
Fast, Accurate, and Robust T2 Mapping of Articular Cartilage by Neural Networks

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. In Silico Study Phase—Synthetic MRI Data
2.3. In Situ Study Phase—MRI Measurements

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| “Low-SNR” Sequence | “High-SNR” Sequence | |
|---|---|---|
| Sequence Type | 2D MESE | |
| Orientation | Axial | |
| Repetition Time [ms] | 500 | |
| Echo Times [ms] | ||
| Field of View [mm] | 140 × 140 | |
| Acquisition Matrix | 512 × 512 | |
| Reconstruction Matrix | 512 × 512 | |
| Scan percentage [%] | 100 | |
| Flip angle [°] | 90 | |
| Number of Signal Averages [n] | 1 | 4 |
| SENSE Factor | 3 | 1 |
| Slices [n] | 1 | |
| Slice Thickness [mm] | 2 | |
| Duration [min:s] | 2:15 | 26:34 |
2.4. Fitting Methods
- (1)
- Traditional LSE without any modification (LSE);
- (2)
- Offset LSE (OLSE);
- (3)
- Noise-Corrected LSE (NCLSE).
2.5. Computation Time
2.6. Statistical Analysis
3. Results
3.1. In Silico Fitting Results
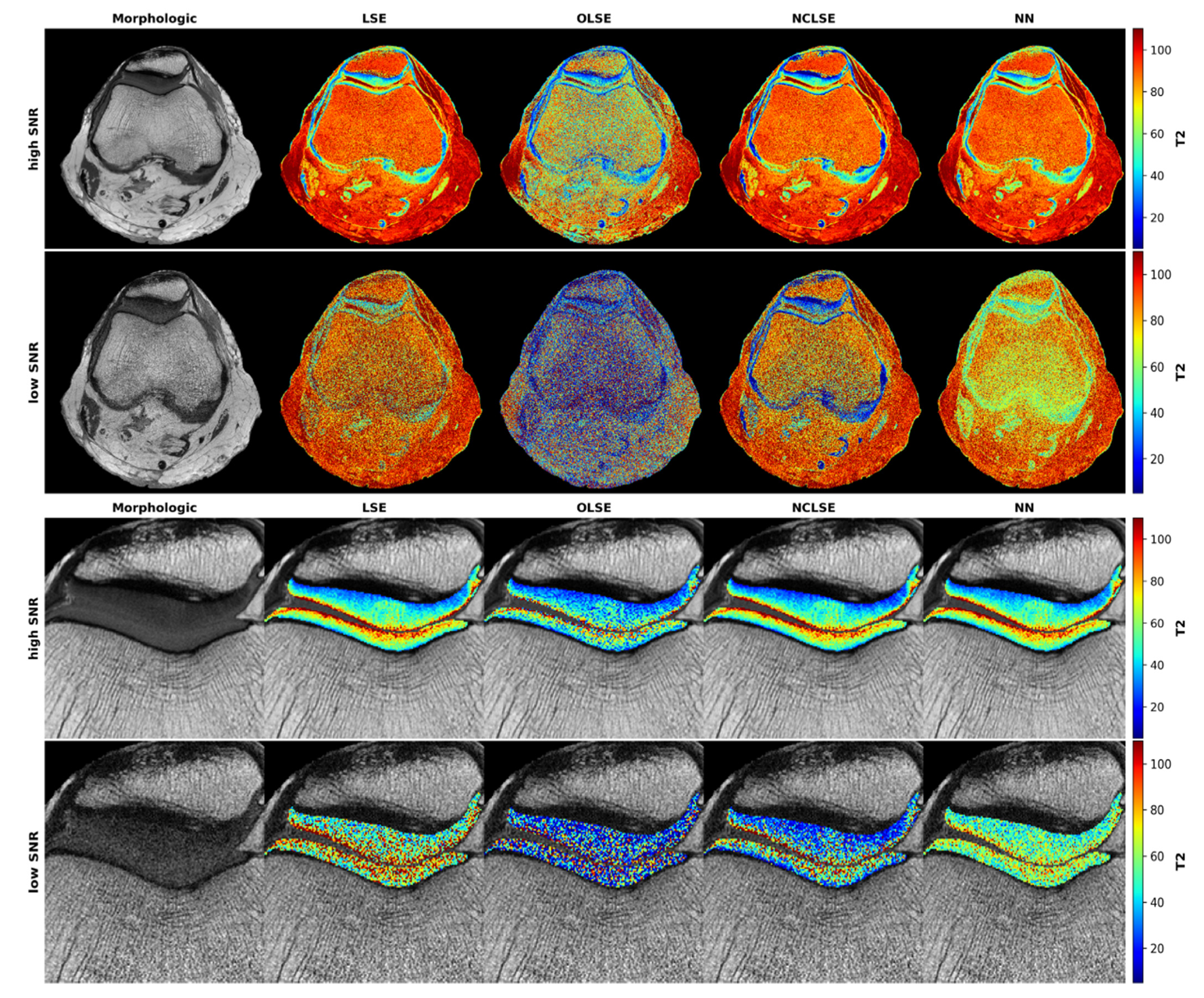
3.2. In Situ Fitting Results
3.3. Computation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Glyn-Jones, S.; Palmer, A.J.R.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Crema, M.D.; Roemer, F.W.; Marra, M.D.; Burstein, D.; Gold, G.E.; Eckstein, F.; Baum, T.; Mosher, T.J.; Carrino, J.A.; Guermazi, A. Articular Cartilage in the Knee: Current MR Imaging Techniques and Applications in Clinical Practice and Research. RadioGraphics 2011, 31, 37–61. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Carrasco, M.A.; Moraga, C.; Delgado, I. Knee Chondral Lesions: Incidence and Correlation between Arthroscopic and Magnetic Resonance Findings. Arthroscopy 2007, 23, 312–315. [Google Scholar] [CrossRef]
- Von Engelhardt, L.V.; Kraft, C.N.; Pennekamp, P.H.; Schild, H.H.; Schmitz, A.; von Falkenhausen, M. The Evaluation of Articular Cartilage Lesions of the Knee with a 3-Tesla Magnet. Arthroscopy 2007, 23, 496–502. [Google Scholar] [CrossRef]
- Baum, T.; Joseph, G.B.; Karampinos, D.C.; Jungmann, P.M.; Link, T.M.; Bauer, J.S. Cartilage and Meniscal T2 Relaxation Time as Non-Invasive Biomarker for Knee Osteoarthritis and Cartilage Repair Procedures. Osteoarthr. Cartil. 2013, 21, 1474–1484. [Google Scholar] [CrossRef] [Green Version]
- Guermazi, A.; Alizai, H.; Crema, M.D.; Trattnig, S.; Regatte, R.R.; Roemer, F.W. Compositional MRI Techniques for Evaluation of Cartilage Degeneration in Osteoarthritis. Osteoarthr. Cartil. 2015, 23, 1639–1653. [Google Scholar] [CrossRef] [Green Version]
- Huppertz, M.S.; Schock, J.; Radke, K.L.; Abrar, D.B.; Post, M.; Kuhl, C.; Truhn, D.; Nebelung, S. Longitudinal T2 Mapping and Texture Feature Analysis in the Detection and Monitoring of Experimental Post-Traumatic Cartilage Degeneration. Life 2021, 11, 201. [Google Scholar] [CrossRef]
