
Remodeling Pattern of Spinal Canal after Full Endoscopic Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression: One Year Repetitive MRI and Clinical Follow-Up Evaluation

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Indication, Inclusion and Exclusion Criteria
2.2. Surgical Technique of Lumbar Endoscopic Unilateral Laminotomy with Bilateral Decompression and Interlaminar Contralateral Endoscopic Lumbar Foraminotomy
2.3. Collection of Operative, Clinical and Radiological Data
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. Combined Clinical and Radiographic Parameters of Patients Who Underwent LE-ULBD with 4 Subtypes of Postoperative MRI Canal Remodeling
3.3. Comparison of Clinical and Radiographic Parameters of Patients Who Underwent LE-ULBD with Four Subtypes of Postoperative MRI Canal Remodeling
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, M.; Kim, H.S.; Oh, S.W.; Adsul, N.M.; Singh, R.; Kashlan, O.N.; Noh, J.H.; Jang, I.T.; Oh, S.H. Evolution of Spinal Endoscopic Surgery. Neurospine 2019, 16, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Development of Endoscopic Spine Surgery for Healthy Life: To Provide Spine Care for Better, for Worse, for Richer, for Poorer, in Sickness and in Health. Neurospine 2020, 17 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. A Narrative Review of Development of Full-Endoscopic Lumbar Spine Surgery. Neurospine 2020, 17 (Suppl. 1), S20–S33. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochir. 2019, 162, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, R.; Martin, K.; Harry, M.; Georgios, G. Use of newly developed instruments and endoscopes: Full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J. Neurosurg. Spine SPI 2007, 6, 521–530. [Google Scholar]
- Drazin, D.; Ugiliweneza, B.; Al-Khouja, L.; Yang, D.; Johnson, P.; Kim, T.; Boakye, M. Treatment of Recurrent Disc Herniation: A Systematic Review. Cureus 2016, 8, e622. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Adsul, N.; Kapoor, A.; Choi, S.H.; Kim, J.H.; Kim, K.J.; Bang, J.S.; Yang, K.H.; Han, S.; Lim, J.H.; et al. A Mobile Outside-in Technique of Transforaminal Lumbar Endoscopy for Lumbar Disc Herniations. J. Vis. Exp. 2018, 138, e57999. [Google Scholar] [CrossRef] [Green Version]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: A prospective, randomized, controlled study. J. Neurosurg. Spine 2009, 10, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-S.; Wu, P.H.; Jang, I.-T. Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression Outside-In Approach: A Proctorship Guideline With 12 Steps of Effectiveness and Safety. Neurospine 2020, 17 (Suppl. 1), S99–S109. [Google Scholar] [CrossRef] [PubMed]
