
Separating Patients with SEID from Those with CFS in the French ME/CFS Association, with Some Thoughts on Nomenclature


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey of ASFC Members
2.2. Questionnaire
2.3. SEID Diagnosis
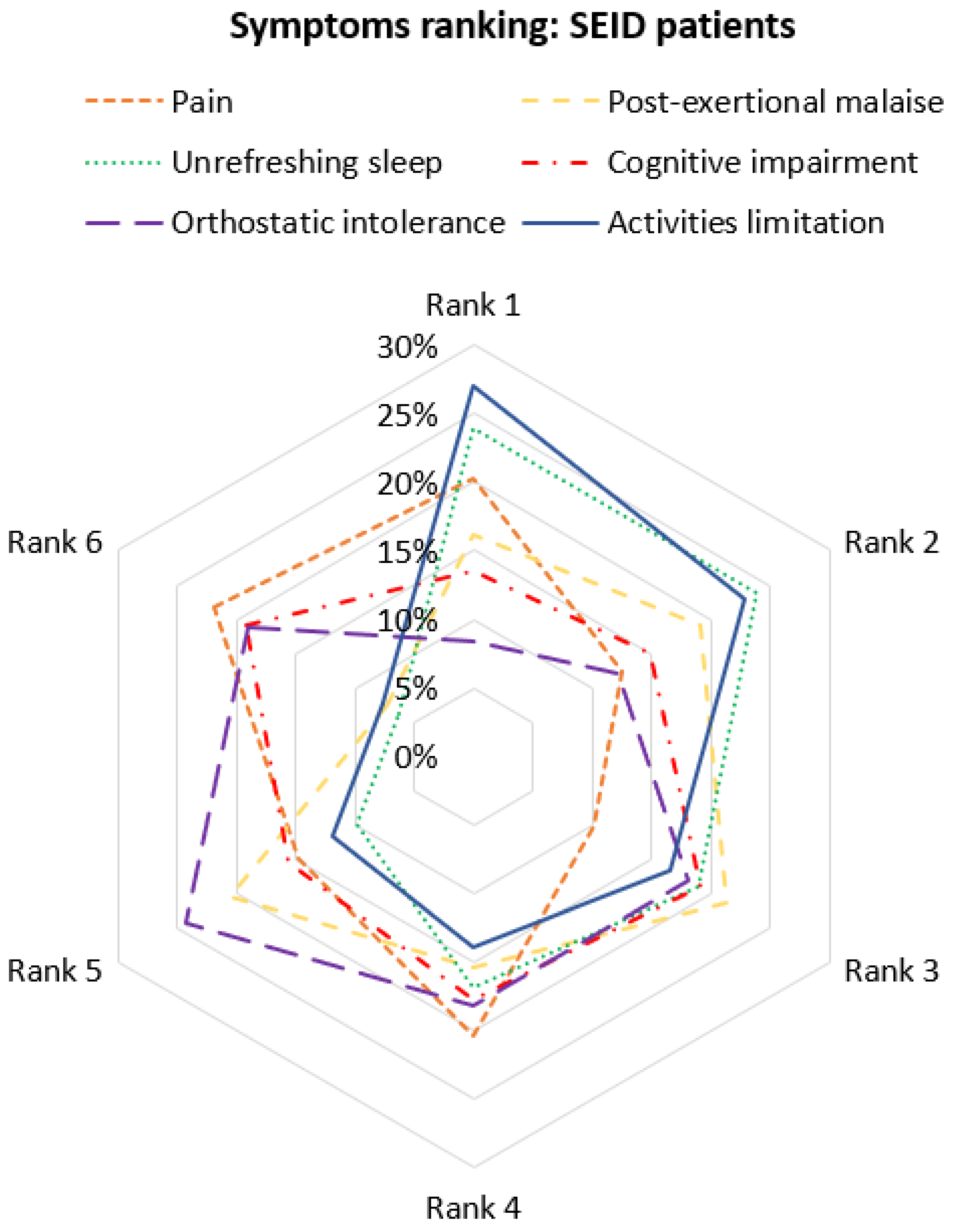
2.4. Symptoms Ranking
2.5. Statistical and Textual Analysis
3. Results
3.1. Demographics
3.2. SEID vs. Non-SEID Subjects
3.3. Distinctive Value of Symptom Questions for SEID Diagnosis
3.4. Disability Degree of Each Symptom in SEID Group
3.5. Respondents’ Opinion of SEID Label
4. Discussion
4.1. Population Studied
4.2. Main Symptoms
4.3. SEID Diagnosis
4.4. SEID vs. Non-SEID
4.4.1. PEM
4.4.2. Unrefreshing Sleep
4.4.3. Cognitive Impairment
4.4.4. Orthostatic Intolerance
4.4.5. Symptoms’ Ranking
4.4.6. Mixed Opinion about “SEID” Label
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holmes, G.P.; Kaplan, J.E.; Gantz, N.M.; Komaroff, A.L.; Schonberger, L.B.; Straus, S.E.; Jones, J.F.; Dubois, R.E.; Cunningham-Rundles, C.; Pahwa, S.; et al. Chronic fatigue syndrome: A working case definition. Ann. Intern. Med. 1988, 108, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Brurberg, K.G.; Fønhus, M.S.; Larun, L.; Flottorp, S.; Malterud, K. Case definitions for chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME): A systematic review. BMJ Open 2014, 4, e003973. [Google Scholar] [CrossRef] [PubMed]
- Sharif, K.; Watad, A.; Bragazzi, N.L.; Lichtbroun, M.; Martini, M.; Perricone, C.; Amital, H.; Shoenfeld, Y. On chronic fatigue syndrome and nosological categories. Clin. Rheumatol. 2018, 37, 1161–1170. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; Meirleir, K.L.D.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic. Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [Green Version]
- de Korwin, J.-D.; Chiche, L.; Banovic, I.; Ghali, A.; Delliaux, S.; Authier, F.-J.; Cozon, G.; Hatron, P.-Y.; Fornasieri, I.; Morinet, F. Le syndrome de fatigue chronique: Une nouvelle maladie? Rev. Med. Interne 2016, 37, 811–819. [Google Scholar] [CrossRef]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Newton, J.L. Are Myalgic Encephalomyelitis and chronic fatigue syndrome different illnesses? A preliminary analysis. J. Health Psychol. 2016, 21, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, Board on the Health of Select Populations, Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press (US): Washington, DC, USA, 2015. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK274235/ (accessed on 17 March 2015).
- Jason, L.A.; Richman, J.A. How Science Can Stigmatize: The Case of Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2007, 14, 85–103. [Google Scholar] [CrossRef]
- Sotzny, F.; Blanco, J.; Capelli, E.; Castro-Marrero, J.; Steiner, S.; Murovska, M.; Scheibenbogen, C.; on behalf of the European Network on ME/CFS (EUROMENE). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Evidence for an autoimmune disease. Autoimmun. Rev. 2018, 17, 601–609. [Google Scholar] [CrossRef]