- Linka, K.; Itskov, M.; Truhn, D.; Nebelung, S.; Thüring, J. T2 MR Imaging vs. Computational Modeling of Human Articular Cartilage Tissue Functionality. J. Mech. Behav. Biomed. Mater. 2017, 74, 477–487. [Google Scholar] [CrossRef]
- Kretzschmar, M.; Nevitt, M.C.; Schwaiger, B.J.; Joseph, G.B.; McCulloch, C.E.; Link, T.M. Spatial Distribution and Temporal Progression of T2 Relaxation Time Values in Knee Cartilage Prior to the Onset of Cartilage Lesions—Data from the Osteoarthritis Initiative (OAI). Osteoarthr. Cartil. 2019, 27, 737–745. [Google Scholar] [CrossRef]
- Baselice, F.; Ferraioli, G.; Grassia, A.; Pascazio, V. Optimal Configuration for Relaxation Times Estimation in Complex Spin Echo Imaging. Sensors 2014, 14, 2182–2198. [Google Scholar] [CrossRef] [Green Version]
- Grussu, F.; Battiston, M.; Palombo, M.; Schneider, T.; Gandini Wheeler-Kingshott, C.A.M.; Alexander, D.C. Deep Learning Model Fitting for Diffusion-Relaxometry: A Comparative Study. In Computational Diffusion MRI; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Raya, J.G.; Dietrich, O.; Horng, A.; Weber, J.; Reiser, M.F.; Glaser, C. T2 Measurement in Articular Cartilage: Impact of the Fitting Method on Accuracy and Precision at Low SNR. Magn. Reson. Med. 2009, 63, 181–193. [Google Scholar] [CrossRef]
- Keene, K.R.; Beenakker, J.M.; Hooijmans, M.T.; Naarding, K.J.; Niks, E.H.; Otto, L.A.M.; Pol, W.L.; Tannemaat, M.R.; Kan, H.E.; Froeling, M. T2 Relaxation—Time Mapping in Healthy and Diseased Skeletal Muscle Using Extended Phase Graph Algorithms. Magn. Reson. Med. 2020, 84, 2656–2670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Eliezer, N.; Sodickson, D.K.; Block, K.T. Rapid and Accurate T2 Mapping from Multi-Spin-Echo Data Using Bloch-Simulation-Based Reconstruction: Mapping Using Bloch-Simulation-Based Reconstruction. Magn. Reson. Med. 2015, 73, 809–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebel, R.M.; Wilman, A.H. Transverse Relaxometry with Stimulated Echo Compensation. Magn. Reson. Med. 2010, 64, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; He, T.; Feng, M.; Carpenter, J.-P.; Greiser, A.; Xin, X.; Chen, W.; Pennell, D.J.; Yang, G.-Z.; Firmin, D.N. Improved Pixel-by-Pixel MRI R2* Relaxometry by Nonlocal Means: Improved R2* Mapping by Nonlocal Means. Magn. Reson. Med. 2014, 72, 260–268. [Google Scholar] [CrossRef]
- Marro, K.; Otto, R.; Kolokythas, O.; Shimamura, A.; Sanders, J.E.; McDonald, G.B.; Friedman, S.D. A Simulation-Based Comparison of Two Methods for Determining Relaxation Rates from Relaxometry Images. Magn. Reson. Imaging 2011, 29, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Diskin, T.; Draskovic, G.; Pascal, F.; Wiesel, A. Deep Robust Regression. In Proceedings of the 2017 IEEE 7th International Workshop on Computational Advances in Multi-Sensor Adaptive Processing (CAMSAP), Curaçao, The Netherlands, 10–13 December 2017; pp. 1–5. [Google Scholar]