- Khalsa, S.S.; Kim, H.S.; Singh, R.; Kashlan, O.N. Radiographic outcomes of endoscopic decompression for lumbar spinal stenosis. Neurosurg. Focus 2019, 46, E10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.T.; Meceda, E.J.A.; Park, C.-K. Inside-Out Approach of Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression: A Detailed Technical Description, Rationale and Outcomes. Neurospine 2020, 17 (Suppl. 1), S88–S98. [Google Scholar] [CrossRef]
- Lee, C.-W.; Yoon, K.-J.; Ha, S.-S. Comparative Analysis between Three Different Lumbar Decompression Techniques (Microscopic, Tubular, and Endoscopic) in Lumbar Canal and Lateral Recess Stenosis: Preliminary Report. BioMed Res. Int. 2019, 2019, 6078469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohtori, S.; Orita, S.; Yamauchi, K.; Eguchi, Y.; Aoki, Y.; Nakamura, J.; Miyagi, M.; Suzuki, M.; Kubota, G.; Inage, K.; et al. Change of Lumbar Ligamentum Flavum after Indirect Decompression Using Anterior Lumbar Interbody Fusion. Asian Spine J. 2017, 11, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahatthanatrakul, A.; Kim, H.S.; Lin, G.X.; Kim, J.S. Decreasing thickness and remodeling of ligamentum flavum after oblique lumbar interbody fusion. Neuroradiology 2020, 62, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Clinical Results and Review of Techniques of Lumbar Endoscopic Unilateral Laminotomy with Bilateral Decompression (LE-ULBD) for Lumbar Stenosis. J. Minim. Invasive Spine Surg. Tech. 2021, 6 (Suppl. 1), S117–S122. [Google Scholar] [CrossRef]
- Kim, H.S.; Wu, P.H.; Raorane, H.D.; Heo, D.H.; Lee, Y.J.; Yang, K.-H.; Jang, I.-T. Endoscopic Resection of Symptomatic Degenerative Repetitive Stress Related Fracture of the Tip of Superior Articular Process. An Unusual Cause of Severe Back Pain: Report of 2 Cases and Technical Note. J. Minim. Invasive Spine Surg. Tech. 2020, 5, 36–41. [Google Scholar] [CrossRef]
- Kim, H.S.; Patel, R.; Paudel, B.; Jang, I.-T.; Jang, J.-S.; Oh, S.-H.; Park, J.E.; Lee, S. Early Outcomes of Endoscopic Contralateral Foraminal and Lateral Recess Decompression via an Interlaminar Approach in Patients with Unilateral Radiculopathy from Unilateral Foraminal Stenosis. World Neurosurg. 2017, 108, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, J.Y.; Wu, P.H.; Jang, I.-T. Effect of Dorsal Root Ganglion Retraction in Endoscopic Lumbar Decompressive Surgery for Foraminal Pathology: A Retrospective Cohort Study of Interlaminar Contralateral Endoscopic Lumbar Foraminotomy and Discectomy versus Transforaminal Endoscopic Lumbar Foraminotomy and Discectomy. World Neurosurg. 2021, 148, e101–e114. [Google Scholar] [PubMed]
