
Urinalysis, but Not Blood Biochemistry, Detects the Early Renal Impairment in Patients with COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
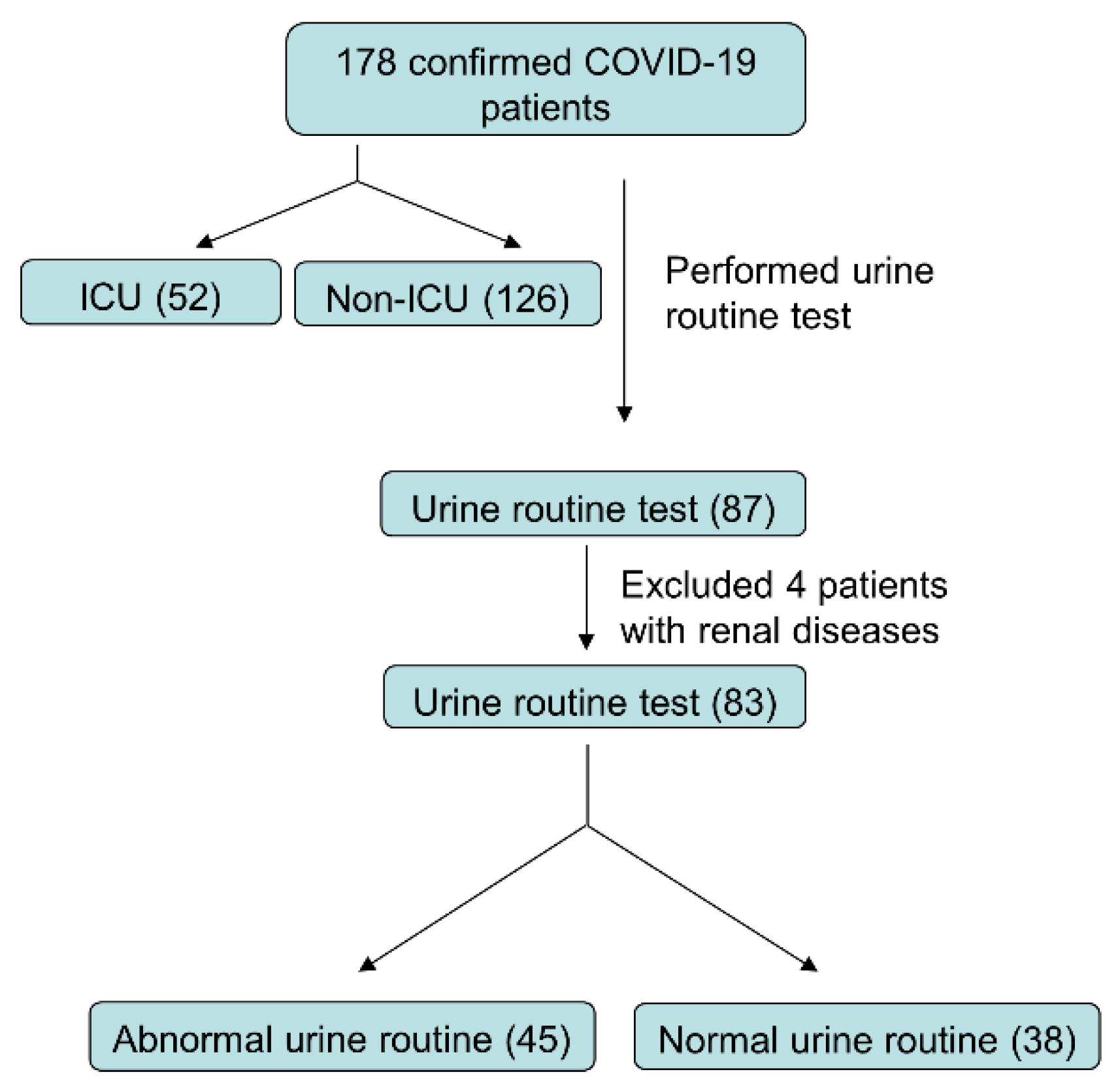
3.1. Presenting Characteristics
3.2. No COVID-19 Patients Diagnosed with AKI
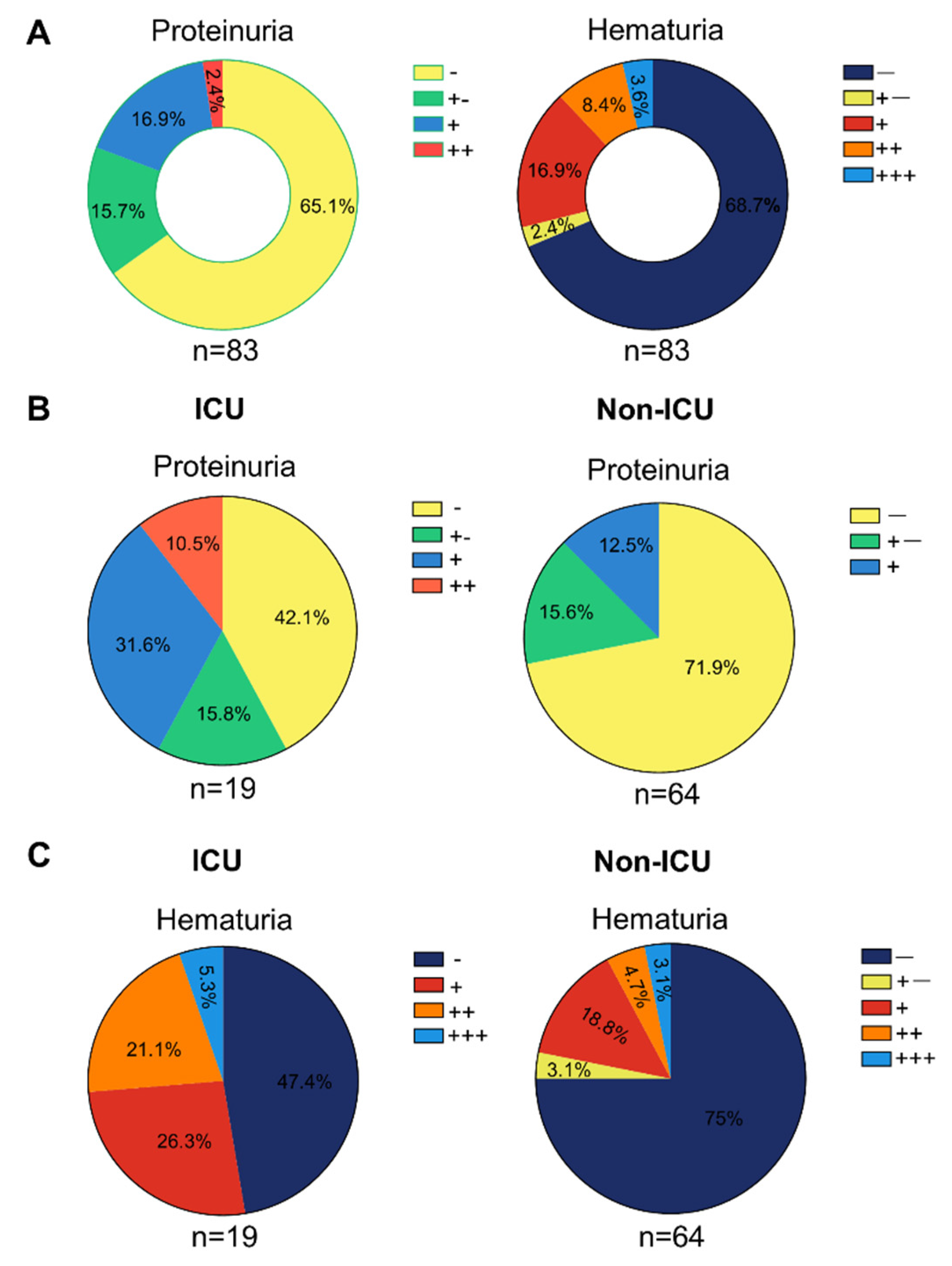
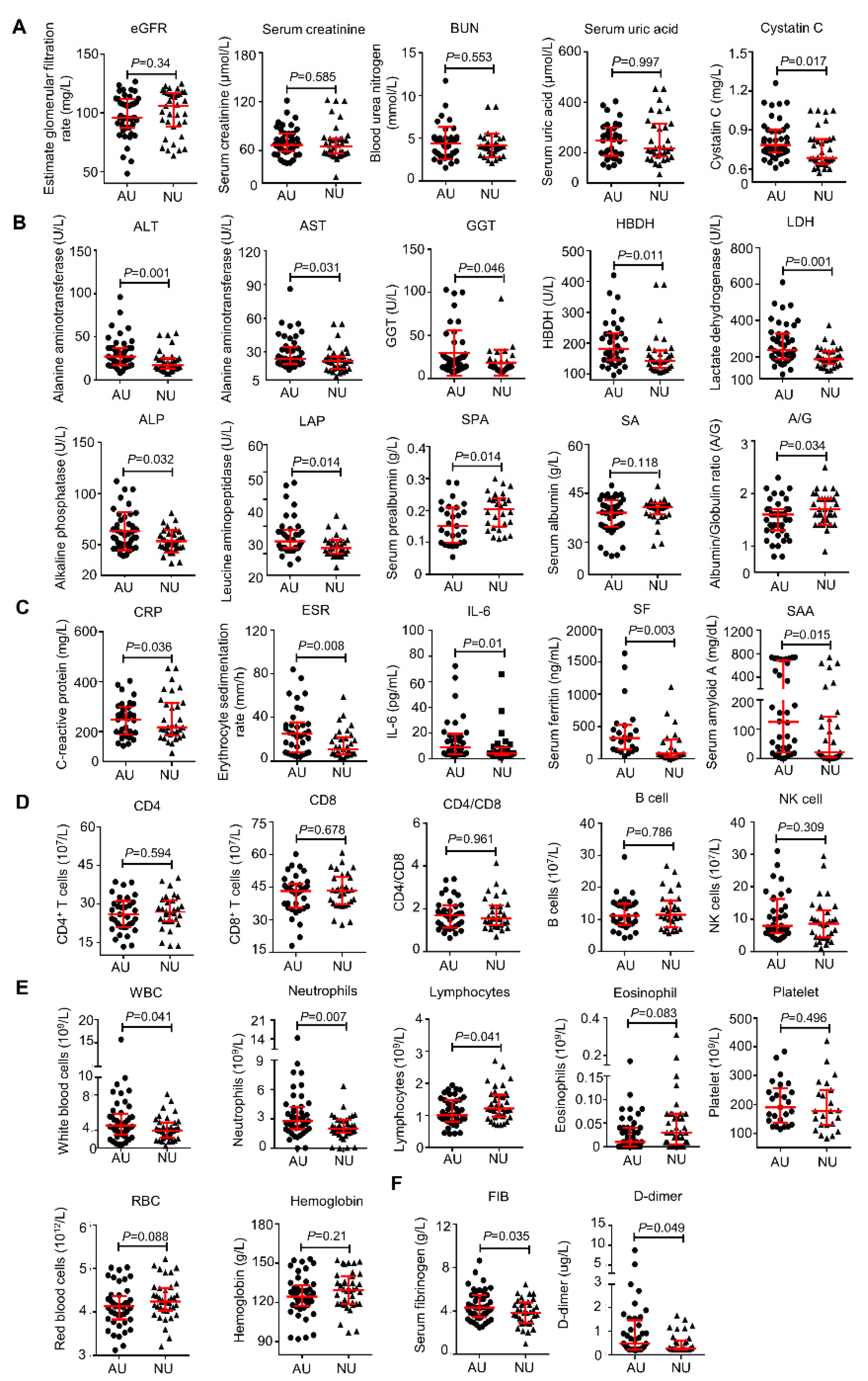
3.3. Potential Kidney Impairment Reflected by the Routine Urine Test
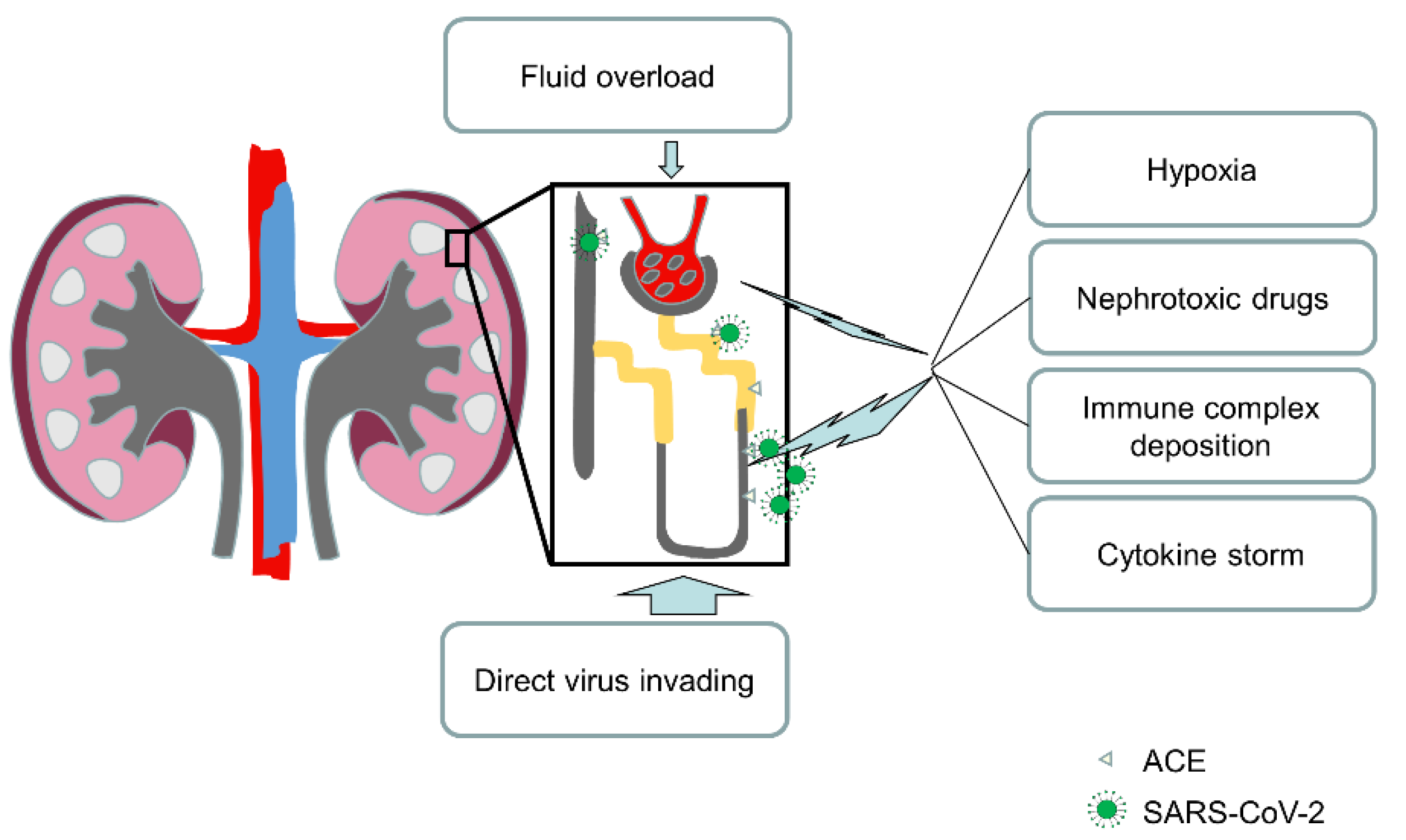
3.4. Kidney Impairment Was Caused by a Direct Virus Invading
3.5. Urinalysis Abnormality Correlates with the Severity of COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280e8. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, M.; Ferguson, I.D.; Miao, W.; Khavari, P.A. SARS-CoV-2 B.1.1.7 and B.1.351 Spike Variants Bind Human ACE2 with Increased Affinity. Lancet Infect. Dis. 2021, 21, 1070. [Google Scholar] [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-Converting Enzyme 2 (ACE2) as a SARS-CoV-2 Receptor: Molecular Mechanisms and Potential Therapeutic Target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary Manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes Is a Risk Factor for the Progression and Prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y.; Yuan, Y.-D.; Yang, Y.-B.; Yan, Y.-Q.; Akdis, C.A.; Gao, Y.-D. Clinical Characteristics of 140 Patients Infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B. Global Pandemics Interconnected—Obesity, Impaired Metabolic Health and COVID-19. Nat. Rev. Endocrinol. 2021, 17, 135–149. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.; Sartori, A.; Vitiello, A.; Piatto, G.; Noaro, G.; Olmi, S.; Foschi, D.; De Re, L.; Zappa, M.; Sarro, G.; et al. Complications and Mortality in a Cohort of Patients Undergoing Emergency and Elective Surgery with Perioperative SARS-CoV-2 Infection: An Italian Multicenter Study. Teachings of Phase 1 to Be Brought in Phase 2 Pandemic. Updates Surg. 2021, 73, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Capstick, T.; Ahmed, R.; Kow, C.S.; Mazhar, F.; Merchant, H.A.; Zaidi, S.T.R. Mortality in COVID-19 Patients with Acute Respiratory Distress Syndrome and Corticosteroids Use: A Systematic Review and Meta-Analysis. Expert Rev. Respir. Med. 2020, 14, 1149–1163. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-Associated Acute Respiratory Distress Syndrome: A Multicentre Prospective Observational Study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- Camporota, L.; Chiumello, D.; Busana, M.; Gattinoni, L.; Marini, J.J. Pathophysiology of COVID-19-Associated Acute Respiratory Distress Syndrome. Lancet Respir. Med. 2021, 9, e1. [Google Scholar] [CrossRef]
- Gusev, E.; Sarapultsev, A.; Hu, D.; Chereshnev, V. Problems of Pathogenesis and Pathogenetic Therapy of COVID-19 from the Perspective of the General Theory of Pathological Systems (General Pathological Processes). Int. J. Mol. Sci. 2021, 22, 7582. [Google Scholar] [CrossRef] [PubMed]
- Zotova, N.V.; Chereshnev, V.A.; Gusev, E.Y. Systemic Inflammation: Methodological Approaches to Identification of the Common Pathological Process. PLoS ONE 2016, 11, e0155138. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney Disease Is Associated with In-Hospital Death of Patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, X.; Chen, H.; Yan, S.; Li, D.; Li, Y.; Gong, Z. Coronavirus Disease 19 Infection Does Not Result in Acute Kidney Injury: An Analysis of 116 Hospitalized Patients from Wuhan, China. Am. J. Nephrol. 