- Corbitt, M.; Eaton-Fitch, N.; Staines, D.; Cabanas, H.; Marshall-Gradisnik, S. A systematic review of cytokines in chronic fatigue syndrome/myalgic encephalomyelitis/systemic exertion intolerance disease (CFS/ME/SEID). BMC Neurol. 2019, 19, 207. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.K.; Sarria, L.; Bekheit, M.; Collado, F.; Almenar-Pérez, E.; Martín-Martínez, E.; Alegre, J.; Castro-Marrero, J.; Fletcher, M.A.; Klimas, N.G.; et al. Unravelling myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): Gender-specific changes in the microRNA expression profiling in ME/CFS. J. Cell. Mol. Med. 2020, 24, 5865–5877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. A Literature Review of GP Knowledge and Understanding of ME/CFS: A Report from the Socioeconomic Working Group of the European Network on ME/CFS (EUROMENE). Medicina 2020, 57, 7. [Google Scholar] [CrossRef] [PubMed]
- Blease, C.; Carel, H.; Geraghty, K. Epistemic injustice in healthcare encounters: Evidence from chronic fatigue syndrome. J. Med. Ethics 2017, 3, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Bakken, I.J.; Tveito, K.; Gunnes, N.; Ghaderi, S.; Stoltenberg, C.; Trogstad, L.; Magnus, P. Two age peaks in the incidence of chronic fatigue syndrome/myalgic encephalomyelitis: A population-based registry study from Norway 2008–2012. BMC Med. 2014, 12, 167. [Google Scholar]
- Reyes, M.; Nisenbaum, R.; Hoaglin, D.C.; Unger, E.R.; Emmons, C.; Randall, B.; Stewart, J.A.; Abbey, S.; Jones, J.F.; Gantz, N.; et al. Prevalence and Incidence of Chronic Fatigue Syndrome in Wichita, Kansas. Arch. Intern. Med. 2003, 163, 1530–1536. [Google Scholar] [CrossRef] [PubMed]
- Rusu, C.; Gee, M.E.; Lagacé, C.; Parlor, M. Chronic fatigue syndrome and fibromyalgia in Canada: Prevalence and associations with six health status indicators. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2015, 35, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Rasa, S.; Nora-Krukle, Z.; Henning, N.; Eliassen, E.; Shikova, E.; Harrer, T.; Scheibenbogen, C.; Murovska, M.; Prusty, B.K. Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2018, 16, 268. [Google Scholar] [CrossRef] [Green Version]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, B.Z.; Shiraishi, Y.; Mears, C.J.; Binns, H.J.; Taylor, R. Chronic fatigue syndrome after infectious mononucleosis in adolescents. Pediatrics 2009, 124, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeus, M.; Nijs, J.; Meirleir, K.D. Chronic musculoskeletal pain in patients with the chronic fatigue syndrome: A systematic review. Eur. J. Pain 2007, 11, 377–386. [Google Scholar] [CrossRef]
- Jason, L.A.; Brown, A.; Clyne, E.; Bartgis, L.; Evans, M.; Brown, M. Contrasting case definitions for chronic fatigue syndrome, Myalgic Encephalomyelitis/chronic fatigue syndrome and myalgic encephalomyelitis. Eval. Health Prof. 2012, 35, 280–304. [Google Scholar] [CrossRef] [PubMed]
- Nacul, L.C.; Lacerda, E.M.; Pheby, D.; Campion, P.; Molokhia, M.; Fayyaz, S.; Leite, J.C.D.C.; Poland, F.; Howe, A.; Drachler, M. Prevalence of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) in three regions of England: A repeated cross-sectional study in primary care. BMC Med. 2011, 9, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Vernon, S.D.; Furst, J.; Simonis, V. Examining case definition criteria for chronic fatigue syndrome and myalgic encephalomyelitis. Fatigue Biomed. Health Behav. 2014, 2, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Newton, J.L.; Strand, E.B.; Vernon, S.D. Chronic Fatigue Syndrome versus Systemic Exertion Intolerance Disease. Fatigue Biomed. Health Behav. 