
Necrotizing Skin and Soft Tissue Infection Due to Syncephalastrum Species and Fusarium solani Species Complex Following Open Tibia Fracture



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
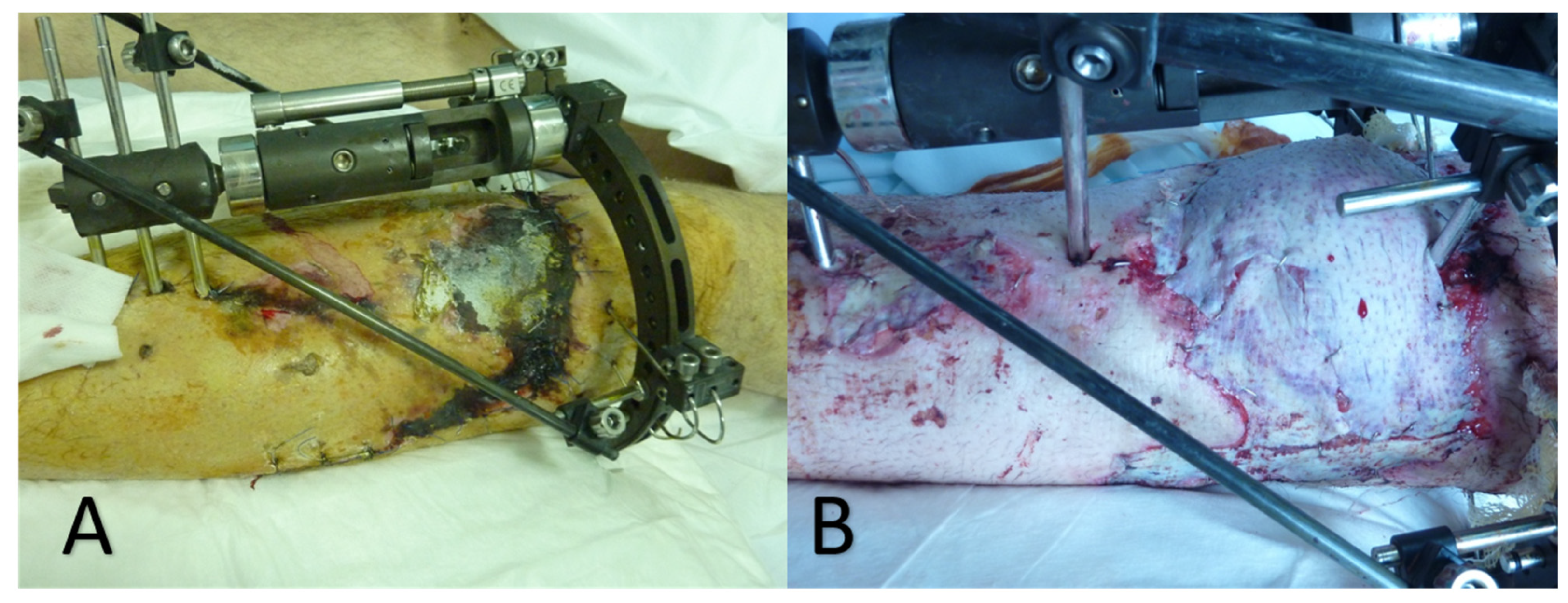
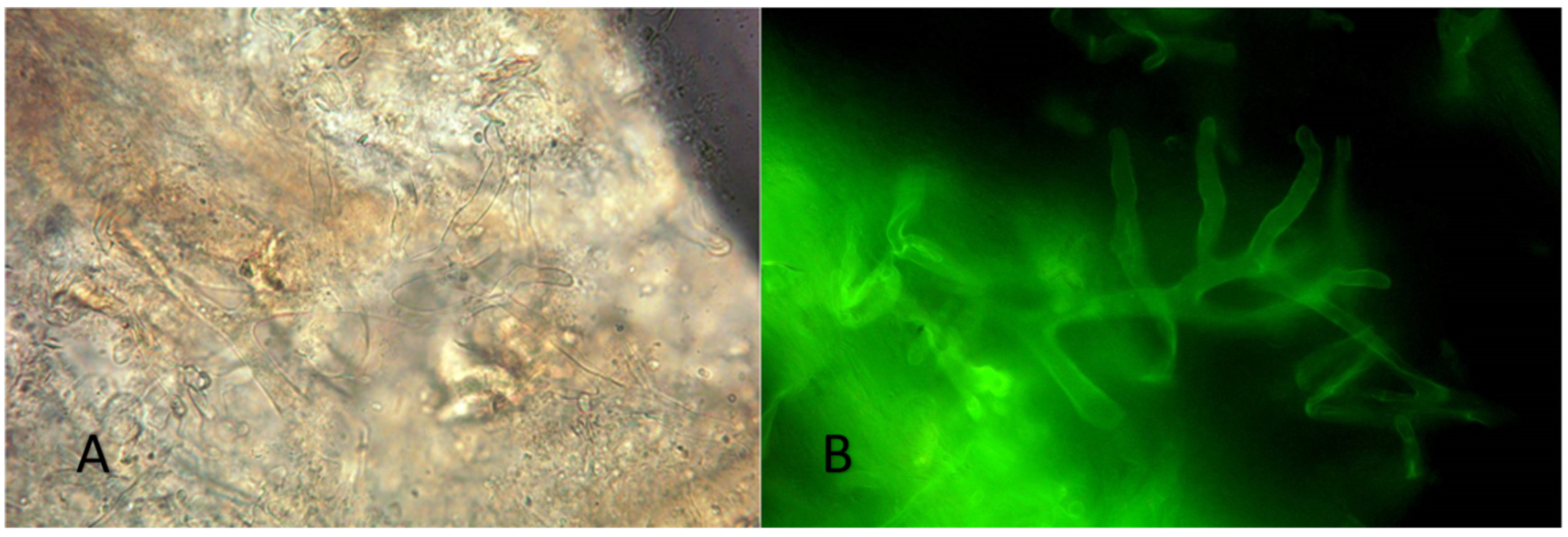
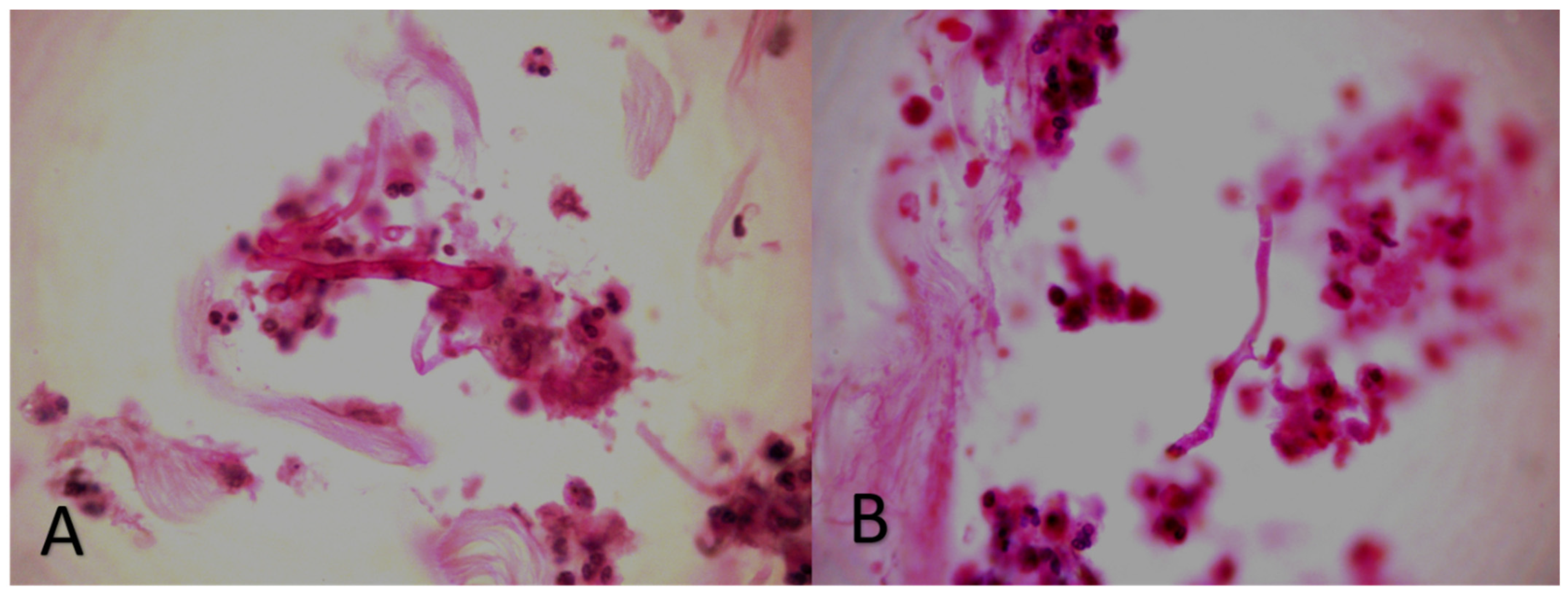
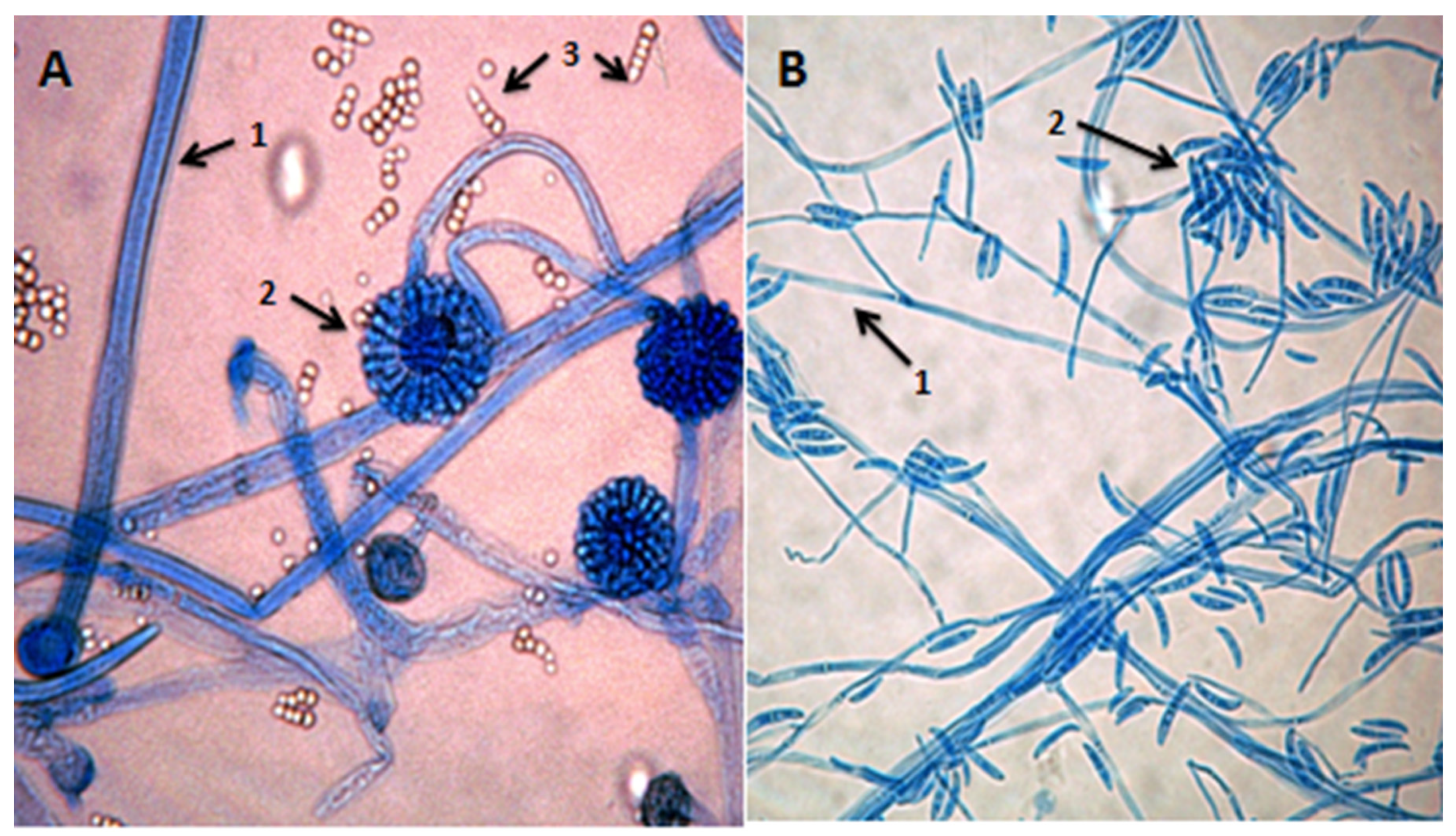
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stevens, D.L.; Bryant, A.E.; Goldstein, E.J. Necrotizing Soft Tissue Infections. Infect. Dis. Clin. N. Am. 2021, 35, 135–155. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.M.; McCarty, A.; Jalilvand, A.; Strassels, S.; Schubauer, K.; Gonzalez-Gallo, K.; Young, A.; Wisler, J. Outcomes of Patients with Necrotizing Soft Tissue Infections: A Propensity-Matched Analysis Using the National Inpatient Sample. Surg. Infect. 2022, 23, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.L.; Fasolka, B.; Treacy, C. Necrotizing fasciitis: A comprehensive review. Nursing 2020, 50, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, K.; Salinas, R.C.; Agudelo Higuita, N.I. Skin and Soft Tissue Infections. Am. Fam. Physician 2015, 92, 474–483. [Google Scholar] [PubMed]
- Andrianaki, A.M.; Koutserimpas, C.; Kafetzakis, A.; Tavlas, E.; Maraki, S.; Papadakis, J.A.; Ioannou, P.; Samonis, G.; Kofteridis, D.P. Diabetic foot infection and osteomyelitis. Are deep-tissue cultures necessary? Germs 2020, 10, 346–355. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Chamakioti, I.; Naoum, S.; Raptis, K.; Alpantaki, K.; Samonis, G. Native Joint Infections by Aspergillus Species. Diagnostics 2021, 11, 2335. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Chamakioti, I.; Raptis, K.; Alpantaki, K.; Vrioni, G.; Samonis, G. Osseous Infections Caused by Aspergillus Species. Diagnostics 2022, 12, 201. [Google Scholar] [CrossRef]
