
French Survey on Pain Perception and Management in Patients with Locked-In Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Information and Clinical Status
3.2. Past and Current Pain
3.3. Factors That Influence Pain
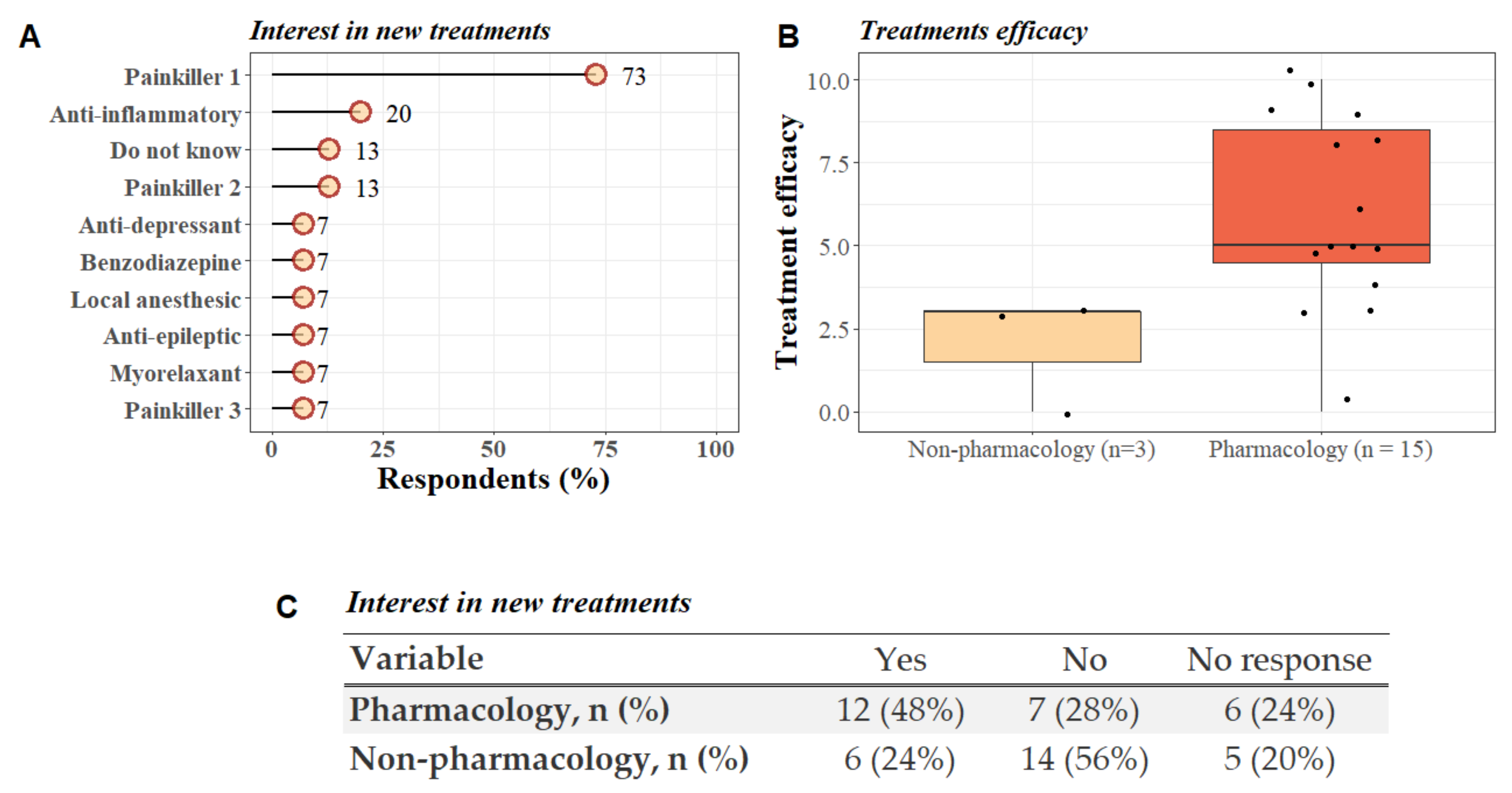
3.4. Treatments
4. Discussion
4.1. Past and Current Pain
4.2. Factors That Influence Pain
4.3. Treatments
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johncy, N.; Shabaraya, A.R. Review on Locked-in Syndrome. IJRR 2020, 7, 392–396. [Google Scholar]
- Laureys, S.; Pellas, F.; Van Eeckhout, P.; Ghorbel, S.; Schnakers, C.; Perrin, F.; Berré, J.; Faymonville, M.-E.; Pantke, K.-H.; Damas, F.; et al. The Locked-in Syndrome: What Is It like to Be Conscious but Paralyzed and Voiceless? Prog. Brain Res. 2005, 150, 495–611. [Google Scholar] [PubMed]
- Maiser, S.; Kabir, A.; Sabsevitz, D.; Peltier, W. Locked-In Syndrome: Case Report and Discussion of Decisional Capacity. J. Pain Symptom Manag. 2016, 51, 789–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- León-Carrión, J.; Van Eeckhout, P.; Domínguez-Morales, M.d.R.; Pérez-Santamaría, F.J. Survey: The Locked-in Syndrome: A Syndrome Looking for a Therapy. Brain Inj. 2002, 16, 571–582. [Google Scholar] [CrossRef]
- Demertzi, A.; Racine, E.; Bruno, M.-A.; Ledoux, D.; Gosseries, O.; Vanhaudenhuyse, A.; Thonnard, M.; Soddu, A.; Moonen, G.; Laureys, S. Pain Perception in Disorders of Consciousness: Neuroscience, Clinical Care, and Ethics in Dialogue. Neuroethics 2013, 6, 37–50. [Google Scholar] [CrossRef] [Green Version]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The Minimally Conscious State: Definition and Diagnostic Criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive Wakefulness Syndrome: A New Name for the Vegetative State or Apallic Syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Gallo, U.E.; Fontanarosa, P.B. Locked-in Syndrome: Report of a Case. Am. J. Emerg. Med. 1989, 7, 581–583. [Google Scholar] [CrossRef]
- Schnakers, C.; Majerus, S.; Laureys, S. Diagnostic et évaluation des états de conscience altérée. Diagnosis and investigation of altered states of consciousness. Reanimation 2004, 13, 368–375. [Google Scholar] [CrossRef]
- León-Carrión, J.; van Eeckhout, P.; Domínguez-Morales, M.d.R. Review of Subject: The Locked-in Syndrome: A Syndrome Looking for a Therapy. Brain Inj. 2002, 16, 555–569. [Google Scholar] [CrossRef]
- Michaelides, A.; Zis, P. Depression, Anxiety and Acute Pain: Links and Management Challenges. Postgrad. Med. 2019, 131, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Wilson, H.D.; Cahana, A. Treatment of Chronic Non-Cancer Pain. Lancet 2011, 377, 2226–2235. [Google Scholar] [CrossRef]
