
Endometrium as Control of Endometriosis in Experimental Research: Assessment of Sample Suitability


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Data
2.2. Grouping of Histopathological Diagnoses
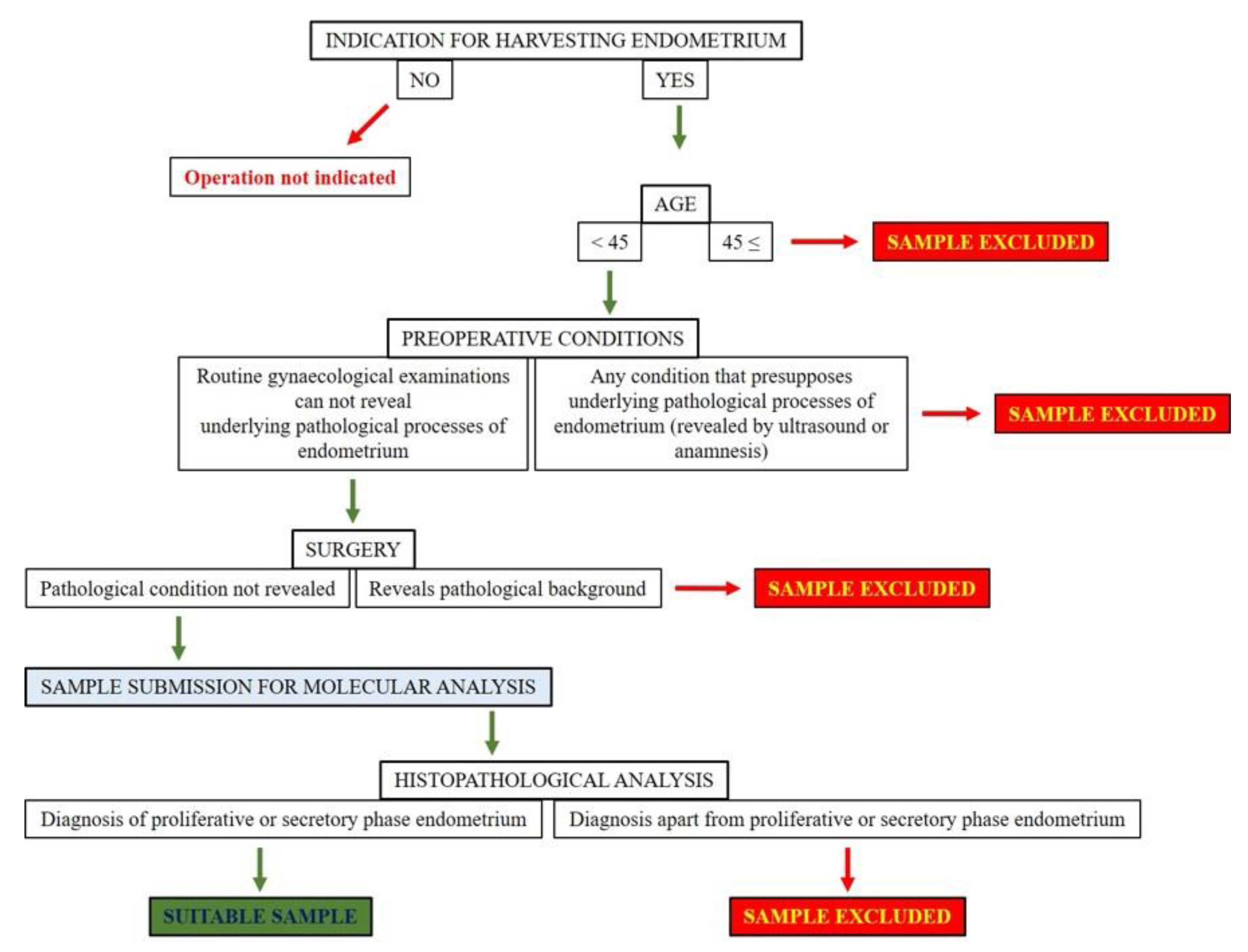
2.3. Using Clinical Exclusion Criteria
2.4. Using Clinical Selection Criteria
2.5. Using Histopathological Selection and Exclusion Criteria
2.6. Tissue Culturing
2.7. Hormone Application
2.8. H&E Staining
2.9. Mathematical Analysis
2.10. Ethical Approval
3. Results
3.1. Histopathological Findings of the Samples
3.2. Histopathological Findings of Endometrial Scraping and Biopsy Procedures
3.3. Histopathological Findings of Endometrial Scraping Procedures (D&C)
3.4. Histopathological Findings of Hysteroscopy with Endometrial Biopsy Procedures (HSC)
3.5. Clinically Suitable Samples for In Vitro Experimental Research Extracted by Scraping and Hysteroscopy with Endometrial Biopsy Procedures
3.6. Clinically Suitable Samples for In Vitro Experimental Research Extracted by Scraping Procedures (D&C)
3.7. Clinically Suitable Samples for In Vitro Experimental Research Extracted by Hysteroscopy with Endometrial Biopsy Procedures (HSC)
3.8. Suitable Samples for Further In Vitro Experimental Research Studies
3.9. Experiences Obtained from the Submitted and Cultured Eutopic Endometrial Tissues
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hsu, A.L.; Khachikyan, I.; Stratton, P. Invasive and noninvasive methods for the diagnosis of endometriosis. Clin. Obstet. Gynecol. 2010, 53, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Rolla, E. Endometriosis: Advances and controversies in classification, pathogenesis, diagnosis, and treatment. F1000Res 2019, 8, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagana, A.S.; Vitale, S.G.; Salmeri, F.M.; Triolo, O.; Ban Frangez, H.; Vrtacnik-Bokal, E.; Stojanovska, L.; Apostolopoulos, V.; Granese, R.; Sofo, V. Unus pro omnibus, omnes pro uno: A novel, evidence-based, unifying theory for the pathogenesis of endometriosis. Med. Hypotheses 2017, 103, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.H.; Au, H.K.; Lee, W.C.; Chi, C.C.; Ling, T.Y.; Wang, L.M.; Kao, S.H.; Huang, Y.H.; Tzeng, C.R. Expression of the pluripotent transcription factor OCT4 promotes cell migration in endometriosis. Fertil. Steril. 2013, 99, 1332–1339.e5. [Google Scholar] [CrossRef] [PubMed]
- Lagana, A.S.; Salmeri, F.M.; Vitale, S.G.; Triolo, O.; Gotte, M. Stem cell trafficking during endometriosis: May epigenetics play a pivotal role? Reprod. Sci. 2018, 25, 978–979. [Google Scholar] [CrossRef] [PubMed]
- Macer, M.L.; Taylor, H.S. Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 535–549. [Google Scholar] [CrossRef] [Green Version]
- Bouquet De Joliniere, J.; Ayoubi, J.M.; Gianaroli, L.; Dubuisson, J.B.; Gogusev, J.; Feki, A. Endometriosis: A new cellular and molecular genetic approach for understanding the pathogenesis and evolutivity. Front. Surg. 2014, 1, 16. [Google Scholar] [CrossRef] [Green Version]
- Lagana, A.S.; Garzon, S.; Gotte, M.; Vigano, P.; Franchi, M.; Ghezzi, F.; Martin, D.C. The pathogenesis of endometriosis: Molecular and cell biology insights. Int. J. Mol. Sci. 2019, 20, 5615. [Google Scholar] [CrossRef] [Green Version]