- Kim, H.S.; Raorane, H.D.; Wu, P.H.; Heo, D.H.; Sharma, S.B.; Jang, I.T. Incidental Durotomy During Endoscopic Stenosis Lumbar Decompression: Incidence, Classification, and Proposed Management Strategies. World Neurosurg. 2020, 139, e13–e22. [Google Scholar] [CrossRef]
- Kim, H.S.; Raorane, H.D.; Wu, P.H.; Heo, D.H.; Yi, Y.J.; Yang, K.-H.; Jang, I.-T. Feasibility of Endoscopic Transforaminal Lumbar Interbody Fusion (eTLIF) Through the Posterior Paraspinal Approach: Technical Note and Preliminary Result. J. Minim. Invasive Spine Surg. Tech. 2021, 6, 35–41. [Google Scholar] [CrossRef]
- Kim, H.-S.; Wu, P.H.; Lee, Y.J.; Kim, D.H.; Jang, I.T. Technical Considerations of Uniportal Endoscopic Posterolateral Lumbar Interbody Fusion: A Review of Its Early Clinical Results in Application in Adult Degenerative Scoliosis. World Neurosurg. 2020, 145, 682–692. [Google Scholar] [CrossRef]
- Kim, H.-S.; Wu, P.-H.; An, J.-W.; Lee, Y.-J.; Lee, J.-H.; Kim, M.-H.; Lee, I.; Park, J.-S.; Lee, J.-H.; Park, J.-H.; et al. Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note. Brain Sci. 2021, 11, 1169. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.-U.; De Carvalho, P.S.T.; De Carvalho, P.; Yeung, A. Minimal Clinically Important Difference in Patient-Reported Outcome Measures with the Transforaminal Endoscopic Decompression for Lateral Recess and Foraminal Stenosis. Int. J. Spine Surg. 2020, 14, 254–266. [Google Scholar] [CrossRef]
- McGrath, L.B.; White-Dzuro, G.A.; Hofstetter, C.P. Comparison of clinical outcomes following minimally invasive or lumbar endoscopic unilateral laminotomy for bilateral decompression. J. Neurosurg. Spine 2019, 30, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, T.; Tanaka, N.; Kim, J.; Okada, M.; Ochi, M.; Hutton, W.C. Biomechanical assessment of minimally invasive decompression for lumbar spinal canal stenosis: A cadaver study. J. Spinal Disord. Tech. 2009, 22, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.T.; Nam, H.G.W.; Kim, S.B.; Kim, H.S.; Park, J.S.; Park, C.K. Therapeutic Feasibility of Full Endoscopic Decompression in One- to Three-Level Lumbar Canal Stenosis via a Single Skin Port Using a New Endoscopic System, Percutaneous Stenoscopic Lumbar Decompression. Asian Spine J. 2019, 13, 272–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Choi, M.; Ryu, D.S.; Choi, I.; Kim, C.H.; Kim, H.S.; Sohn, M.J. Efficacy and Safety of Full-endoscopic Decompression via Interlaminar Approach for Central or Lateral Recess Spinal Stenosis of the Lumbar Spine: A Meta-analysis. Spine 2018, 43, 1756–1764. [Google Scholar] [CrossRef]