- Yu, C.; Yao, W. Robust Linear Regression: A Review and Comparison. Commun. Stat. Simul. Comput. 2017, 46, 6261–6282. [Google Scholar] [CrossRef]
- Koff, M.F.; Amrami, K.K.; Felmlee, J.P.; Kaufman, K.R. Bias of Cartilage T2 Values Related to Method of Calculation. Magn. Reson. Imaging 2008, 26, 1236–1243. [Google Scholar] [CrossRef] [Green Version]
- MacKay, J.W.; Low, S.B.L.; Smith, T.O.; Toms, A.P.; McCaskie, A.W.; Gilbert, F.J. Systematic Review and Meta-Analysis of the Reliability and Discriminative Validity of Cartilage Compositional MRI in Knee Osteoarthritis. Osteoarthr. Cartil. 2018, 26, 1140–1152. [Google Scholar] [CrossRef] [Green Version]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A Survey on Deep Learning in Medical Image Analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Beliakov, G.; Kelarev, A.; Yearwood, J. Derivative-Free Optimization and Neural Networks for Robust Regression. Optimization 2012, 61, 1467–1490. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Feng, L.; Kijowski, R. MANTIS: Model-Augmented Neural NeTwork with Incoherent K-space Sampling for Efficient MR Parameter Mapping. Magn. Reson. Med. 2019, 82, 174–188. [Google Scholar] [CrossRef] [PubMed]
- Zibetti, M.V.W.; Johnson, P.M.; Sharafi, A.; Hammernik, K.; Knoll, F.; Regatte, R.R. Rapid Mono and Biexponential 3D-T1ρ Mapping of Knee Cartilage Using Variational Networks. Sci. Rep. 2020, 10, 19144. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Canales-Rodríguez, E.J.; Pizzolato, M.; Piredda, G.F.; Hilbert, T.; Fischi-Gomez, E.; Weigel, M.; Barakovic, M.; Bach Cuadra, M.; Granziera, C.; et al. Model-Informed Machine Learning for Multi-Component T 2 Relaxometry. Med. Image Anal. 2021, 69, 101940. [Google Scholar] [CrossRef] [PubMed]
- Meadows, K.D.; Johnson, C.L.; Peloquin, J.M.; Spencer, R.G.; Vresilovic, E.J.; Elliott, D.M. Impact of Pulse Sequence, Analysis Method, and Signal to Noise Ratio on the Accuracy of Intervertebral Disc T2 Measurement. JOR Spine 2020, 3, e1102. [Google Scholar] [CrossRef]
- Otto, R.; Ferguson, M.R.; Marro, K.; Grinstead, J.W.; Friedman, S.D. Limitations of Using Logarithmic Transformation and Linear Fitting to Estimate Relaxation Rates in Iron-Loaded Liver. Pediatr. Radiol. 2011, 41, 1259–1265. [Google Scholar] [CrossRef]
- Sbrizzi, A.; van der Heide, O.; Cloos, M.; van der Toorn, A.; Hoogduin, H.; Luijten, P.R.; van den Berg, C.A.T. Fast Quantitative MRI as a Nonlinear Tomography Problem. Magn. Reson. Imaging 2018, 46, 56–63. [Google Scholar] [CrossRef]
- Gudbjartsson, H.; Patz, S. The Rician Distribution of Noisy MRI Data. Magn. Reson. Med. 1995, 34, 910–914. [Google Scholar] [CrossRef]
- Aja-Fernández, S.; Vegas-Sánchez-Ferrero, G. Statistical Analysis of Noise in MRI; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-39933-1. [Google Scholar]