2020, 51, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.S.; James, B.D.; Al-Chalabi, S.; Sykes, L.; Kalra, P.A.; Green, D. Community- versus Hospital-Acquired Acute Kidney Injury in Hospitalised COVID-19 Patients. BMC Nephrol. 2021, 22, 269. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wu, M.; Yao, J.; Guo, J.; Liao, X.; Song, S.; Li, J.; Duan, G.; Zhou, Y.; Wu, X.; et al. Caution on Kidney Dysfunctions of COVID-19 Patients. MedRxiv 2020, preprint. [Google Scholar] [CrossRef]
- Silver, S.A.; Beaubien-Souligny, W.; Shah, P.S.; Harel, S.; Blum, D.; Kishibe, T.; Meraz-Munoz, A.; Wald, R.; Harel, Z. The Prevalence of Acute Kidney Injury in Patients Hospitalized With COVID-19 Infection: A Systematic Review and Meta-Analysis. Kidney Med. 2021, 3, 83–98.e1. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.; Mahajan, Z.A.; Vasistha, P.; Chakraborty, R.; Mukunda, K.; Tibrewal, A.; Neyra, J.A. Incidence and Outcomes of Acute Kidney Injury in COVID-19: A Systematic Review. Blood Purif. 2021, 51, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Fu, E.L.; Janse, R.J.; de Jong, Y.; van der Endt, V.H.W.; Milders, J.; van der Willik, E.M.; de Rooij, E.N.M.; Dekkers, O.M.; Rotmans, J.I.; van Diepen, M. Acute Kidney Injury and Kidney Replacement Therapy in COVID-19: A Systematic Review and Meta-Analysis. Clin. Kidney J. 2020, 13, 550–563. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Zhou, H.; Li, M.; Zhang, Z.; Guo, W.; Yu, T.; Gui, Y.; Wang, Q.; Zhao, L.; Luo, S.; et al. A novel simple scoring model for predicting severity of patients with SARS-CoV-2 infection. Transbound. Emerg. Dis. 2020, 67, 2823–2829. [Google Scholar] [CrossRef] [PubMed]