- Mamali, V.; Koutserimpas, C.; Zarkotou, O.; Vrioni, G.; Samonis, G. Isolated Cerebral Mucormycosis Caused by Lichtheimia Species in a Polytrauma Patient. Diagnostics 2022, 12, 358. [Google Scholar] [CrossRef]
- Skiada, A.; Lass-Floerl, C.; Klimko, N.; Ibrahim, A.; Roilides, E.; Petrikkos, G. Challenges in the diagnosis and treatment of mucormycosis. Med. Mycol. 2018, 56 (Suppl. S1), 93–101. [Google Scholar] [CrossRef] [Green Version]
- Ang, A.; Chew, K.L. Disseminated Fusarium solani complex infection. Clin. Microbiol. Infect. 2020, 26, 1636–1637. [Google Scholar] [CrossRef]
- Peetermans, M.; de Prost, N.; Eckmann, C.; Norrby-Teglund, A.; Skrede, S.; De Waele, J.J. Necrotizing skin and soft-tissue infections in the intensive care unit. Clin. Microbiol. Infect. 2020, 26, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, K.; Esposito, S.; Gould, I.; Ascione, T.; Bassetti, M.; Bonnet, E.; Bouza, E.; Chan, M.; Davis, J.S.; De Simone, G.; et al. Hot topics in necrotising skin and soft tissue infections. Int. J. Antimicrob. Agents 2018, 52, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madsen, M.B.; Arnell, P.; Hyldegaard, O. Necrotizing Soft-Tissue Infections: Clinical Features and Diagnostic Aspects. Adv. Exp. Med. Biol. 2020, 1294, 39–52. [Google Scholar] [PubMed]