- Dewanngan, N.K.; Yadav, Y.R.; Parihar, V.S.; Ratre, S.; Kher, Y.; Bhatele, P. Extent of Decompression of Lumbar Spinal Canal after Endoscopic Surgery. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2017, 78, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Carrascosa-Granada, A.; Velazquez, W.; Wagner, R.; Saab Mazzei, A.; Vargas-Jimenez, A.; Jorquera, M.; Albacar, J.A.B.; Sallabanda, K. Comparative Study Between Uniportal Full-Endoscopic Interlaminar and Tubular Approach in the Treatment of Lumbar Spinal Stenosis: A Pilot Study. Glob. Spine J. 2020, 10 (Suppl. 2), 70s–80s. [Google Scholar] [CrossRef]
- Ishimoto, Y.; Yoshimura, N.; Muraki, S.; Yamada, H.; Nagata, K.; Hashizume, H.; Takiguchi, N.; Minamide, A.; Oka, H.; Kawaguchi, H.; et al. Associations between radiographic lumbar spinal stenosis and clinical symptoms in the general population: The Wakayama Spine Study. Osteoarthr. Cartil. 2013, 21, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Kuittinen, P.; Sipola, P.; Saari, T.; Aalto, T.J.; Sinikallio, S.; Savolainen, S.; Kröger, H.; Turunen, V.; Leinonen, V.; Airaksinen, O. Visually assessed severity of lumbar spinal canal stenosis is paradoxically associated with leg pain and objective walking ability. BMC Musculoskelet. Disord. 2014, 15, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.H.; Kim, H.S.; Lee, Y.J.; Kim, D.H.; Lee, J.H.; Jeon, J.B.; Raorane, H.D.; Jang, I.T. Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion with Endoscopic Disc Drilling Preparation Technique for Symptomatic Foraminal Stenosis Secondary to Severe Collapsed Disc Space: A Clinical and Computer Tomographic Study with Technical Note. Brain Sci. 2020, 10, 373. [Google Scholar]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Technical note on Uniportal full endoscopic posterolateral approach transforaminal lumbar interbody fusion with reduction for grade 2 spondylolisthesis. Interdiscip. Neurosurg. 2020, 21, 100712. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. Uniportal Endoscopic Lateral to Medial Direction Transforaminal Lumbar Interbody Fusion: A Case Report and Technical Guide for Navigating Through Landmarks in Left Lumbar 4/5 Post Laminotomy Revision Lumbar Fusion Surgery. J. Minim. Invasive Spine Surg. Tech. 2021, 6, 66–73. [Google Scholar] [CrossRef]
- Lee, C.-W.; Yoon, K.-J.; Kim, S.-W. Percutaneous Endoscopic Decompression in Lumbar Canal and Lateral Recess Stenosis—The Surgical Learning Curve. Neurospine 2019, 16, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H. Early Career Challenges in Setting Up an Endoscopic Spine Surgery Practice. World Neurosurg. 2020, 144, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Kim, H.S.; Choi, D.J.; Gamaliel, Y.-H.T. Overview of Tips in Overcoming Learning Curve in Uniportal and Biportal Endoscopic Spine Surgery. J. Minim. Invasive Spine Surg. Tech. 2021, 6 (Suppl. 1), S84–S96. [Google Scholar] [CrossRef]