2015, 3, 127–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, L.; Norris, J.L.; Valencia, I.J.; Montoya, J.G. Patients diagnosed with Myalgic encephalomyelitis/chronic fatigue syndrome also fit systemic exertion intolerance disease criteria. Fatigue Biomed. Health Behav. 2017, 5, 114–128. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; Sunnquist, M.; Gleason, K.; Fox, P. Mistaken conclusions about systemic exercise intolerance disease being comparable to research case definitions of CFS: A rebuttal to Chu et al. Fatigue Biomed. Health Behav. 2017, 5, 231–238. [Google Scholar] [CrossRef]
- Lim, E.-J.; Son, C.-G. Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2020, 18, 289. [Google Scholar] [CrossRef] [PubMed]
- De Becker, P.; McGregor, N.; De Meirleir, K. A definition-based analysis of symptoms in a large cohort of patients with chronic fatigue syndrome. J. Intern. Med. 2001, 250, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Torres-Harding, S.R.; Jurgens, A.; Helgerson, J. Comparing the Fukuda et al. Criteria and the Canadian Case Definition for Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2004, 12, 37–52. [Google Scholar] [CrossRef]
- Jason, L.A.; King, C.P.; Frankenberry, E.L.; Jordan, K.M.; Tryon, W.W.; Rademaker, F.; Huang, C.-F. Chronic fatigue syndrome: Assessing symptoms and activity level. J. Clin. Psychol. 1999, 55, 411–424. [Google Scholar] [CrossRef]
- McManimen, S.L.; Sunnquist, M.L.; Jason, L.A. Deconstructing post-exertional malaise: An exploratory factor analysis. J. Health Psychol. 2019, 24, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Gerrity, T.R.; Bates, J.; Bell, D.S.; Chrousos, G.; Furst, G.; Hedrick, T.; Hurwitz, B.; Kula, R.W.; Levine, S.M.; Moore, R.C.; et al. Chronic fatigue syndrome: What role does the autonomic nervous system play in the pathophysiology of this complex illness? Neuroimmunomodulation 2002, 10, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Low, P.A.; Sandroni, P.; Joyner, M.; Shen, W.-K. Postural tachycardia syndrome (POTS). J. Cardiovasc. Electrophysiol. 2009, 20, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Bou-Holaigah, I.; Rowe, P.C.; Kan, J.; Calkins, H. The relationship between neurally mediated hypotension and the chronic fatigue syndrome. JAMA 1995, 274, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Soetekouw, P.M.; Lenders, J.W.; Bleijenberg, G.; Thien, T.; van der Meer, J.W. Autonomic function in patients with chronic fatigue syndrome. Clin. Auton. Res. 1999, 9, 334–340. [Google Scholar] [CrossRef]
- Timmers, H.J.L.M.; Wieling, W.; Soetekouw, P.M.; Bleijenberg, G.; van der Meer, J.W.; Lenders, J.W. Hemodynamic and neurohumoral responses to head-up tilt in patients with chronic fatigue syndrome. Clin. Auton. Res. 2002, 12, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Miwa, K. Cardiac dysfunction and orthostatic intolerance in patients with myalgic encephalomyelitis and a small left ventricle. Heart Vessel. 2015, 30, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Torres-Harding, S.R.; Carrico, A.W.; Taylor, R.R. Symptom occurrence in persons with chronic fatigue syndrome. Biol. Psychol. 2002, 59, 15–27. [Google Scholar] [CrossRef]
- Roerink, M.E.; Lenders, J.W.; Schmits, I.C.; Pistorius, A.M.A.; Smit, J.W.; Knoop, H.; Van Der Meer, J.W.M. Postural orthostatic tachycardia is not a useful diagnostic marker for chronic fatigue syndrome. J. Intern. Med. 2017, 281, 179–188. [Google Scholar] [CrossRef]