- Irshad, M.; Nasir, N.; Hashmi, U.H.; Farooqi, J.; Mahmood, S.F. Invasive pulmonary infection by Syncephalastrum species: Two case reports and review of literature. IDCases 2020, 21, e00913. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.A.; Kong, D.C.M.; Chen, S.C. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 2019, 25, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Reid, G.; Lynch, J.P., 3rd; Fishbein, M.C.; Clark, N.M. Mucormycosis. Semin. Respir. Crit. Care Med. 2020, 41, 99–114. [Google Scholar] [CrossRef]
- Chander, J.; Kaur, M.; Singla, N.; Punia, R.P.S.; Singhal, S.K.; Attri, A.K.; Alastruey-Izquierdo, A.; Stchigel, A.M.; Cano-Lira, J.F.; Guarro, J. Mucormycosis: Battle with the Deadly Enemy over a Five-Year Period in India. J. Fungi 2018, 4, 46. [Google Scholar] [CrossRef] [Green Version]
- Skiada, A.; Drogari-Apiranthitou, M.; Pavleas, I.; Daikou, E.; Petrikkos, G. Global Cutaneous Mucormycosis: A Systematic Review. J. Fungi 2022, 8, 194. [Google Scholar] [CrossRef]
- Amatya, R.; Khanal, B.; Rijal, A. Syncephalastrum species producing mycetoma-like lesions. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 284–286. [Google Scholar] [CrossRef]
- Chavan, R.; Menon, A.; Soman, R.; Rodrigues, C.; Shetty, A.; Bhadiyadra, R.; Agashe, V.M. Fungal osteomyelitis and soft tissue infections: Simple solutions to uncommon scenarios. J. Infect. Dev. Ctries. 2020, 14, 1033–1039. [Google Scholar] [CrossRef]
- Petrikkos, G.; Skiada, A.; Lortholary, O.; Roilides, E.; Walsh, T.J.; Kontoyiannis, D.P. Epidemiology and clinical manifestations of mucormycosis. Clin. Infect. Dis. 2012, 54 (Suppl. S1), S23–S34. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Weintrob, A.C.; Dunne, J.R.; Weisbrod, A.B.; Lloyd, B.; Warkentien, T.; Malone, D.; Wells, J.; Murray, C.K.; Bradley, W.; et al. Clinical relevance of mold culture positivity with and without recurrent wound necrosis following combat-related injuries. J. Trauma Acute Care Surg. 2014, 77, 769–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonifaz, A.; Tirado-Sánchez, A.; Hernández-Medel, M.L.; Kassack, J.J.; Araiza, J.; González, G.M. Mucormycosis with cutaneous involvement. A retrospective study of 115 cases at a tertiary care hospital in Mexico. Australas. J. Dermatol. 2021, 62, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Barcoto, M.O.; Pedrosa, F.; Bueno, O.C.; Rodrigues, A. Pathogenic nature of Syncephalastrum in Atta sexdens rubropilosa fungus gardens. Pest Manag. Sci. 2017, 73, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Mangaraj, S.; Sethy, G.; Patro, M.K.; Padhi, S. A rare case of subcutaneous mucormycosis due to Syncephalastrum racemosum: Case report and review of literature. Indian J. Med. Microbiol. 2014, 32, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Jindal, N.; Kalra, N.; Arora, S.; Arora, D.; Bansal, R. Onychomycosis of toenails caused by Syncephalastrum racemosum: A rare non-dermatophyte mould. Indian J. Med Microbiol. 2016, 34, 257–258. [Google Scholar] [CrossRef] [PubMed]
- Raju, B.; Santhanakumar, K.S.; Kesavachandran, U. Gastrointestinal involvement of unusual Mucormycete Syncephalastrum racemosum in a diabetic patient with adenocarcinoma: Rare case presentation with review of literature. Infection 2020, 48, 791–797. [Google Scholar] [CrossRef]
- Mohanty, P.; Dash, S.; Mohapatra, L.; Jain, M. Total Dystrophic Onychomycosis Due to Syncephalastrum racemosum—A Rare Cause and Its Novel Treatment Option. Indian Dermatol. Online J. 2019, 10, 171–173. [Google Scholar]