- Heo, D.H.; Lee, D.C.; Park, C.K. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: Biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurg. Focus 2019, 46, E9. [Google Scholar] [CrossRef] [Green Version]
- Heo, D.H.; Hong, Y.H.; Lee, D.C.; Chung, H.J.; Park, C.K. Technique of Biportal Endoscopic Transforaminal Lumbar Interbody Fusion. Neurospine 2020, 17 (Suppl. 1), S129–S137. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Description | Postoperative Day 1 Spinal Canal Area mm2 | Postoperative 6 Months Spinal Canal Area mm2 | Postoperative 1 Year Spinal Canal Area mm2 |
|---|---|---|---|---|
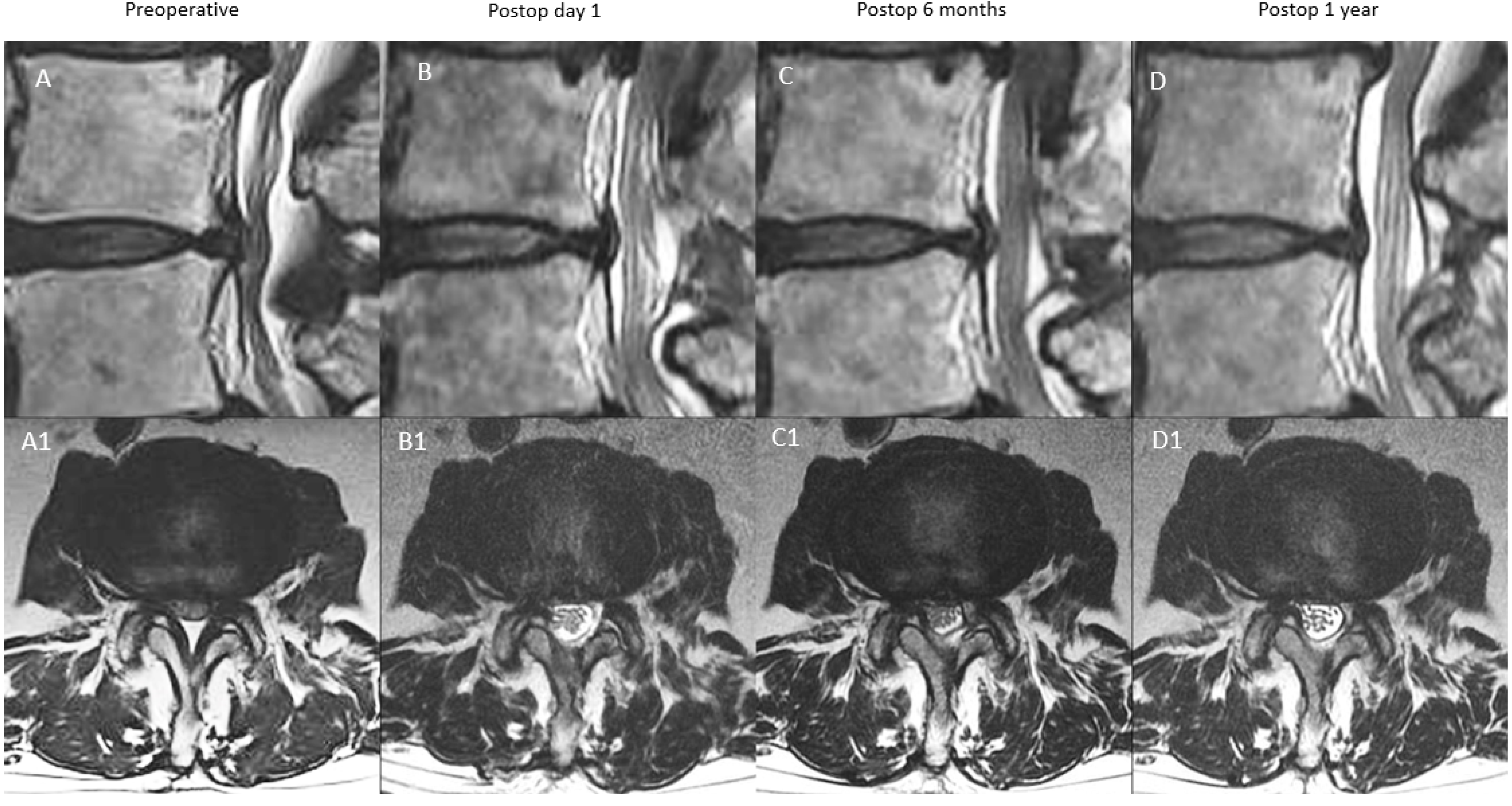
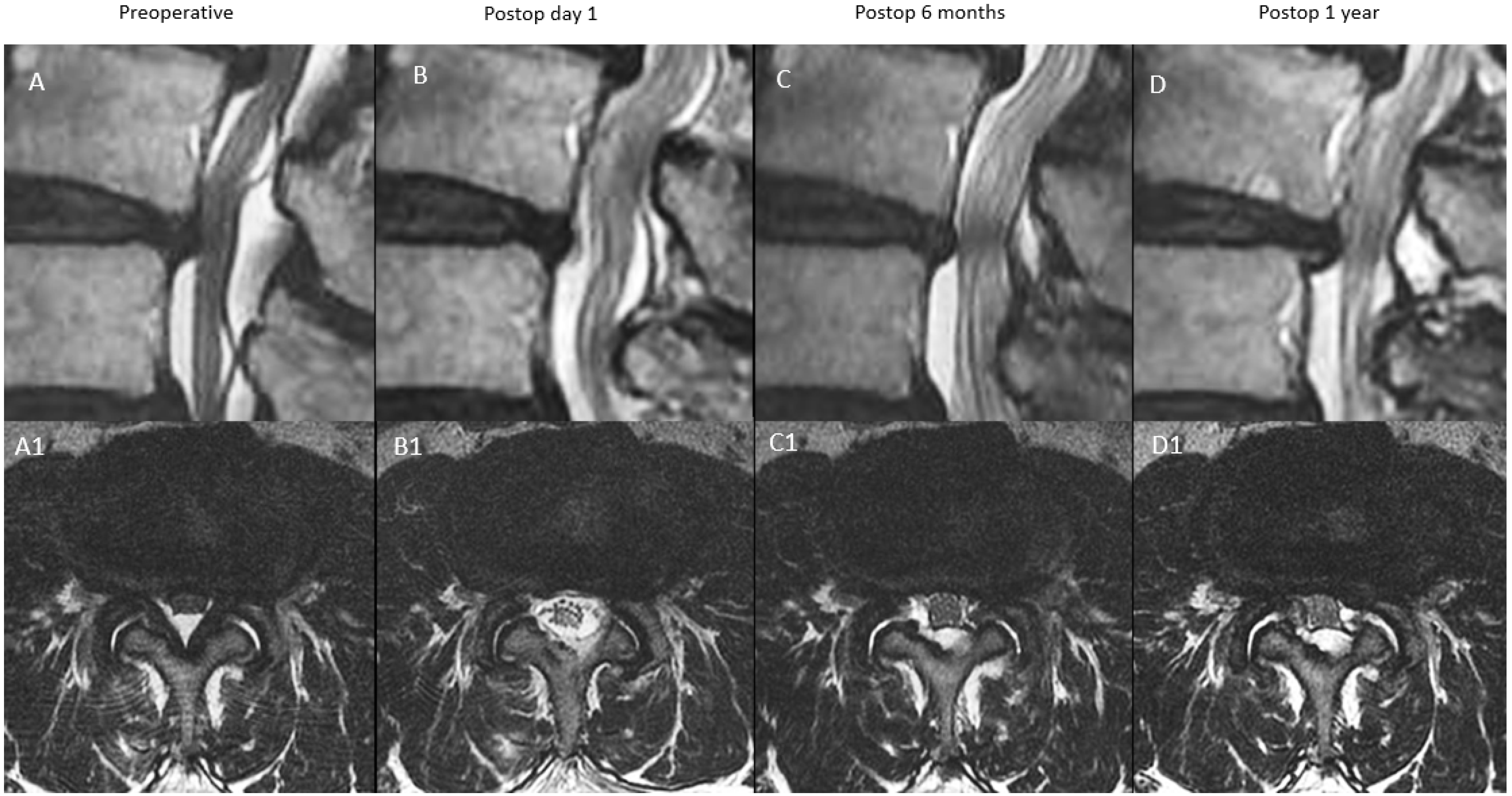
| A: Continuous Type | There is significant decompression with increased spinal canal area on postoperative day one, a modest drop at postoperative 6 months and close to postoperative 6 months value at postoperative one year | X | ≥70% X | 70–90% X (close to postoperative six months value) |
| B: Remodelling Type | There is significant decompression with increased spinal canal area on postoperative day one, a significant drop at postoperative 6 months and modest improvement at one year but less than 90% of the postoperative day one spinal canal area | X | <70% X | 70–90% X |
| C: Expansion Type | There is significant decompression with increased spinal canal area on postoperative day one, a modest drop at postoperative 6 months and significant improvement at one year with more than 90% of the postoperative day one spinal canal area | X | ≥70% X | 90–100% X |
| D: Restenosis Type | There is significant decompression with increased spinal canal area on postoperative day one, a significant drop at postoperative 6 months and minimal improvement at one year with <70% of the postoperative day one spinal canal area | X | <70% X | <70% X |
| Type A | Type B | Type C | Type D | Combined | p Value | |
|---|---|---|---|---|---|---|
| Number of patients | 32 | 53 | 30 | 11 | 126 | N/A |
| Number of Patients with Level Lumbar Two Three | 2 | 5 | 2 | 3 | 12 | N/A |
| Number of Patients with Level Lumbar Three Four | 6 | 14 | 9 | 3 | 32 | N/A |
| Number of Patients with Level Lumbar Four Five | 13 | 30 | 14 | 3 | 60 | N/A |
| Number of Patients with Level Lumbar Five Sacral One | 11 | 3 | 4 | 2 | 20 | N/A |
| Age (mean, range in years) | 59.41 (21–80) | 67.60 (28–83) | 60.33 (21–86) | 67.18 (57–78) | 63.75 (21–86) | 0.007 |
| F/U Period (mean, range in years) | 26.53 (17–37) | 28.13 (18–36) | 26.77 (17–35) | 29.81 (26–38) | 27.55 (17–38) | 0.184 |