- Maclean, A.; Kamal, A.; Adishesh, M.; Alnafakh, R.; Tempest, N.; Hapangama, D.K. Human uterine biopsy: Research value and common pitfalls. Int. J. Reprod. Med. 2020, 2020, 9275360. [Google Scholar] [CrossRef]
- Sourial, S.; Tempest, N.; Hapangama, D.K. Theories on the pathogenesis of endometriosis. Int. J. Reprod. Med. 2014, 2014, 179515. [Google Scholar] [CrossRef] [Green Version]
- Borghese, B.; Mondon, F.; Noel, J.C.; Fayt, I.; Mignot, T.M.; Vaiman, D.; Chapron, C. Gene expression profile for ectopic versus eutopic endometrium provides new insights into endometriosis oncogenic potential. Mol. Endocrinol. 2008, 22, 2557–2562. [Google Scholar] [CrossRef]
- Gabriel, M.; Fey, V.; Heinosalo, T.; Adhikari, P.; Rytkonen, K.; Komulainen, T.; Huhtinen, K.; Laajala, T.D.; Siitari, H.; Virkki, A.; et al. A relational database to identify differentially expressed genes in the endometrium and endometriosis lesions. Sci. Data 2020, 7, 284. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Salamonsen, L.A.; Winship, A.; Menkhorst, E.; Nie, G.; Gargett, C.E.; Dimitriadis, E. Fertile ground: Human endometrial programming and lessons in health and disease. Nat. Rev. Endocrinol. 2016, 12, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Gargett, C.E.; Schwab, K.E.; Zillwood, R.M.; Nguyen, H.P.; Wu, D. Isolation and culture of epithelial progenitors and mesenchymal stem cells from human endometrium. Biol. Reprod. 2009, 80, 1136–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cousins, F.L.; Dorien, F.O.; Gargett, C.E. Endometrial stem/progenitor cells and their role in the pathogenesis of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, T. Endometrial stem/progenitor cells. J. Obstet. Gynaecol. Res. 2014, 40, 2015–2022. [Google Scholar] [CrossRef]
- Gibson, D.A.; Simitsidellis, I.; Collins, F.; Saunders, P.T.K. Endometrial intracrinology: Oestrogens, androgens and endometrial disorders. Int. J. Mol. Sci. 2018, 19, 3276. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Yuan, Q.; Qu, Y.; Zhou, Y.; Bei, J. Endometrial mesenchymal stem cells isolated from menstrual blood by adherence. Stem Cells Int. 2016, 2016, 3573846. [Google Scholar] [CrossRef]
- Musina, R.A.; Belyavski, A.V.; Tarusova, O.V.; Solovyova, E.V.; Sukhikh, G.T. Endometrial mesenchymal stem cells isolated from the menstrual blood. Bull. Exp. Biol. Med. 2008, 145, 539–543. [Google Scholar] [CrossRef]
- Nikolakopoulou, K.; Turco, M.Y. Investigation of infertility using endometrial organoids. Reproduction 2021, 161, R113–R127. [Google Scholar] [CrossRef]
- Noumoff, J.; Haydock, S.W.; Sachdeva, R.; Heyner, S.; Pritchard, M.L. Characteristics of cell lines derived from normal and malignant endometrial tissue. Gynecol. Oncol. 1987, 27, 141–149. [Google Scholar] [CrossRef]
- Holdsworth-Carson, S.J.; Colgrave, E.M.; Donoghue, J.F.; Fung, J.N.; Churchill, M.L.; Mortlock, S.; Paiva, P.; Healey, M.; Montgomery, G.W.; Girling, J.E.; et al. Generation of immortalized human endometrial stromal cell lines with different endometriosis risk genotypes. Mol. Hum. Reprod. 2019, 25, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Fan, H. In-vitro models of human endometriosis. Exp. Ther. Med. 2020, 19, 1617–1625. [Google Scholar] [PubMed]
