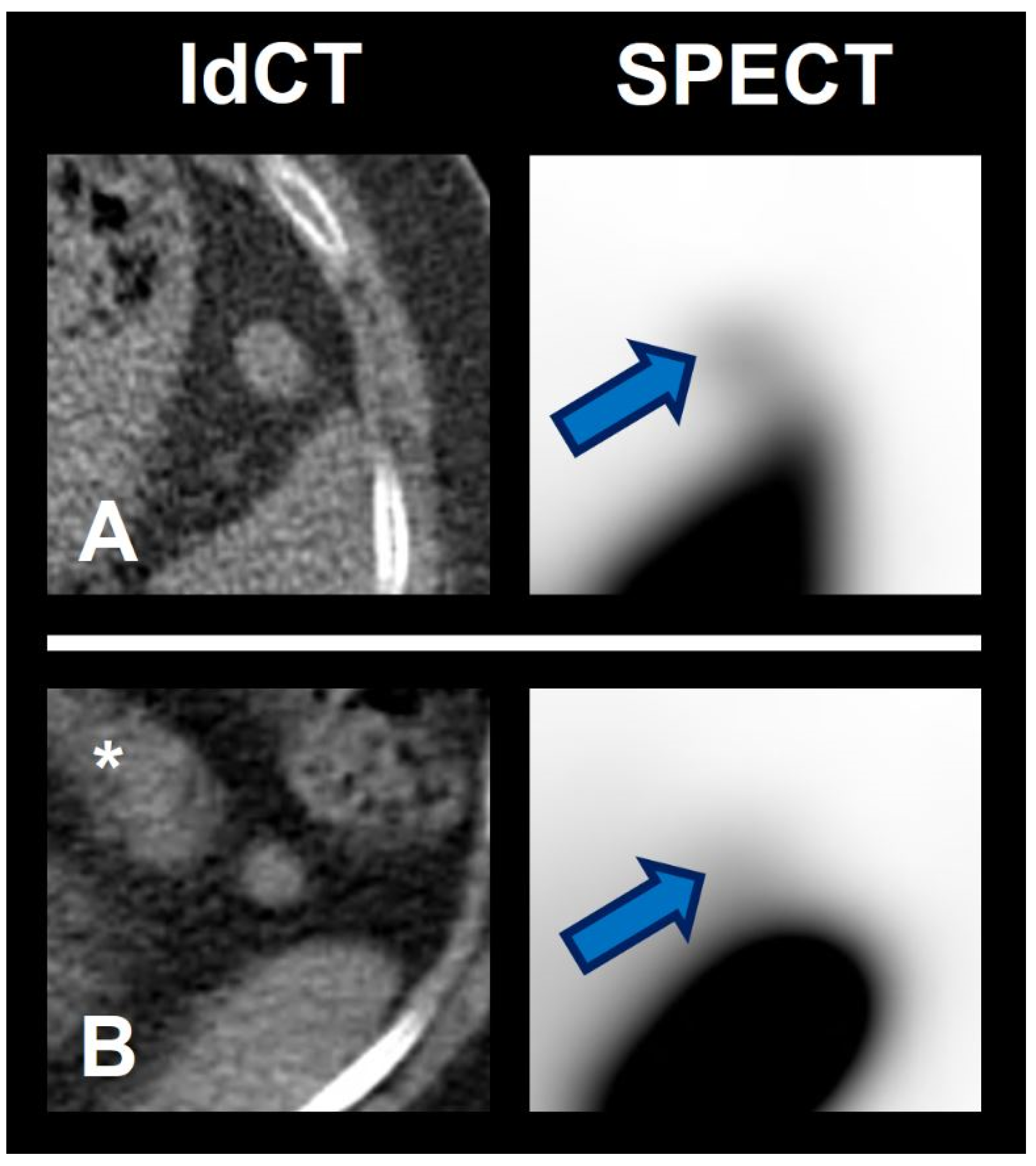
3.3.3. Exemplary Use of the Quantitative Cutoff in Histology-Proven Cases
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Graziani, T.; Baldari, G.; Sammartano, A.; Scarlattei, M.; Migliari, S.; Pescarenico, G.M.; Cidda, C.; Bola, S.; Ruffini, L. SPECT/CT with 99mTc labelled heat-denatured erythrocyte to detect thoracic and abdominal splenic tissue. Acta Bio Med. Atenei Parm. 2020, 91, e2020098. [Google Scholar]
- Ekmekçi, Ş.; Diz-Küçükkaya, R.; Türkmen, C.; Adalet, I. Selective spleen scintigraphy in the evaluation of accessory spleen/splenosis in splenectomized/nonsplenectomized patients and the contribution of SPECT imaging. Mol. Imaging Radionucl. Ther. 2015, 24, 1–7. [Google Scholar] [CrossRef]
- Pelletier-Galarneau, M.; Ozimok, C.; Bazarjani, S.; Zuckier, L. Selective spleen scintigraphy using 99mTc-heat denatured red blood cells in the era of fusion SPECT-CT imaging. J. Nucl. Med. 2014, 55, 1994. [Google Scholar]
- Royal, H.D.; Brown, M.L.; Drum, D.; Nagle, C.; Sylvester, J.; Ziessman, H. Society of Nuclear Medicine procedure guideline for hepatic and splenic imaging 3.0. Soc. Nucl. Med. Proced. Guidel. Man. 2003, 53–57. [Google Scholar]
- Hagan, I.; Hopkins, R.; Lyburn, I. Superior demonstration of splenosis by heat-denatured Tc-99m red blood cell scintigraphy compared with Tc-99m sulfur colloid scintigraphy. Clin. Nucl. Med. 2006, 31, 463–466. [Google Scholar] [CrossRef]
- Massey, M.D.; Stevens, J.S. Residual spleen found on denatured red blood cell scan following negative colloid scans. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1991, 32, 2286–2287. [Google Scholar]
- Ziessman, H.A. Hepatobiliary scintigraphy in 2014. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 967–975. [Google Scholar] [CrossRef] [Green Version]
- De Roo, M. Scintigraphy of the Spleen. In Medical Imaging of the Spleen; De Schepper, A.M., Vanhoenacker, F., Eds.; Springer: Berlin, Germany, 2000; p. 155. ISBN 3-540-65535-2. [Google Scholar]
- Gunes, I.; Yilmazlar, T.; Sarikaya, I.; Akbunar, T.; Irgil, C. Scintigraphic detection of splenosis: Superiority of tomographic selective spleen scintigraphy. Clin. Radiol. 1994, 49, 115–117. [Google Scholar] [CrossRef]
- Yammine, J.N.; Yatim, A.; Barbari, A. Radionuclide imaging in thoracic splenosis and a review of the literature. Clin. Nucl. Med. 2003, 28, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-C.; Lee, R.-C.; Chiang, J.-H.; Wei, C.-J.; Chu, L.-S.; Liu, R.-S.; Chang, C.-Y. MR features of abdominal splenosis. Am. J. Roentgenol. 2003, 180, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Koç, Z.P.; Kara, P.Ö.; Tombak, A. Splenosis mimicking lymphoma relapse confirmed by 18F-FDG PET/CT and Tc-99m nano-colloid scintigraphy thirty years after splenectomy for trauma. Mol. Imaging Radionucl. Ther. 2019, 28, 38. [Google Scholar] [CrossRef] [PubMed]