| Male:Female Ratio | 10:22 | 28:25 | 12:18 | 5:6 | 55:71 | 0.262 |
| Complication Rate | 0.00 | 13.21 | 10.00 | 45.45 | 11.90 | 0.001 |
| Revision Surgery | 2 | 1 | 1 | 2 | 6 | 0.219 |
| Preoperative MRI Measurement Area in Upper End Plate (mean, SD) mm2 | 97.39 ± 41.26 | 76.40 ± 24.58 | 95.18 ± 38.71 | 65.47 ± 17.98 | 85.25 ± 34.29 | 0.003 |
| Postoperative Day 1 MRI Measurement in Upper End Plate (mean, SD) mm2 | 136.55 ± 47.18 | 123.82 ± 24.79 | 146.63 ± 48.31 | 114.57 ± 21.10 | 131.68 ± 38.68 | 0.023 |
| Postoperative 6 months MRI Measurement Area in Upper End Plate (mean, SD) mm2 | 126.33 ± 48.14 | 108.46 ± 23.30 | 135.78 ± 45.70 | 92.77 ± 17.03 | 118.14 ± 38.69 | <0.001 |
| Postoperative One Year In Upper End Plate MRI Measurement Area (mean, SD) mm2 | 125.38 ± 39.54 | 118.79 ± 24.77 | 144.67 ± 47.42 | 103.64 ± 14.75 | 125.30 ± 36.49 | 0.002 |
| Preoperative MRI Measurement Area in Mid Disc (mean, SD) mm2 | 82.36 ± 35.18 | 56.82 ± 19.57 | 84.00 ± 48.86 | 45.31 ± 17.04 | 68.77 ± 35.43 | <0.001 |
| Postoperative Day 1 MRI Measurement in Mid Disc (mean, SD) mm2 | 137.52 ± 46.68 | 129.65 ± 25.80 | 150.85 ± 53.20 | 116.96 ± 24.01 | 135.59 ± 40.28 | 0.047 |
| Postoperative 6 months MRI Measurement Area in Mid Disc (mean, SD) mm2 | 129.59 ± 43.70 | 106.61 ± 24.99 | 138.92 ± 50.36 | 86.86 ± 22.64 | 115.88 ± 40.05 | <0.001 |
| Postoperative One Year in Mid Disc (mean, SD) mm2 | 127.21 ± 44.98 | 119.76 ± 27.53 | 148.33 ± 54.54 | 95.15 ± 21.74 | 126.31 ± 42.01 | 0.001 |
| Preoperative MRI Measurement Area in Lower Endplate (mean, SD) mm2 | 93.72 ± 37.69 | 72.65 ± 30.87 | 92.68 ± 44.50 | 65.43 ± 28.73 | 82.14 ± 37.39 | 0.010 |
| Postoperative Day 1 MRI Measurement in Lower Endplate (mean, SD) mm2 | 143.61 ± 46.06 | 136.28 ± 31.51 | 151.18 ± 51.79 | 146.86 ± 37.31 | 142.61 ± 41.35 | 0.451 |
| Postoperative 6 months MRI Measurement Area in Lower Endplate (mean, SD) mm2 | 134.52 ± 44.08 | 125.41 ± 28.61 | 146.6 ± 50.37 | 125.13 ± 36.53 | 132.74 ± 39.91 | 0.117 |
| Postoperative One Year in Lower Endplate (mean, SD) mm2 | 134.76 ± 45.27 | 127.36 ± 32.34 | 148.00 ± 49.34 | 123.83 ± 33.56 | 133.85 ± 40.90 | 0.132 |
| Preoperative VAS (mean, SD) | 7.66 ± 1.18 | 7.74 ± 1.35 | 7.30 ± 1.49 | 7.73 ± 1.19 | 7.61 ± 1.33 | 0.529 |
| Postoperative VAS at 1 week(mean, SD) | 3.00 ± 0.51 | 3.11 ± 0.51 | 3.10 ± 0.76 | 3.09 ± 0.54 | 3.08 ± 0.57 | 0.844 |
| Postoperative VAS at 3 months(mean, SD) | 2.06 ± 0.80 | 2.15 ± 0.84 | 2.17 ± 0.87 | 2.45 ± 0.82 | 2.39 ± 0.78 | 0.899 |
| Postoperative VAS at final follow-up(mean, SD) | 134.76 ± 45.27 | 127.36 ± 32.34 | 148.00 ± 49.34 | 123.83 ± 33.56 | 2.16 ± 0.83 | 0.616 |