- Morell-Garcia, D.; Ramos-Chavarino, D.; Bauça, J.M.; Argente Del Castillo, P.; Ballesteros-Vizoso, M.A.; García de Guadiana-Romualdo, L.; Gómez-Cobo, C.; Pou, J.A.; Amezaga-Menéndez, R.; Alonso-Fernández, A.; et al. Urine Biomarkers for the Prediction of Mortality in COVID-19 Hospitalized Patients. Sci. Rep. 2021, 11, 11134. [Google Scholar] [CrossRef]
- Sundaram, S.; Soni, M.; Annigeri, R. Urine Abnormalities Predict Acute Kidney Injury in COVID-19 Patients: An Analysis of 110 Cases in Chennai, South India. Diabetes Metab. Syndr. 2021, 15, 187–191. [Google Scholar] [CrossRef] [PubMed]
- McAdams, M.C.; Li, M.; Xu, P.; Gregg, L.P.; Patel, J.; Willett, D.L.; Velasco, F.; Lehmann, C.U.; Hedayati, S.S. Using Dipstick Urinalysis to Predict Development of Acute Kidney Injury in Patients with COVID-19. BMC Nephrol. 2022, 23, 50. [Google Scholar] [CrossRef] [PubMed]
- Bi, X.; Liu, W.; Ding, X.; Liang, S.; Zheng, Y.; Zhu, X.; Quan, S.; Yi, X.; Xiang, N.; Du, J.; et al. Proteomic and Metabolomic Profiling of Urine Uncovers Immune Responses in Patients with COVID-19. Cell Rep. 2022, 38, 110271. [Google Scholar] [CrossRef] [PubMed]
- Gross, O.; Moerer, O.; Rauen, T.; Böckhaus, J.; Hoxha, E.; Jörres, A.; Kamm, M.; Elfanish, A.; Windisch, W.; Dreher, M.; et al. Validation of a Prospective Urinalysis-Based Prediction Model for ICU Resources and Outcome of COVID-19 Disease: A Multicenter Cohort Study. J. Clin. Med. 2021, 10, 3049. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-Associated Acute Kidney Injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Gusev, E.; Solomatina, L.; Zhuravleva, Y.; Sarapultsev, A. The Pathogenesis of End-Stage Renal Disease from the Standpoint of the Theory of General Pathological Processes of Inflammation. Int. J. Mol. Sci. 2021, 22, 11453. [Google Scholar] [CrossRef] [PubMed]