- Ajayi, A.F.; Akhigbe, R.E. Staging of the estrous cycle and induction of estrus in experimental rodents: An update. Fertil. Res. Pract. 2020, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Sato, J.; Nasu, M.; Tsuchitani, M. Comparative histopathology of the estrous or menstrual cycle in laboratory animals. J. Toxicol. Pathol. 2016, 29, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Simitsidellis, I.; Gibson, D.A.; Saunders, P.T.K. Animal models of endometriosis: Replicating the aetiology and symptoms of the human disorder. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Grummer, R. Animal models in endometriosis research. Hum. Reprod. Update 2006, 12, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Story, L.; Kennedy, S. Animal studies in endometriosis: A review. ILAR J. 2004, 45, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, F.; Wibisono, H.; Mon Khine, Y.; Harada, T. Animal models for research on endometriosis. Front. Biosci. 2021, 13, 37–53. [Google Scholar]
- Tirado-Gonzalez, I.; Barrientos, G.; Tariverdian, N.; Arck, P.C.; Garcia, M.G.; Klapp, B.F.; Blois, S.M. Endometriosis research: Animal models for the study of a complex disease. J. Reprod. Immunol. 2010, 86, 141–147. [Google Scholar] [CrossRef]
- Critchley, H.O.D.; Maybin, J.A.; Armstrong, G.M.; Williams, A.R.W. Physiology of the endometrium and regulation of menstruation. Physiol. Rev. 2020, 100, 1149–1179. [Google Scholar] [CrossRef] [PubMed]
- Simitsidellis, I.; Saunders, P.T.K.; Gibson, D.A. Androgens and endometrium: New insights and new targets. Mol. Cell Endocrinol. 2018, 465, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.A.; Simitsidellis, I.; Collins, F.; Saunders, P.T.K. Androgens, oestrogens and endometrium: A fine balance between perfection and pathology. J. Endocrinol. 2020, 246, R75–R93. [Google Scholar] [CrossRef] [PubMed]
- Tempest, N.; Jansen, M.; Baker, A.M.; Hill, C.J.; Hale, M.; Magee, D.; Treanor, D.; Wright, N.A.; Hapangama, D.K. Histological 3D reconstruction and in vivo lineage tracing of the human endometrium. J. Pathol. 2020, 251, 440–451. [Google Scholar] [CrossRef]
- Proestling, K.; Birner, P.; Balendran, S.; Nirtl, N.; Marton, E.; Yerlikaya, G.; Kuessel, L.; Reischer, T.; Wenzl, R.; Streubel, B.; et al. Enhanced expression of the stemness-related factors OCT4, SOX15 and TWIST1 in ectopic endometrium of endometriosis patients. Reprod. Biol. Endocrinol. 2016, 14, 81. [Google Scholar] [CrossRef] [Green Version]
- McCluggage, W.G. My approach to the interpretation of endometrial biopsies and curettings. J. Clin. Pathol. 2006, 59, 801–812. [Google Scholar] [CrossRef]
- Lax, S.F. Molecular genetic changes in epithelial, stromal and mixed neoplasms of the endometrium. Pathology 2007, 39, 46–54. [Google Scholar] [CrossRef]