| Preoperative ODI(mean, SD) | 73.75 ± 8.62 | 74.57 ± 9.58 | 70.93 ± 9.79 | 74.73 ± 7.55 | 73.51 ± 9.25 | 0.361 |
| Postoperative ODI at 1 week(mean, SD) | 30.31 ± 4.22 | 30.38 ± 4.42 | 31.60 ± 7.11 | 31.27 ± 5.00 | 30.73 ± 5.16 | 0.703 |
| Postoperative ODI at 3 months (mean, SD) | 26.88 ± 5.28 | 26.42 ± 4.66 | 27.07 ± 6.53 | 26.55 ± 4.30 | 26.70 ± 5.24 | 0.952 |
| Postoperative ODI at final follow-up(mean, SD) | 24.56 ± 4.85 | 24.57 ± 5.09 | 25.33 ± 6.31 | 25.45 ± 4.66 | 24.83 ± 5.27 | 0.889 |
| Percentage MacNab Good To Excellent Outcome(%) | 96.88 | 96.23 | 96.67 | 90.91 | 96.03 | 0.837 |
| Combined Data LE-ULBD Type A to D | Mean | Std. Deviation | p Value |
|---|---|---|---|
| VAS improvement at 1 weeks | 4.53 | 1.35 | <0.001 |
| VAS improvement at 3 months | 5.22 | 1.53 | <0.001 |
| VAS improvement at final follow-up | 5.45 | 1.67 | <0.001 |
| ODI improvement at 1 weeks | 42.78 | 10.00 | <0.001 |
| ODI improvement at 3 months | 46.81 | 10.25 | <0.001 |
| ODI improvement at final follow-up | 48.68 | 10.80 | <0.001 |
| Increment of day 1 postoperative MRI spinal canal in upper end plate (mean, SD) mm2 | 46.43 | 20.35 | <0.001 |
| Increment of 6 months postoperative MRI spinal canal area in upper end plate (mean, SD) mm2 | 32.89 | 19.75 | <0.001 |
| Increment of one year postoperative MRI spinal canal area in upper end plate (mean, SD) mm2 | 40.05 | 27.80 | <0.001 |
| Increment of day 1 postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 66.82 | 27.85 | <0.001 |
| Increment of 6 months postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 47.10 | 25.37 | <0.001 |
| Increment of one year postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 57.53 | 27.04 | <0.001 |
| Increment of day 1 postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 60.47 | 27.58 | <0.001 |
| Increment of 6 months postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 50.61 | 24.64 | <0.001 |
| Increment of one year postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 51.71 | 25.12 | <0.001 |
| Group Charateristics | Type A | Type B | Type C | Type D | p Value |
|---|---|---|---|---|---|
| Improvement of VAS at 1 week | 4.66 ± 1.26 | 4.62 ± 1.40 | 4.20 ± 1.27 | 4.64 ± 1.57 | 0.499 |
| Improvement of VAS at 3 months | 5.28 ± 1.37 | 5.40 ± 1.61 | 4.83 ± 1.56 | 5.27 ± 1.49 | 0.446 |
| Improvement of VAS at final FU | 5.59 ± 1.58 | 5.58 ± 1.71 | 5.13 ± 1.72 | 5.27 ± 1.68 | 0.624 |
| Improvement of ODI at 1 week | 43.44 ± 9.16 | 44.19 ± 10.36 | 39.33 ± 9.21 | 43.45 ± 11.80 | 0.187 |
| Improvement of ODI at 3 months | 46.88 ± 9.85 | 48.15 ± 10.83 | 43.87 ± 9.92 | 48.18 ± 8.92 | 0.313 |
| Improvement of ODI at final FU | 49.19 ± 10.51 | 50.00 ± 11.29 | 45.60 ± 10.58 | 49.27 ± 9.39 | 0.346 |