- Bouhassira, D. Neuropathic Pain: Definition, Assessment and Epidemiology. Rev. Neurol. 2019, 175, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Pistoia, F.; Sacco, S.; Sarà, M.; Franceschini, M.; Carolei, A. Intrathecal Baclofen: Effects on Spasticity, Pain, and Consciousness in Disorders of Consciousness and Locked-in Syndrome. Curr. Pain Headache Rep. 2015, 19, 466. [Google Scholar] [CrossRef]
- Boly, M.; Faymonville, M.-E.; Schnakers, C.; Peigneux, P.; Lambermont, B.; Phillips, C.; Lancellotti, P.; Luxen, A.; Lamy, M.; Moonen, G.; et al. Perception of Pain in the Minimally Conscious State with PET Activation: An Observational Study. Lancet Neurol. 2008, 7, 1013–1020. [Google Scholar] [CrossRef]
- Laureys, S.; Faymonville, M.E.; Peigneux, P.; Damas, P.; Lambermont, B.; Del Fiore, G.; Degueldre, C.; Aerts, J.; Luxen, A.; Franck, G.; et al. Cortical Processing of Noxious Somatosensory Stimuli in the Persistent Vegetative State. NeuroImage 2002, 17, 732–741. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice Guideline Update Recommendations Summary: Disorders of Consciousness. Arch. Phys. Med. Rehabil. 2018, 99, 1699–1709. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Manuli, A.; Leo, A.; De Luca, R.; Lo Buono, V.; Russo, M.; Bramanti, A.; Bramanti, P. Pain Perception in Patients with Chronic Disorders of Consciousness: What Can Limbic System Tell Us? Clin. Neurophysiol. 2017, 128, 454–462. [Google Scholar] [CrossRef]
- Bruno, M.-A.; Bernheim, J.L.; Ledoux, D.; Pellas, F.; Demertzi, A.; Laureys, S. A Survey on Self-Assessed Well-Being in a Cohort of Chronic Locked-in Syndrome Patients: Happy Majority, Miserable Minority. BMJ Open 2011, 1, e000039. [Google Scholar] [CrossRef] [Green Version]
- Bergés, I.-M.; Ottenbacher, K.J.; Kuo, Y.-F.; Smith, P.M.; Smith, D.; Ostir, G.V. Satisfaction With Quality of Life Poststroke: Effect of Sex Differences in Pain Response. Arch. Phys. Med. Rehabil. 2007, 88, 413–417. [Google Scholar] [CrossRef] [Green Version]
- Skevington, S.M. Investigating the Relationship between Pain and Discomfort and Quality of Life, Using the WHOQOL. Pain 1998, 76, 395–406. [Google Scholar] [CrossRef]
- Glare, P.A.; Davies, P.S.; Finlay, E.; Gulati, A.; Lemanne, D.; Moryl, N.; Oeffinger, K.C.; Paice, J.A.; Stubblefield, M.D.; Syrjala, K.L. Pain in Cancer Survivors. JCO 2014, 32, 1739–1747. [Google Scholar] [CrossRef] [Green Version]
- Westerlind, E.; Singh, R.; Persson, H.C.; Sunnerhagen, K.S. Experienced Pain after Stroke: A Cross-Sectional 5-Year Follow-up Study. BMC Neurol. 2020, 20, 4. [Google Scholar] [CrossRef] [PubMed]