- Vergara, D.; Ginolfi, F.; Moscati, S.; Giordano, B.; Ferrara, N.; Panico, C.; Imbriaco, M. Multiple intra-hepatic and abdominal splenosis: An easy call if you know about it. Acta Radiol. Open 2018, 7, 2058460118772324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandon, Y.K.; Coppa, C.P.; Purysko, A.S. Splenosis: A great mimicker of neoplastic disease. Abdom. Radiol. 2018, 43, 3054–3059. [Google Scholar] [CrossRef] [PubMed]
- Vernuccio, F.; Dimarco, M.; Porrello, G.; Cannella, R.; Cusmà, S.; Midiri, M.; Brancatelli, G. Abdominal splenosis and its differential diagnoses: What the radiologist needs to know. Curr. Probl. Diagn. Radiol. 2020, 50, 229–235. [Google Scholar] [CrossRef]
- Demirci, E.; Kabasakal, L.; Mülazimoğlu, M. Abdominal Splenosis Mimicking Peritoneal Metastasis in Prostate-Specific Membrane Antigen PET/CT, Confirmed With Selective Spleen SPECT/CT. Clin. Nucl. Med. 2017, 42, e504–e505. [Google Scholar] [CrossRef]
- Coccolini, F.; Gheza, F.; Lotti, M.; Virzì, S.; Iusco, D.; Ghermandi, C.; Melotti, R.; Baiocchi, G.; Giulini, S.M.; Ansaloni, L. Peritoneal carcinomatosis. World J. Gastroenterol. WJG 2013, 19, 6979. [Google Scholar] [CrossRef]
- Lauer, U.M.; Schell, M.; Beil, J.; Berchtold, S.; Koppenhöfer, U.; Glatzle, J.; Königsrainer, A.; Möhle, R.; Nann, D.; Fend, F. Phase I study of oncolytic vaccinia virus GL-ONC1 in patients with peritoneal carcinomatosis. Clin. Cancer Res. 2018, 24, 4388–4398. [Google Scholar] [CrossRef] [Green Version]
- Nakamoto, R.; Zaba, L.C.; Liang, T.; Reddy, S.A.; Davidzon, G.; Aparici, C.M.; Nguyen, J.; Moradi, F.; Iagaru, A.; Franc, B.L. Prognostic value of bone marrow metabolism on pretreatment 18F-FDG PET/CT in patients with metastatic melanoma treated with anti-PD-1 therapy. J. Nucl. Med. 2021, 62, 1380–1383. [Google Scholar] [CrossRef]
- Chiaravalloti, A.; Danieli, R.; Abbatiello, P.; Di Pietro, B.; Travascio, L.; Cantonetti, M.; Guazzaroni, M.; Orlacchio, A.; Simonetti, G.; Schillaci, O. Factors affecting intrapatient liver and mediastinal blood pool 18F-FDG standardized uptake value changes during ABVD chemotherapy in Hodgkin’s lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1123–1132. [Google Scholar] [CrossRef]
- Ananthan, K.; Yusuf, G.T.; Kumar, M. Intrahepatic and intra-abdominal splenosis: A case report and review of literature. World J. Hepatol. 2019, 11, 773. [Google Scholar] [CrossRef]