- Na, K.R.; Kim, H.R.; Ham, Y.; Choi, D.E.; Lee, K.W.; Moon, J.Y.; Kim, Y.-S.; Cheon, S.; Sohn, K.M.; Kim, J.; et al. Acute Kidney Injury and Kidney Damage in COVID-19 Patients. J. Korean Med. Sci. 2020, 35, e257. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-Cell RNA-Seq Data Analysis on the Receptor ACE2 Expression Reveals the Potential Risk of Different Human Organs Vulnerable to 2019-NCoV Infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Qi, F.; Qian, S.; Zhang, S.; Zhang, Z. Single Cell RNA Sequencing of 13 Human Tissues Identify Cell Types and Receptors of Human Coronaviruses. Biochem. Biophys. Res. Commun. 2020, 526, 135–140. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Wang, R.; Feng, Z.; Zhang, J.; Yang, H.; Tan, Y.; Wang, H.; Wang, C.; Liu, L.; et al. Human Kidney Is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ Distribution of Severe Acute Respiratory Syndrome (SARS) Associated Coronavirus (SARS-CoV) in SARS Patients: Implications for Pathogenesis and Virus Transmission Pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Chu, K.H.; Tsang, W.K.; Tang, C.S.; Lam, M.F.; Lai, F.M.; To, K.F.; Fung, K.S.; Tang, H.L.; Yan, W.W.; Chan, H.W.H.; et al. Acute Renal Impairment in Coronavirus-Associated Severe Acute Respiratory Syndrome. Kidney Int. 2005, 67, 698–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal Histopathological Analysis of 26 Postmortem Findings of Patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling Serum Cytokines in COVID-19 Patients Reveals IL-6 and IL-10 Are Disease Severity Predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Bennett, T.D.; Moffitt, R.A.; Hajagos, J.G.; Amor, B.; Anand, A.; Bissell, M.M.; Bradwell, K.R.; Bremer, C.; Byrd, J.B.; Denham, A.; et al. Clinical Characterization and Prediction of Clinical Severity of SARS-CoV-2 Infection Among US Adults Using Data From the US National COVID Cohort Collaborative. JAMA Netw. Open 2021, 4, e2116901. [Google Scholar] [CrossRef] [PubMed]
- Welder, D.; Jeon-Slaughter, H.; Ashraf, B.; Choi, S.-H.; Chen, W.; Ibrahim, I.; Bat, T. Immature Platelets as a Biomarker for Disease Severity and Mortality in COVID-19 Patients. Br. J. Haematol. 2021, 194, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Copaescu, A.; James, F.; Mouhtouris, E.; Vogrin, S.; Smibert, O.C.; Gordon, C.L.; Drewett, G.; Holmes, N.E.; Trubiano, J.A. The Role of Immunological and Clinical Biomarkers to Predict Clinical COVID-19 Severity and Response to Therapy—A Prospective Longitudinal Study. Front. Immunol. 2021, 12, 758. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 178) | ICU (n = 52) | Non-ICU (n = 126) | ap Value | |
|---|---|---|---|---|
| Age (Years) | 47.0 (35.0–61.0) | 56.50 (40.5–65.5) | 45.0 (32.8–57.0) | <0.001 |
| Gender | ||||
| male | 72 (40.4) | 32 (61.5) | 40 (31.7) | <0.001 |
| female | 106 (59.6) | 20 (38.5) | 86 (68.3) | <0.001 |
| Signs and symptoms | ||||
| Fever | 148 (83.1) | 46 (88.5) | 100 (79.4) | 0.199 |
| Body temperature (max.) (°C) | 38.5 (37.8–39.0) | 39 (38.1–39.1) | 38.3 (37.7–39.0) | 0.005 |
| >38 | 110 (61.8) | 39 (75) | 71 (56.3) | 0.020 |
| Shortness of breath | 39 (21.9) | 13 (25) | 26 (20.6) | 0.553 |
| Cough | 128 (71.9) | 49 (94.2) | 79 (62.3) | <0.001 |
| Hypoxemia | 30 (16.9) | 17 (32.7) | 13 (10.3) | <0.001 |
| Chest tightness | 35 (19.7) | 13 (25) | 22 (17.5) | 0.300 |