- Staud, R.; Rodriguez, M.E. Mechanisms of Disease: Pain in Fibromyalgia Syndrome. Nat. Rev. Rheumatol. 2006, 2, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, M.-C.; Baumstarck, K.; Alessandrini, M.; Blandin, V.; Billette de Villemeur, T.; Auquier, P. Quality of Life in Patients with Locked-in Syndrome: Evolution over a 6-Year Period. Orphanet. J. Rare Dis. 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of Pain Syndromes Associated with Nervous or Somatic Lesions and Development of a New Neuropathic Pain Diagnostic Questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO Guidelines for the Use of Analgesics in Cancer Pain. Int. J. Tissue React. 1985, 7, 93–96. [Google Scholar]
- Hamani, C.; Fonoff, E.T.; Parravano, D.C.; Silva, V.A.; Galhardoni, R.; Monaco, B.; Navarro, J.; Yeng, L.T.; Teixeira, M.J.; Ciampi de Andrade, D. Motor Cortex Stimulation for Chronic Neuropathic Pain: Results of a Double-Blind Randomized Study. Brain 2021, 144, 2994–3004. [Google Scholar] [CrossRef]
- Annen, J.; Laureys, S.; Gosseries, O. Brain-Computer Interfaces for Consciousness Assessment and Communication in Severely Brain-Injured Patients. Handb. Clin. Neurol. 2020, 168, 137–152. [Google Scholar]
- O’Brien, E.M.; Waxenberg, L.B.; Gremillion, H.A.; Robinson, M.E. Intraindividual Variability in Daily Sleep and Pain Ratings Among Chronic Pain Patients: Bidirectional Association and the Role of Negative Mood. Clin. J. Pain 2011, 27, 9. [Google Scholar] [CrossRef]
- Akınoğlu, B.; Aytül Çakci, F. Role of Physiotherapy and Rehabilitation with Cooperation of Family in Locked-in Syndrome: Four-Year Follow-up of a CaseE. Turk. J. Physiother. Rehabil. 2018, 29, 95–99. [Google Scholar] [CrossRef]
- Vanhaudenhuyse, A.; Nyssen, A.-S.; Faymonville, M.-E. Recent Insight on How the Neuroscientific Approach Helps Clinicians. OBM ICM 2020, 5, 1–20. [Google Scholar] [CrossRef]
- Grant, J.A.; Courtemanche, J.; Rainville, P. A Non-Elaborative Mental Stance and Decoupling of Executive and Pain-Related Cortices Predicts Low Pain Sensitivity in Zen Meditators. Pain 2011, 152, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Gard, T.; Holzel, B.K.; Sack, A.T.; Hempel, H.; Lazar, S.W.; Vaitl, D.; Ott, U. Pain Attenuation through Mindfulness Is Associated with Decreased Cognitive Control and Increased Sensory Processing in the Brain. Cereb. Cortex 2012, 22, 2692–2702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhaudenhuyse, A.; Boly, M.; Balteau, E.; Schnakers, C.; Moonen, G.; Luxen, A.; Lamy, M.; Degueldre, C.; Brichant, J.F.; Maquet, P.; et al. Pain and Non-Pain Processing during Hypnosis: A Thulium-YAG Event-Related FMRI Study. NeuroImage 2009, 47, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Casiglia, E.; Finatti, F.; Tikhonoff, V.; Stabile, M.R.; Mitolo, M.; Albertini, F.; Gasparotti, F.; Facco, E.; Lapenta, A.M.; Venneri, A. Mechanisms of hypnotic analgesia explained by functional magnetic resonance (fMRI). Int. J. Clin. Expl. Hypn. 2020, 68, 1–15. [Google Scholar] [CrossRef]