| Increment of day 1 postoperative MRI spinal canal in upper end plate (mean, SD) mm2 | 39.16 ± 22.73 | 47.42 ± 18.77 | 51.45 ± 18.16 | 49.10 ± 23.05 | 0.010 |
| Increment of 6 months postoperative MRI spinal canal area in upper end plate (mean, SD) mm2 | 28.95 ± 22.14 | 32.06 ± 19.40 | 40.60 ± 16.93 | 27.30 ± 17.43 | 0.076 |
| Increment of one year postoperative MRI spinal canal area in upper end plate (mean, SD) mm2 | 28.00 ± 42.57 | 42.38 ± 19.29 | 49.49 ± 18.41 | 38.18 ± 18.94 | 0.018 |
| Increment of day 1 postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 55.16 ± 27.51 | 72.83 ± 23.87 | 66.85 ± 34.48 | 71.65 ± 16.87 | 0.036 |
| Increment of 6 months postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 47.23 ± 25.88 | 49.79 ± 21.93 | 54.92 ± 30.70 | 41.55 ± 12.92 | 0.030 |
| Increment of one year postoperative MRI spinal canal area in mid disc (mean, SD) mm2 | 44.86 ± 25.73 | 62.94 ± 24.43 | 64.33 ± 31.82 | 49.83 ± 13.31 | 0.006 |
| Increment of day 1 postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 49.89 ± 34.50 | 63.63 ± 23.70 | 58.50 ± 24.27 | 81.43 ± 16.81 | 0.007 |
| Increment of 6 months postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 40.80 ± 29.35 | 52.76 ± 22.70 | 53.92 ± 22.18 | 59.70 ± 18.80 | 0.055 |
| Increment of one year postoperative MRI spinal canal area in lower end plate (mean, SD) mm2 | 41.04 ± 28.56 | 54.72 ± 24.29 | 55.32 ± 22.49 | 58.40 ± 18.05 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-S.; Wu, P.-H.; Grasso, G.; An, J.-W.; Kim, M.; Lee, I.; Park, J.-S.; Lee, J.-H.; Kang, S.; Lee, J.; et al. Remodeling Pattern of Spinal Canal after Full Endoscopic Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression: One Year Repetitive MRI and Clinical Follow-Up Evaluation. Diagnostics 2022, 12, 793. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040793
Kim H-S, Wu P-H, Grasso G, An J-W, Kim M, Lee I, Park J-S, Lee J-H, Kang S, Lee J, et al. Remodeling Pattern of Spinal Canal after Full Endoscopic Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression: One Year Repetitive MRI and Clinical Follow-Up Evaluation. Diagnostics. 2022; 12(4):793. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040793
Chicago/Turabian StyleKim, Hyeun-Sung, Pang-Hung Wu, Giovanni Grasso, Jin-Woo An, Myeonghun Kim, Inkyung Lee, Jong-Seon Park, Jun-Hyoung Lee, Sangsoo Kang, Jeongshik Lee, and et al. 2022. "Remodeling Pattern of Spinal Canal after Full Endoscopic Uniportal Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression: One Year Repetitive MRI and Clinical Follow-Up Evaluation" Diagnostics 12, no. 4: 793. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040793