- Milford, D.; Rosbach, N.; Bendszus, M.; Heiland, S. Mono-Exponential Fitting in T2-Relaxometry: Relevance of Offset and First Echo. PLoS ONE 2015, 10, e0145255. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; He, T.; Gatehouse, P.D.; Li, X.; Harith Alam, M.; Pennell, D.J.; Chen, W.; Firmin, D.N. Improved MRI R2* Relaxometry of Iron-Loaded Liver with Noise Correction: Improved MRI R2* for Liver Iron Quantification. Magn. Reson. Med. 2013, 70, 1765–1774. [Google Scholar] [CrossRef]
- Michálek, J.; Hanzlíková, P.; Trinh, T.; Pacík, D. Fast and Accurate Compensation of Signal Offset for T2 Mapping. Magn. Reson. Mater. Phy. 2019, 32, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Limpert, E.; Stahel, W.A.; Abbt, M. Log-Normal Distributions across the Sciences: Keys and Clues. BioScience 2001, 51, 341. [Google Scholar] [CrossRef]
- Canales-Rodríguez, E.J.; Pizzolato, M.; Piredda, G.F.; Hilbert, T.; Kunz, N.; Pot, C.; Yu, T.; Salvador, R.; Pomarol-Clotet, E.; Kober, T.; et al. Comparison of Non-Parametric T2 Relaxometry Methods for Myelin Water Quantification. Med. Image Anal. 2021, 69, 101959. [Google Scholar] [CrossRef] [PubMed]
- Aja-Fernandez, S.; Alberola-Lopez, C.; Westin, C.-F. Noise and Signal Estimation in Magnitude MRI and Rician Distributed Images: A LMMSE Approach. IEEE Trans. Image Process. 2008, 17, 1383–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and Reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Peterfy, C.G.; Schneider, E.; Nevitt, M. The Osteoarthritis Initiative: Report on the Design Rationale for the Magnetic Resonance Imaging Protocol for the Knee. Osteoarthr. Cartil. 2008, 16, 1433–1441. [Google Scholar] [CrossRef] [Green Version]
- Foi, A. Noise Estimation and Removal in MR Imaging: The Variance-Stabilization Approach. In Proceedings of the 2011 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Chicago, IL, USA, 30 March–2 April 2011; pp. 1809–1814. [Google Scholar]
- Pieciak, T.; Aja-Fernandez, S.; Vegas-Sanchez-Ferrero, G. Non-Stationary Rician Noise Estimation in Parallel MRI Using a Single Image: A Variance-Stabilizing Approach. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2015–2029. [Google Scholar] [CrossRef] [Green Version]
- Aja-Fernández, S.; Pie¸ciak, T.; Vegas-Sánchez-Ferrero, G. Spatially Variant Noise Estimation in MRI: A Homomorphic Approach. Med. Image Anal. 2015, 20, 184–197. [Google Scholar] [CrossRef]
- Aja-Fernández, S.; Vegas-Sánchez-Ferrero, G.; Tristán-Vega, A. Noise Estimation in Parallel MRI: GRAPPA and SENSE. Magn. Reson. Imaging 2014, 32, 281–290. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2017, arXiv:1412.6980. [Google Scholar]
- Girshick, R. Fast R-CNN. In Proceedings of the 2015 IEEE International Conference on Computer Vision (ICCV), Santiago, Chile, 11–18 December 2015; pp. 1440–1448. [Google Scholar]