- Bicego, A.; Monseur, J.; Collinet, A.; Donneau, A.-F.; Fontaine, R.; Libbrecht, D.; Malaise, N.; Nyssen, A.-S.; Raaf, M.; Rousseaux, F.; et al. Complementary Treatment Comparison for Chronic Pain Management: A Randomized Longitudinal Study. PLoS ONE 2021, 16, e0256001. [Google Scholar] [CrossRef]
- Vanhaudenhuyse, A.; Gillet, A.; Malaise, N.; Salamun, I.; Grosdent, S.; Maquet, D.; Nyssen, A.-S.; Faymonville, M.-E. Psychological Interventions Influence Patients’ Attitudes and Beliefs about Their Chronic Pain. J. Tradit. Complement. Med. 2018, 8, 296–302. [Google Scholar] [CrossRef]
- Casanova, E.; Lazzari, R.E.; Lotta, S.; Mazzucchi, A. Locked-in Syndrome: Improvement in the Prognosis after an Early Intensive Multidisciplinary Rehabilitation11No Commercial Party Having a Direct Financial Interest in the Results of the Research Supporting This Article Has or Will Confer a Benefit upon the Author(s) or upon Any Organization with Which the Author(s) Is/Are Associated. Arch. Phys. Med. Rehabil. 2003, 84, 862–867. [Google Scholar] [CrossRef]
- Branco, M.P.; Pels, E.G.M.; Sars, R.H.; Aarnoutse, E.J.; Ramsey, N.F.; Vansteensel, M.J.; Nijboer, F. Brain-Computer Interfaces for Communication: Preferences of Individuals With Locked-in Syndrome. Neurorehabil. Neural Repair. 2021, 35, 267–279. [Google Scholar] [CrossRef]
- Rousseau, M.-C.; Pietra, S.; Nadji, M.; Billette de Villemeur, T. Evaluation of Quality of Life in Complete Locked-In Syndrome Patients. J. Palliat. Med. 2013, 16, 1455–1458. [Google Scholar] [CrossRef] [PubMed]
- Khalili-Ardali, M.; Wu, S.; Tonin, A.; Birbaumer, N.; Chaudhary, U. Neurophysiological Aspects of the Completely Locked-in Syndrome in Patients with Advanced Amyotrophic Lateral Sclerosis. Clin. Neurophysiol. 2021, 132, 1064–1076. [Google Scholar] [CrossRef]
- Svernling, K.; Törnbom, M.; Nordin, Å.; Sunnerhagen, K.S. Locked-in Syndrome in Sweden, an Explorative Study of Persons Who Underwent Rehabilitation: A Cohort Study. BMJ Open 2019, 9, e023185. [Google Scholar] [CrossRef] [PubMed]
- Corallo, F.; Bonanno, L.; Lo Buono, V.; De Salvo, S.; Rifici, C.; Pollicino, P.; Allone, C.; Palmeri, R.; Todaro, A.; Alagna, A.; et al. Augmentative and Alternative Communication Effects on Quality of Life in Patients with Locked-in Syndrome and Their Caregivers. J. Stroke Cerebrovasc. Dis. 2017, 26, 1929–1933. [Google Scholar] [CrossRef] [PubMed]