| Fatigue | 41 (23.0) | 16 (30.8) | 25 (19.8) | 0.122 |
| Myalgia | 49 (27.5) | 17 (32.7) | 32 (25.4) | 0.358 |
| Headache | 12 (6.7) | 4 (7.7) | 8 (6.3) | 0.748 |
| Oxygen application | 121 (68.0) | 50 (96.2) | 71 (56.3) | <0.001 |
| Severe case | 81 (45.5) | 45 (86.5) | 36 (28.6) | <0.001 |
| Basic diseases | ||||
| hypertension | 29 (16.3) | 15 (28.8) | 14 (11.1) | 0.007 |
| hyperlipidemia | 3 (1.7) | 1 (1.9) | 2 (1.6) | >0.999 |
| diabetes | 19 (10.7) | 9 (17.3) | 10 (7.9) | 0.106 |
| digestive system | 10 (5.6) | 4 (7.7) | 6 (4.8) | 0.481 |
| respiratory system | 10 (5.6) | 4 (7.7) | 6 (4.8) | 0.481 |
| cardiovascular | 10 (5.6) | 7(13.5) | 3 (2.4) | 0.007 |
| cancer | 8 (4.5) | 1 (1.9) | 7 (5.6) | 0.440 |
| urinary system | 4 (2.2) | 2 (3.8) | 2 (1.6) | 0.581 |
| Others | 23 (12.9) | 5 (9.6) | 18 (14.3) | 0.47 |
| Non-basic diseases | 100 (56.2) | 19 (36.5) | 81 (64.3) | <0.001 |
| Scr (μmol/L) | 65.2 (56.8–74.8) | 71.0 (55.8–89.4) | 65.3 (56.5–74.3) | 0.067 |
| increase | 0 | 0 | 0 | >0.999 |
| BUN (mmol/L) | 3.81 (2.83–4.54) | 4.14 (3.33–4.82) | 3.72 (2.76–4.57) | 0.078 |
| increase | 5 (2.8) | 3 (5.8) | 2 (1.6) | 0.150 |
| eGFR (ml/min) | 214.6 (308.05) | 93.7 (78.1–108.0) | 102.5 (90.7–113.1) | 0.014 |
| decrease | 42 (23.6) | 19 (36.5) | 23 (18.3) | 0.009 |
| Cystatin C (mg/L) | 0.77 (0.68–0.86) | 0.81 (0.73–0.88) | 0.77 (0.68–0.87) | 0.155 |
| increase | 3 (1.7) | 1 (1.9) | 2 (1.6) | >0.999 |
| Total (n = 83) | ICU (n = 19) | Non-IC (n = 64) | ap Value | |
|---|---|---|---|---|
| Abnormal urine routine | 45 (54.2) | 15 (78.9) | 30 (46.9) | 0.014 |
| Proteinuria | ||||
| positive | 29 (34.9) | 11(57.9) | 18 (28.1) | 0.017 |
| Hematuria | ||||