- Drenthen, G.S.; Backes, W.H.; Aldenkamp, A.P.; Op’t Veld, G.J.; Jansen, J.F.A. A New Analysis Approach for T2 Relaxometry Myelin Water Quantification: Orthogonal Matching Pursuit. Magn. Reson. Med. 2018, 81, 3292–3303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedoia, V.; Lee, J.; Norman, B.; Link, T.M.; Majumdar, S. Diagnosing Osteoarthritis from T2 Maps Using Deep Learning: An Analysis of the Entire Osteoarthritis Initiative Baseline Cohort. Osteoarthr. Cartil. 2019, 27, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Divine, G.W.; Norton, H.J.; Barón, A.E.; Juarez-Colunga, E. The Wilcoxon–Mann–Whitney Procedure Fails as a Test of Medians. Am. Stat. 2018, 72, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Statistics Notes: Multiple Significance Tests: The Bonferroni Method. BMJ 1995, 310, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouhrara, M.; Reiter, D.A.; Celik, H.; Bonny, J.-M.; Lukas, V.; Fishbein, K.W.; Spencer, R.G. Incorporation of Rician Noise in the Analysis of Biexponential Transverse Relaxation in Cartilage Using a Multiple Gradient Echo Sequence at 3 and 7 Tesla: Rician Noise and Analysis of Relaxation. Magn. Reson. Med. 2015, 73, 352–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupé, P.; Manjón, J.V.; Gedamu, E.; Arnold, D.; Robles, M.; Collins, D.L. Robust Rician Noise Estimation for MR Images. Med. Image Anal. 2010, 14, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Abrar, D.B.; Schleich, C.; Radke, K.L.; Frenken, M.; Stabinska, J.; Ljimani, A.; Wittsack, H.-J.; Antoch, G.; Bittersohl, B.; Hesper, T.; et al. Detection of Early Cartilage Degeneration in the Tibiotalar Joint Using 3 T GagCEST Imaging: A Feasibility Study. Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 249–260. [Google Scholar] [CrossRef]
- Nebelung, S.; Sondern, B.; Jahr, H.; Tingart, M.; Knobe, M.; Thüring, J.; Kuhl, C.; Truhn, D. Non-Invasive T1ρ Mapping of the Human Cartilage Response to Loading and Unloading. Osteoarthr. Cartil. 2018, 26, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Müller-Lutz, A.; Kamp, B.; Nagel, A.M.; Ljimani, A.; Abrar, D.; Schleich, C.; Wollschläger, L.; Nebelung, S.; Wittsack, H.-J. Sodium MRI of Human Articular Cartilage of the Wrist: A Feasibility Study on a Clinical 3T MRI Scanner. Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 241–248. [Google Scholar] [CrossRef]
- Englund, M.; Guermazi, A.; Roemer, F.W.; Aliabadi, P.; Yang, M.; Lewis, C.E.; Torner, J.; Nevitt, M.C.; Sack, B.; Felson, D.T. Meniscal Tear in Knees without Surgery and the Development of Radiographic Osteoarthritis among Middle-Aged and Elderly Persons: The Multicenter Osteoarthritis Study. Arthritis Rheum 2009, 60, 831–839. [Google Scholar] [CrossRef] [Green Version]