- Llobet, D.; Pallares, J.; Yeramian, A.; Santacana, M.; Eritja, N.; Velasco, A.; Dolcet, X.; Matias-Guiu, X. Molecular pathology of endometrial carcinoma: Practical aspects from the diagnostic and therapeutic viewpoints. J. Clin. Pathol. 2009, 62, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Yeramian, A.; Moreno-Bueno, G.; Dolcet, X.; Catasus, L.; Abal, M.; Colas, E.; Reventos, J.; Palacios, J.; Prat, J.; Matias-Guiu, X. Endometrial carcinoma: Molecular alterations involved in tumor development and progression. Oncogene 2013, 32, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Zauber, P.; Denehy, T.R.; Taylor, R.R.; Ongcapin, E.H.; Marotta, S.; Sabbath-Solitare, M. Strong correlation between molecular changes in endometrial carcinomas and concomitant hyperplasia. Int. J. Gynecol. Cancer 2015, 25, 863–868. [Google Scholar] [CrossRef]
- Erikson, D.W.; Barragan, F.; Piltonen, T.T.; Chen, J.C.; Balayan, S.; Irwin, J.C.; Giudice, L.C. Stromal fibroblasts from perimenopausal endometrium exhibit a different transcriptome than those from the premenopausal endometrium. Biol. Reprod. 2017, 97, 387–399. [Google Scholar] [CrossRef] [Green Version]
- Shuster, L.T.; Rhodes, D.J.; Gostout, B.S.; Grossardt, B.R.; Rocca, W.A. Premature menopause or early menopause: Long-term health consequences. Maturitas 2010, 65, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inal, Z.O.; Inal, H.A.; Kucukosmanoglu, I.; Kucukkendirci, H. Assessment of endometrial sampling and histopathological results: Analysis of 4247 cases. Eurasian J. Med. 2017, 49, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Brannstrom, M. Uterus transplantation and beyond. J. Mater. Sci. Mater. Med. 2017, 28, 70. [Google Scholar] [CrossRef] [PubMed]
- Bull, J.R.; Rowland, S.P.; Scherwitzl, E.B.; Scherwitzl, R.; Danielsson, K.G.; Harper, J. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. NPJ Digit. Med. 2019, 2, 83. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Groups | Histopathological Diagnoses |
|---|---|
| Proliferative phase endometrium | - Proliferative phase endometrium |
| Secretory phase endometrium | - Secretory phase endometrium |
| Menstrual phase endometrium | - Menstrual phase endometrium |
| Exogenous hormones | - Pseudo-decidualization - Effects of gestagens |
| Menopausal endometrium | - Pseudo-menopausal endometrium - Endometrial atrophy |
| Inadequate for analysis | - Desquamated endometrium - Inadequate sample - Submucosal uterine leiomyoma |
| Endometrial polyp | - Endometrial polyp |
| Endometrial hyperplasia | - Simple endometrial hyperplasia - Simple glandular endometrial hyperplasia - Complex endometrial hyperplasia - Adenomatous endometrial hyperplasia - Simple glandular atypical endometrial hyperplasia - Complex atypical endometrial hyperplasia |
| Malignant tumors | - Endometrioid adenocarcinoma - Uterine carcinosarcoma |
| Endometritis | - Acute endometritis - Chronic endometritis |
| Clinical Selection | Type of Operation | Indication of Surgery | Age | Histopathological Diagnosis | Endometriosis/Adenomyosis |
|---|---|---|---|---|---|
| curettage | heavy menstrual bleeding (HMB) | 46 | proliferative phase endometrium | no | |
| LEEP + curettage | cervical cytologic atypia | 28 | CIN-II, proliferative phase endometrium | no | |