- Wu, C.; Zhang, B.; Chen, L.; Zhang, B.; Chen, X. Solitary perihepatic splenosis mimicking liver lesion: A case report and literature review. Medicine 2015, 94, e586. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pat. ID | Sex | Age [y] | Splen-Ectomy | Pancrea-Tectomy | Uptake in Sites of Physiologic Uptake | Number of Lesions as Rated in Scintigraphy | Newly Discovered Lesions 1 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Bone Marrow | Pancreas | Regular Spleen | Pos. | Neg. | ||||||
| 1 | m | 44 | partially | no | 0.45 | 0.25 | n/a | 9 | 0 | 0 |
| 2 | f | 67 | no | no | 0.27 | 0.27 | 23.18 | 1 * | 1 | 2 |
| 3 | m | 68 | yes | no | 0.03 | 0.03 | n/a | 1 | 2 | 1 |
| 4 | m | 51 | yes | no | 0.22 | 0.18 | n/a | 1 | 1 | 0 |
| 5 | f | 67 | no | no | 0.09 | 0.09 | 14.45 | 0 | 0 | 0 |
| 6 | f | 84 | yes | distal | 0.22 | n/a | n/a | 4 | 0 | 0 |
| 7 | m | 67 | yes | distal | 0.12 | n/a | n/a | 1 | 0 | 0 |
| 8 | m | 35 | no | no | 0.16 | 0.05 | 3.91 | 1 | 0 | 0 |
| 9 | f | 60 | no | no | 0.25 | 0.53 | 19.95 | 1 | 0 | 0 |
| 10 | m | 62 | yes | no | 0.17 | 0.15 | n/a | 3 | 0 | 0 |
| 11 | m | 62 | yes | no | 0.15 | 0.03 | n/a | 1 | 0 | 0 |
| 12 | w | 73 | no | no | 0.08 | 0.06 | 3.70 | 1 | 0 | 0 |
| 13 | f | 60 | no | no | 0.15 | 0.67 | 29.82 | 1 | 0 | 0 |
| 14 | f | 59 | yes | distal | 0.17 | n/a | n/a | 1 | 0 | 0 |
| 15 | f | 39 | partially | no | 0.20 | 0.06 | n/a | 8 | 0 | 0 |
| 16 | f | 56 | no | no | 0.07 | 0.19 | 16.59 | 0 | 1 | 1 |
| 17 | m | 64 | no | PPPD | 0.19 | n/a | 3.86 | 1 | 1 | 1 |
| 18 | f | 28 | no | no | 0.12 | n/a ** | 0.61 | 0 | 1 | 0 |
| 19 | m | 50 | yes | no | 0.19 | 0.04 | n/a | 12 | 0 | 0 |
| 20 | m | 51 | No | distal | 0.22 | 0.07 | 3.04 | 0 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzgreve, A.; Völter, F.; Delker, A.; Kunz, W.G.; Fabritius, M.P.; Brendel, M.; Albert, N.L.; Bartenstein, P.; Unterrainer, M.; Unterrainer, L.M. Detection of Splenic Tissue Using 99mTc-Labelled Denatured Red Blood Cells Scintigraphy—A Quantitative Single Center Analysis. Diagnostics 2022, 12, 486. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020486
Holzgreve A, Völter F, Delker A, Kunz WG, Fabritius MP, Brendel M, Albert NL, Bartenstein P, Unterrainer M, Unterrainer LM. Detection of Splenic Tissue Using 99mTc-Labelled Denatured Red Blood Cells Scintigraphy—A Quantitative Single Center Analysis. Diagnostics. 2022; 12(2):486. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020486
Chicago/Turabian StyleHolzgreve, Adrien, Friederike Völter, Astrid Delker, Wolfgang G. Kunz, Matthias P. Fabritius, Matthias Brendel, Nathalie L. Albert, Peter Bartenstein, Marcus Unterrainer, and Lena M. Unterrainer. 2022. "Detection of Splenic Tissue Using 99mTc-Labelled Denatured Red Blood Cells Scintigraphy—A Quantitative Single Center Analysis" Diagnostics 12, no. 2: 486. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12020486