- Leonard, M.; Renard, F.; Harsan, L.; Pottecher, J.; Braun, M.; Schneider, F.; Froehlig, P.; Blanc, F.; Roquet, D.; Achard, S.; et al. Diffusion Tensor Imaging Reveals Diffuse White Matter Injuries in Locked-in Syndrome Patients. PLoS ONE 2019, 14, e0213528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lugo, Z.R.; Bruno, M.-A.; Gosseries, O.; Demertzi, A.; Heine, L.; Thonnard, M.; Blandin, V.; Pellas, F.; Laureys, S. Beyond the Gaze: Communicating in Chronic Locked-in Syndrome. Brain Inj. 2015, 29, 1056–1061. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Sample | Patients with Pain | Patients without Pain | p-Value 1 |
|---|---|---|---|---|
| (n = 51) | (n = 25) | (n = 26) | ||
| Sex, n (%) | 0.31 | |||
| Female | 18 (50%) | 10 (62%) | 8 (40%) | |
| Male | 18 (50%) | 6 (38%) | 12 (60%) | |
| Unknown | 15 | 9 | 6 | |
| Etiology, n (%) | 0.57 | |||
| Stroke | 41 (80%) | 21 (84%) | 20 (77%) | |
| TBI | 4 (7.8%) | 2 (8.0%) | 2 (7.7%) | |
| Infection | 2 (3.9%) | 0 (0%) | 2 (7.7%) | |
| Other | 4 (7.8%) | 2 (8.0%) | 2 (7.7%) | |
| Time since injury, Median (IQR) | 9 (6–18) | 6 (3–18) | 10 (6–16) | 0.26 |
| Tracheotomy, n (%) | 26 (51%) | 15 (29%) | 1 (22%) | 0.21 |
| Gastrostomy, n (%) | 34 (67%) | 19 (37%) | 15 (29%) | 0.17 |
| Verbal communication, n (%) | 13 (25%) | 5 (9.8%) | 8 (16%) | 0.38 |
| Use of an alphabetic code, n (%) | 35 (69%) | 19 (37%) | 16 (31%) | 0.27 |
| Own a wheelchair, n (%) | 36 (71%) | 15 (29%) | 21 (41%) | 0.1 |
| Survey completion, n (%) | ||||
| Alone | 7 (14%) | 7 (14%) | 0 (0%) | |
| With family member | 10 (20%) | 10 (20%) | 0 (0%) | |
| With healthcare | 8 (16%) | 8 (16%) | 0 (0%) | |
| No response | 26 (51%) | 0 (0%) | 26 (51%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonin, E.A.C.; Delsemme, Z.; Blandin, V.; Alnagger, N.L.; Thibaut, A.; Faymonville, M.-E.; Laureys, S.; Vanhaudenhuyse, A.; Gosseries, O. French Survey on Pain Perception and Management in Patients with Locked-In Syndrome. Diagnostics 2022, 12, 769. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030769
Bonin EAC, Delsemme Z, Blandin V, Alnagger NL, Thibaut A, Faymonville M-E, Laureys S, Vanhaudenhuyse A, Gosseries O. French Survey on Pain Perception and Management in Patients with Locked-In Syndrome. Diagnostics. 2022; 12(3):769. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030769
Chicago/Turabian StyleBonin, Estelle A. C., Zoé Delsemme, Véronique Blandin, Naji L. Alnagger, Aurore Thibaut, Marie-Elisabeth Faymonville, Steven Laureys, Audrey Vanhaudenhuyse, and Olivia Gosseries. 2022. "French Survey on Pain Perception and Management in Patients with Locked-In Syndrome" Diagnostics 12, no. 3: 769. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030769