- Brown, A.A.; Jason, L.A.; Evans, M.A.; Flores, S. Contrasting Case Definitions: The ME International Consensus Criteria vs. the Fukuda et al. CFS Criteria. N. Am. J. Psychol. 2013, 15, 103–120. [Google Scholar]
- Taylor, R.R.; Kielhofner, G.W. Work-related impairment and employment-focused rehabilitation options for individuals with chronic fatigue syndrome: A review. J. Ment. Health 2005, 14, 253–267. [Google Scholar] [CrossRef]
- Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. The Development of a Consistent Europe-Wide Approach to Investigating the Economic Impact of Myalgic Encephalomyelitis (ME/CFS): A Report from the European Network on ME/CFS (EUROMENE). Healthcare 2020, 8, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huibers, M.J.H.; Wessely, S. The act of diagnosis: Pros and cons of labelling chronic fatigue syndrome. Psychol. Med. 2006, 36, 895–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Sunnquist, M.; Brown, A.; McManimen, S.; Furst, J. Reflections on the Institute of Medicine’s systemic exertion intolerance disease. Pol. Arch. Med. Wewn. 2015, 125, 576–581. [Google Scholar] [CrossRef]
- Petrison, L. Survey Results (Pt. 1): Evaluating a Proposed Name to Replace “ME/CFS”. Available online: http://paradigmchange.me/wp/name-results/ (accessed on 17 March 2015).
- Jason, L.A.; Nicholson, L.; Sunnquist, M. Patient Perceptions Regarding Possible Changes to the Name and Criteria for Chronic Fatigue Syndrome and Myalgic Encephalomyelitis. J. Family Med. Community Health 2016, 3, 1090. [Google Scholar]
- Johnson, M.L.; Cotler, J.; Terman, J.M.; Jason, L.A. Risk factors for suicide in chronic fatigue syndrome. Death Stud. 2022, 46, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Taylor, R.R.; Plioplys, S.; Stepanek, Z.; Shlaes, J. Evaluating attributions for an illness based upon the name: Chronic fatigue syndrome, myalgic encephalopathy and Florence Nightingale disease. Am. J. Community Psychol. 2002, 30, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Holbert, C.; Torres-Harding, S.; Taylor, R.R. Stigma and the Term Chronic Fatigue Syndrome: Results of Surveys on Changing the Name. J. Disabil. Policy Stud. 2004, 14, 222–228. [Google Scholar] [CrossRef]
- Nicholson, L.; Brown, A.; Jason, L.A.; Ohanian, D.; O’Connor, K. Educational Priorities for Healthcare Providers and Name Suggestions for Chronic Fatigue Syndrome: Including the Patient Voice. Clin. Res. Open Access 2016, 2. [Google Scholar] [CrossRef]
- Twisk, F.N.M. Replacing Myalgic Encephalomyelitis and Chronic Fatigue Syndrome with Systemic Exercise Intolerance Disease Is Not the Way forward. Diagnostics 2016, 6, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twisk, F.N.M. A critical analysis of the proposal of the Institute of Medicine to replace myalgic encephalomyelitis and chronic fatigue syndrome by a new diagnostic entity called systemic exertion intolerance disease. Curr. Med. Res. Opin. 2015, 31, 1333–1347. [Google Scholar] [CrossRef] [PubMed]
- Strassheim, V.J.; Sunnquist, M.; Jason, L.A.; Newton, J.L. Defining the prevalence and symptom burden of those with self-reported severe chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME): A two-phase community pilot study in the North East of England. BMJ Open 2018, 8, e020775. [Google Scholar] [CrossRef]