- De Hoog, G.S.; Guarro, J.; Gene, J.; Figueras, M.J. Atlas of Clinical Fungi, 2nd ed.; Centraalbureau voor Schimmelcultures: Utrecht, The Netherlands, 2000; Volume 1. [Google Scholar]
- Tang, P.J.; Zhang, Z.H.; Niu, L.L.; Gu, C.B.; Zheng, W.Y.; Cui, H.C.; Yuan, X.H. Fusarium solani G6, a novel vitexin-producing endophytic fungus: Characterization, yield improvement and osteoblastic proliferation activity. Biotechnol. Lett. 2021, 43, 1371–1383. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Richardson, M.; Roilides, E.; Van Diepeningen, A.; Caira, M.; Munoz, P.; Johnson, E.; Meletiadis, J.; Pana, Z.D.; Lackner, M.; et al. ESCMID and ECMM joint guidelines on diagnosis and management of hyalohyphomycosis: Fusarium spp.; Scedosporium spp. and others. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 27–46. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Anaissie, E. Cutaneous infection by Fusarium species in healthy and immunocompromised hosts: Implications for diagnosis and management. Clin. Infect. Dis. 2002, 35, 909–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, J.J. The Fusarium solani species complex: Ubiquitous pathogens of agricultural importance. Mol. Plant Pathol. 2016, 17, 146–158. [Google Scholar] [CrossRef] [PubMed]
- Bellanger, A.P.; Rocchi, S.; Berceanu, A.; Scherer, E.; Larosa, F.; Millon, L. Positive quantitative PCR detecting Fusarium solani in a case of mixed invasive fungal disease due to Mucorales and Fusarium solani. Bone Marrow Transplant. 2020, 55, 873–876. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, P.; Guedouar, H.; Laouiti, F.; Grenouillet, F.; Dannaoui, E. Identification of Mucorales by Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry. J. Fungi 2019, 5, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duane, T.M.; Huston, J.M.; Collom, M.; Beyer, A.; Parli, S.; Buckman, S.; Shapiro, M.; McDonald, A.; Diaz, J.; Tessier, J.M.; et al. Surgical Infection Society 2020 Updated Guidelines on the Management of Complicated Skin and Soft Tissue Infections. Surg. Infect. 2021, 22, 383–399. [Google Scholar] [CrossRef]
- Hsiao, C.T.; Weng, H.H.; Yuan, Y.D.; Chen, C.T.; Chen, I.C. Predictors of mortality in patients with necrotizing fasciitis. Am. J. Emerg. Med. 2008, 26, 170–175. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamali, V.; Koutserimpas, C.; Manoloudaki, K.; Zarkotou, O.; Samonis, G.; Vrioni, G. Necrotizing Skin and Soft Tissue Infection Due to Syncephalastrum Species and Fusarium solani Species Complex Following Open Tibia Fracture. Diagnostics 2022, 12, 1163. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051163
Mamali V, Koutserimpas C, Manoloudaki K, Zarkotou O, Samonis G, Vrioni G. Necrotizing Skin and Soft Tissue Infection Due to Syncephalastrum Species and Fusarium solani Species Complex Following Open Tibia Fracture. Diagnostics. 2022; 12(5):1163. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051163
Chicago/Turabian StyleMamali, Vasiliki, Christos Koutserimpas, Kassiani Manoloudaki, Olympia Zarkotou, George Samonis, and Georgia Vrioni. 2022. "Necrotizing Skin and Soft Tissue Infection Due to Syncephalastrum Species and Fusarium solani Species Complex Following Open Tibia Fracture" Diagnostics 12, no. 5: 1163. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051163