| curettage | heavy menstrual bleeding (HMB) | 39 | proliferative phase endometrium | no | |
| curettage | heavy menstrual bleeding (HMB) | 44 | disordered proliferative endometrium | no | |
| hysteroscopy (HSC) | pathological findings on ultrasound | 44 | proliferative phase endometrium | no | |
| hysteroscopy (HSC) | heavy menstrual bleeding (HMB) | 26 | proliferative phase endometrium | yes | |
| hysteroscopy (HSC) | heavy menstrual bleeding (HMB) | 31 | proliferative phase endometrium | no | |
| transcervical resection of polyp (TCRP) | pathological findings on ultrasound | 28 | disordered proliferative endometrium | no | |
| hysteroscopy (HSC) | pathological findings on ultrasound | 39 | proliferative phase endometrium | no | |
| curettage | pathological findings on ultrasound | 48 | proliferative phase endometrium | no | |
| selected | |||||
| excluded | |||||
| histopathologic exclusion | |||||
| reason of exclusion | |||||
| Menstruation | Proliferative Phase | Secretory Phase | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 |
| Early Follicaular Phase E2 = 8.7–75 ng/L → 42 ng/L | |||||||||||||||||||||||
| Follicular Phase E2 = 12.5–166 ng/L → 89 ng/L P4 = 0.06–0.9 µg/L → 0.5 µg/L | |||||||||||||||||||||||
| Ovulation E2 = 85.8–498 ng/L → 292 ng/L P4 = 0.1–12 µg/L → 6.1 µg/L | |||||||||||||||||||||||
| Luteal Phase E2 = 43.8–211 ng/L → 112.7 ng/L P4 = 1.8–24 µg/L → 12.9 µg/L | |||||||||||||||||||||||
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 205 | 17.64 |
| Secretory phase endometrium | 124 | 10.67 |
| Menstrual phase endometrium | 17 | 1.46 |
| Exogenous hormones | 72 | 6.20 |
| Menopausal endometrium | 53 | 4.56 |
| Inadequate for analysis | 188 | 16.18 |
| Endometrial polyp | 157 | 13.51 |
| Endometrial hyperplasia | 279 | 24.01 |
| Malignant tumors | 47 | 4.04 |
| Endometritis | 20 | 1.72 |
| Total | 1162 | 100 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 143 | 15.07 |
| Secretory phase endometrium | 95 | 10.01 |
| Menstrual phase endometrium | 17 | 1.79 |
| Exogenous hormones | 50 | 5.27 |
| Menopausal endometrium | 41 | 4.32 |
| Inadequate for analysis | 181 | 19.07 |
| Endometrial polyp | 117 | 12.33 |
| Endometrial hyperplasia | 253 | 26.66 |
| Malignant tumors | 42 | 4.43 |
| Endometritis | 10 | 1.05 |
| Total | 949 | 100 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 118 | 14.17 |
| Secretory phase endometrium | 82 | 9.84 |
| Menstrual phase endometrium | 15 | 1.80 |
| Exogenous hormones | 42 | 5.04 |
| Menopausal endometrium | 37 | 4.44 |
| Inadequate for analysis | 164 | 19.69 |
| Endometrial polyp | 102 | 12.24 |
| Endometrial hyperplasia | 227 | 27.25 |
| Malignant tumors | 36 | 4.32 |
| Endometritis | 10 | 1.20 |
| Total | 883 | 100 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 25 | 21.55 |
| Secretory phase endometrium | 13 | 11.21 |
| Menstrual phase endometrium | 2 | 1.72 |
| Exogenous hormones | 8 | 6.90 |
| Menopausal endometrium | 4 | 3.45 |
| Inadequate for analysis | 17 | 14.66 |
| Endometrial polyp | 15 | 12.93 |
| Endometrial hyperplasia | 26 | 22.41 |
| Malignant tumors | 6 | 5.17 |
| Endometritis | 0 | 0.00 |
| Total | 116 | 100 |