- Asprusten, T.T.; Sulheim, D.; Fagermoen, E.; Winger, A.; Skovlund, E.; Wyller, V.B. Systemic exertion intolerance disease diagnostic criteria applied on an adolescent chronic fatigue syndrome cohort: Evaluation of subgroup differences and prognostic utility. BMJ Paediatr. Open 2018, 2, e000233. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, A.M.; David, A.S.; Wessely, S.; Pelosi, A.J.; Dowsett, E.G. Myalgic Encephalomyelitis, or what? Lancet 1988, 332, 100–101. [Google Scholar] [CrossRef]
- NICE Guideline. Myalgic Encephalomyelitis (or Encephalopathy)/Chronic Fatigue Syndrome: Diagnosis and Management. 29 October 2021. Available online: www.nice.org.uk/guidance/ng206 (accessed on 27 January 2022).
- Wong, L.T.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ALL | SEID | NON SEID | p Value | |
|---|---|---|---|---|
| Population | n = 178 | n = 150 | n = 28 | |
| Age | r = 178 | r = 150 | r = 28 | |
| Mean | 51.7 | 51.7 | 51.7 | ns |
| Sex | r = 178 | r = 150 | r = 28 | |
| Women | 149 (84) | 127 (85) | 22 (79) | ns |
| Men | 29 (16) | 23 (15) | 6 (21) | |
| Fatigue onset | r = 137 | r = 118 | r = 19 | |
| Sudden | 64 (47) | 52 (44) | 12 (63) | ns |
| Progressive | 73 (53) | 66 (56) | 7 (37) | |
| Trigger | r = 104 | r = 82 | r = 22 | |
| Infectious | 72 (69) | 56 (68) | 16 (73) | ns |
| Psychological | 14 (13) | 9 (11) | 5 (23) | ns |
| Surgery | 8 (8) | 7 (9) | 1 (5) | ns |
| Hormonal disorder | 7 (7) | 7 (9) | 0 (0) | ns |
| Diagnostic delay | r = 159 | r = 135 | r = 24 | |
| Mean | 7.0 | 7.2 | 5.3 | 5.04 × 10−4 |
| Other symptoms | r = 174 | r = 149 | r = 25 | |
| Generalized pain | 144 (83) | 124 (83) | 20 (80) | ns |
| Sore throat | 83 (48) | 71 (48) | 12 (48) | ns |
| Swollen cervical lymph nodes | 62 (36) | 50 (34) | 12 (48) | ns |
| Swollen axillary lymph nodes | 19 (11) | 16 (11) | 3 (12) | ns |
| Cold sensation | 127 (73) | 106 (71) | 21 (84) | ns |
| Unusual sweats | 106 (61) | 92 (62) | 14 (56) | ns |
| SEID Criteria | SEID | Non SEID | ||
|---|---|---|---|---|
| 1-Fatigue | r = 150 | 150 (100) | r = 28 | 28 (100) |
| S1. Compared to what you were able to do before being exhausted, | ||||
| P1. I feel a flu-like fatigue/exhaustion | r = 149 | 80 (54) | r = 28 | 17 (61) |
| P2. I feel like a battery that is never able to be recharged fully despite resting a lot and limiting my activities | r = 150 | 142 (97) | r = 28 | 25 (89) |
| P3. Thinking takes a lot more work than it used to | r = 150 | 108 (72) | r = 28 | 20 (71) |
| 2-Post-exertional malaise | r = 150 | 150 (100) | r = 28 | 24 (86) |
| S2. After a physical or mental activities, prolonged standing, | ||||
| P1. I feel crashed, relapsed, collapsed | r = 150 | 142 (95) | r = 28 | 20 (71) |
| P2. I feel mentally tired after the slightest effort | r = 146 | 95 (65) | r = 28 | 7 (25) |
| P3. I feel physically drained or sick after mild activity | r = 149 | 136 (91) | r = 28 | 16 (57) |
| P4. The more demanding or prolonged the activity, the more severe and prolonged the payback | r = 150 | 144 (96) | r = 28 | 24 (86) |
| 3-Unrefreshing sleep | r = 150 | 150 (100) | r = 28 | 4 (14) |
| S3. Concerning my sleep, | ||||
| P1. I feel exhausted like I never slept | r = 148 | 128 (86) | r = 28 | 3 (11) |
| P2. I cannot fall asleep or stay asleep | r = 146 | 123 (84) | r = 28 | 3 (11) |