| positive | 24 (28.9) | 10 (52.6) | 14 (21.9) | 0.009 |
| Leucocyturia | ||||
| positive | 14 (16.9) | 2 (10.5) | 12 (18.8) | 0.506 |
| Urine glucose | ||||
| positive | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Urine urothelial cell | ||||
| positive | 10 (12) | 1 (5.3) | 9 (14.1) | 0.441 |
| Urine specific weight | 1.022 ± 0.00118 | 1.027 ± 0.011 | 1.021 ± 0.012 | 0.003 |
| Medications before Admission | Total (n = 83) | AU (n = 45) | NU (n = 38) | ap Value |
|---|---|---|---|---|
| Antibiotic | 25 (30.1) | 11 (35.5) | 14 (26.9) | 0.411 |
| Oseltamivir/Lopinavir | 12 (14.5) | 7 (22.6) | 5 (9.6) | 0.119 |
| Arbidol | 16 (19.3) | 9 (29.0) | 7 (13.5) | 0.082 |
| Chinese Patent Medicine | 9 (10.8) | 3 (9.7) | 6 (11.5) | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Zhang, Z.; Dobrinina, M.; Dong, Y.; Kang, Z.; Chereshnev, V.; Hu, D.; Zhang, Z.; Zhang, J.; Sarapultsev, A. Urinalysis, but Not Blood Biochemistry, Detects the Early Renal Impairment in Patients with COVID-19. Diagnostics 2022, 12, 602. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030602
Zhou H, Zhang Z, Dobrinina M, Dong Y, Kang Z, Chereshnev V, Hu D, Zhang Z, Zhang J, Sarapultsev A. Urinalysis, but Not Blood Biochemistry, Detects the Early Renal Impairment in Patients with COVID-19. Diagnostics. 2022; 12(3):602. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030602
Chicago/Turabian StyleZhou, Haifeng, Zili Zhang, Maria Dobrinina, Yalan Dong, Zhenyu Kang, Valerii Chereshnev, Desheng Hu, Zhe Zhang, Jun Zhang, and Alexey Sarapultsev. 2022. "Urinalysis, but Not Blood Biochemistry, Detects the Early Renal Impairment in Patients with COVID-19" Diagnostics 12, no. 3: 602. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030602