| Operation | Total Case Number | Clinically Suitable (Case Number) | Clinically Suitable (%) |
|---|---|---|---|
| D&C + HSC | 949 | 145 | 15.28 |
| D&C | 833 | 116 | 13.93 |
| HSC | 116 | 29 | 25.00 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 32 | 22.07 |
| Secretory phase endometrium | 23 | 15.86 |
| Menstrual phase endometrium | 5 | 3.45 |
| Exogenous hormones | 8 | 5.52 |
| Menopausal endometrium | 2 | 1.38 |
| Inadequate for analysis | 15 | 10.34 |
| Endometrial polyp | 13 | 8.97 |
| Endometrial hyperplasia | 45 | 31.03 |
| Malignant tumors | 1 | 0.69 |
| Endometritis | 1 | 0.69 |
| Total | 145 | 100 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 23 | 19.83 |
| Secretory phase endometrium | 20 | 17.24 |
| Menstrual phase endometrium | 4 | 3.45 |
| Exogenous hormones | 6 | 5.17 |
| Menopausal endometrium | 2 | 1.72 |
| Inadequate for analysis | 12 | 10.34 |
| Endometrial polyp | 11 | 9.48 |
| Endometrial hyperplasia | 37 | 31.90 |
| Malignant tumors | 0 | 0.00 |
| Endometritis | 1 | 0.86 |
| Total | 116 | 100 |
| Group | Case Number | Percentage (%) |
|---|---|---|
| Proliferative phase endometrium | 9 | 31.03 |
| Secretory phase endometrium | 3 | 10.34 |
| Menstrual phase endometrium | 1 | 3.45 |
| Exogenous hormones | 2 | 6.90 |
| Menopausal endometrium | 0 | 0.00 |
| Inadequate for analysis | 3 | 10.34 |
| Endometrial polyp | 2 | 6.90 |
| Endometrial hyperplasia | 8 | 27.59 |
| Malignant tumors | 1 | 3.45 |
| Endometritis | 0 | 0.00 |
| Total | 29 | 100 |
| D&C + HSC | D&C | HSC | ||||
|---|---|---|---|---|---|---|
| Total Case Number | Clinically Suitable | Total Case Number | Clinically Suitable | Total Case Number | Clinically Suitable | |
| 949 | 145 | 833 | 116 | 116 | 29 | |
| Proliferative phase endometrium | ||||||
| Suitable (case number) | 13 | 11 | 2 | |||
| Suitable (%) | 1.37 | 8.97 | 1.32 | 9.48 | 1.72 | 6.90 |
| Secretory phase endometrium | ||||||
| Suitable (case number) | 19 | 17 | 2 | |||
| Suitable (%) | 2.00 | 13.10 | 2.04 | 14.66 | 1.72 | 6.90 |
| Proliferative and secretory phase endometria | ||||||
| Suitable (case number) | 32 | 28 | 4 | |||
| Suitable (%) | 3.37 | 22.07 | 3.36 | 24.14 | 3.45 | 13.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szegeczki, V.; Fazekas, L.; Kulcsár, M.; Reglodi, D.; Török, P.; Orlik, B.; Laganà, A.S.; Jakab, A.; Juhasz, T. Endometrium as Control of Endometriosis in Experimental Research: Assessment of Sample Suitability. Diagnostics 2022, 12, 970. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040970
Szegeczki V, Fazekas L, Kulcsár M, Reglodi D, Török P, Orlik B, Laganà AS, Jakab A, Juhasz T. Endometrium as Control of Endometriosis in Experimental Research: Assessment of Sample Suitability. Diagnostics. 2022; 12(4):970. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040970
Chicago/Turabian StyleSzegeczki, Vince, László Fazekas, Máté Kulcsár, Dora Reglodi, Péter Török, Brigitta Orlik, Antonio Simone Laganà, Attila Jakab, and Tamas Juhasz. 2022. "Endometrium as Control of Endometriosis in Experimental Research: Assessment of Sample Suitability" Diagnostics 12, no. 4: 970. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12040970