| P3. After long or normal hours of sleep, I still don’t feel good in the morning | r = 148 | 119 (80) | r = 27 | 3 (11) |
| 4-Cognitive impairment | r = 150 | 133 (89) | r = 28 | 19 (68) |
| S4. On the intellectual level or to carry out certain activities such as driving, reading a book, watching a movie, working on computer or participating in a discussion, | ||||
| P1. I feel like a brain fog | r = 146 | 73 (50) | r = 28 | 10 (36) |
| P2. I feel confused | r = 143 | 57 (40) | r = 28 | 7 (25) |
| P3. I feel disoriented | r = 144 | 47 (33) | r = 28 | 4 (14) |
| P4. It is hard to concentrate, I cannot focus | r = 148 | 101 (68) | r = 28 | 11 (39) |
| P5. I cannot process information | r = 146 | 46 (32) | r = 28 | 5 (18) |
| (A) | |
|---|---|
| SEID | |
| n = 150 | |
| Is SEID terminology more appropriate than CFS? | r = 150 |
| Absolutely | 27 (18) |
| Slightly | 42 (28) |
| Not at all | 59 (39) |
| I don’t know | 22 (15) |
| Problem with the image its gives of the disease? | |
| In your family? | r = 149 |
| Very concerned | 45 (30) |
| Slightly concerned | 39 (26) |
| Not concerned | 44 (30) |
| I don’t know | 21 (14) |
| In social relationships? | r = 147 |
| Very concerned | 44 (30) |
| Slightly concerned | 35 (24) |
| Not concerned | 36 (24) |
| I don’t know | 32 (22) |
| At work? | r = 122 |
| Very concerned | 46 (38) |
| Slightly concerned | 23 (19) |
| Not concerned | 20 (16) |
| I don’t know | 33 (27) |
| (B) | |
| Unfavorable comments | |
| "Exertion intolerance" is pejorative | 29 (23) |
| means laziness, patients are "shiftless" | |
| Fatigue without exertion/with minimal effort | 21 (16) |
| no better professional/administrative/ medical recognition | 14 (11) |
| More than just an "exertion intolerance" | 12 (9) |
| Too complicated, "systemic" not understood | 11 (9) |
| Not "serious" or "scientific" enough | 7 (5) |
| Removal of "chronic" term | 3 (2) |
| Favorable comments | |
| Use of "disease" term | 21 (16) |
| Use of "systemic" term | 3 (2) |
| Removal of "fatigue" term | 2 (2) |
| Name proposals | |
| Keep "ME" | 12 (9) |
| Use of "exhaustion" term | 10 (8) |
| Reflect handicap/disability | 6 (5) |
| Include chronic pain | 4 (3) |
| Keep "CFS" | 3 (2) |
| Use "FM" | 3 (2) |
| Include cognitive signs, | 3 (2) |
| refer to biological causes, use a proper name, use "syndrome", "neurological", "multisystemic", "immunological", "disabling" terms, a more scientific name | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campagne, J.; Fornasieri, I.; Andreani, B.; Eginard, M.; de Korwin, J.-D. Separating Patients with SEID from Those with CFS in the French ME/CFS Association, with Some Thoughts on Nomenclature. Diagnostics 2022, 12, 1095. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051095
Campagne J, Fornasieri I, Andreani B, Eginard M, de Korwin J-D. Separating Patients with SEID from Those with CFS in the French ME/CFS Association, with Some Thoughts on Nomenclature. Diagnostics. 2022; 12(5):1095. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051095
Chicago/Turabian StyleCampagne, Julien, Isabelle Fornasieri, Barbara Andreani, Monique Eginard, and Jean-Dominique de Korwin. 2022. "Separating Patients with SEID from Those with CFS in the French ME/CFS Association, with Some Thoughts on Nomenclature" Diagnostics 12, no. 5: 1095. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051095