- Balamoody, S.; Williams, T.G.; Wolstenholme, C.; Waterton, J.C.; Bowes, M.; Hodgson, R.; Zhao, S.; Scott, M.; Taylor, C.J.; Hutchinson, C.E. Magnetic Resonance Transverse Relaxation Time T2 of Knee Cartilage in Osteoarthritis at 3-T: A Cross-Sectional Multicentre, Multivendor Reproducibility Study. Skelet. Radiol 2013, 42, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Obuchowski, N.A.; Reeves, A.P.; Huang, E.P.; Wang, X.-F.; Buckler, A.J.; Kim, H.J.; Barnhart, H.X.; Jackson, E.F.; Giger, M.L.; Pennello, G.; et al. Quantitative Imaging Biomarkers: A Review of Statistical Methods for Computer Algorithm Comparisons. Stat. Methods Med. Res. 2015, 24, 68–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robson, M.D.; Gatehouse, P.D.; Bydder, M.; Bydder, G.M. Magnetic Resonance: An Introduction to Ultrashort TE (UTE) Imaging. J. Comput. Assist. Tomogr. 2003, 27, 825–846. [Google Scholar] [CrossRef] [PubMed]
- McPhee, K.C.; Wilman, A.H. Limitations of Skipping Echoes for Exponential T2 Fitting: Skipped Echo Exponential T2 Fitting. J. Magn. Reson. Imaging 2018, 48, 1432–1440. [Google Scholar] [CrossRef]
- Shao, J.; Ghodrati, V.; Nguyen, K.; Hu, P. Fast and Accurate Calculation of Myocardial T1 and T2 Values Using Deep Learning Bloch Equation Simulations (DeepBLESS). Magn. Reson. Med. 2020, 84, 2831–2845. [Google Scholar] [CrossRef]



| SNR = 5 | SNR = 10 | SNR = 20 | SNR = 30 | |
|---|---|---|---|---|
| LSE | 43 [2, 650] | 19 [1, 199] | 9 [0, 63] | 6 [0, 39] |
| OLSE | 61 [3, 439] | 33 [1, 115] | 17 [1, 94] | 11 [0, 90] |
| NCLSE | 34 [2, 509] | 17 [1, 175] | 8 [0, 61] | 5 [0, 39] |
| NN | 28 [1, 160] | 16 [1, 83] | 8 [0, 47] | 6 [0, 34] |
| Entire Joint | Patellofemoral Cartilage | |
|---|---|---|
| LSE | 19 [1, 500] | 33 [1, 651] |
| OLSE | 47 [2, 236] | 58 [2, 398] |
| NCLSE | 20 [1, 381] | 35 [1, 513] |
| NN | 16 [1, 79] | 23 [1, 120] |
| LSE | OLSE | NCLSE | NN | |
|---|---|---|---|---|
| Computation Time [s] | 28 | 43 | 40 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller-Franzes, G.; Nolte, T.; Ciba, M.; Schock, J.; Khader, F.; Prescher, A.; Wilms, L.M.; Kuhl, C.; Nebelung, S.; Truhn, D. Fast, Accurate, and Robust T2 Mapping of Articular Cartilage by Neural Networks. Diagnostics 2022, 12, 688. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030688
Müller-Franzes G, Nolte T, Ciba M, Schock J, Khader F, Prescher A, Wilms LM, Kuhl C, Nebelung S, Truhn D. Fast, Accurate, and Robust T2 Mapping of Articular Cartilage by Neural Networks. Diagnostics. 2022; 12(3):688. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030688
Chicago/Turabian StyleMüller-Franzes, Gustav, Teresa Nolte, Malin Ciba, Justus Schock, Firas Khader, Andreas Prescher, Lena Marie Wilms, Christiane Kuhl, Sven Nebelung, and Daniel Truhn. 2022. "Fast, Accurate, and Robust T2 Mapping of Articular Cartilage by Neural Networks" Diagnostics 12, no. 3: 688. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030688