
Prediction of Two-Year Recurrence-Free Survival in Operable NSCLC Patients Using Radiomic Features from Intra- and Size-Variant Peri-Tumoral Regions on Chest CT Images



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Data Preparation
2.3. Radiomic Feature Extraction and Selection
2.4. Prediction of the 2-Year Recurrence-Free Survival
3. Results
3.1. Experimental Setting
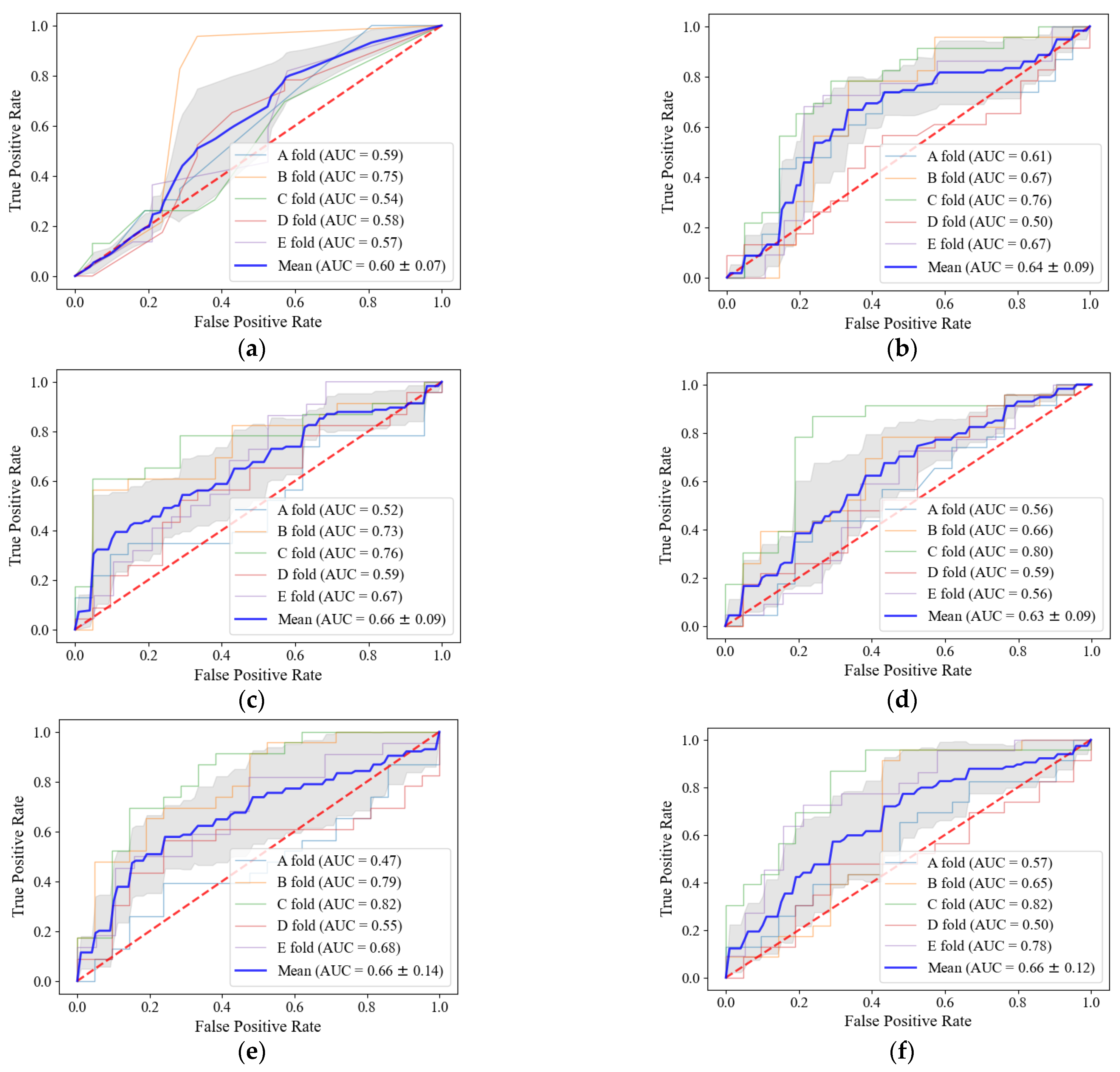
3.2. Classification into Recurrence and Non-Recurrence Group Using Radiomic Features
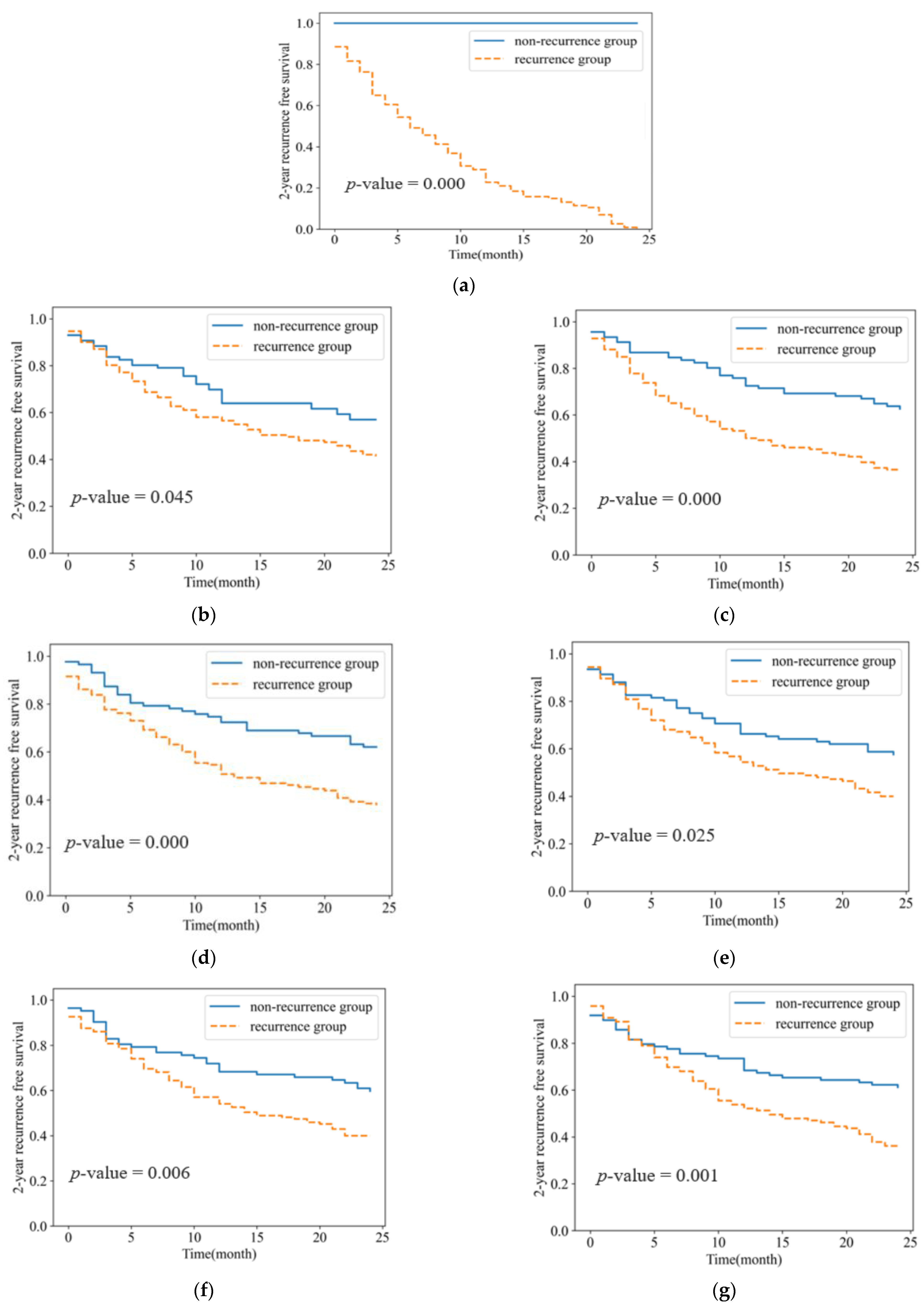
3.3. Probability Estimation of 2-Year Recurrence-Free Survival
3.4. Classification Performance of Radiomic Feature according to the Tumor Size
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-Small Cell Lung Cancer: Epidemiology, Risk Factors, Treatment, and Survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Zheng, M. Classification and Pathology of Lung Cancer. Surg. Oncol. Clin. N. Am. 2016, 25, 447–468. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more ‘personalized’ approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Yoon, S.M.; Shaikh, T.; Hallman, M. Therapeutic management options for stage III non-small cell lung cancer. World J. Clin. Oncol. 2017, 8, 1–20. [Google Scholar] [CrossRef]
- Zarogoulidis, K.; Zarogoulidis, P.; Darwiche, K.; Boutsikou, E.; Machairiotis, N.; Tsakiridis, K.; Katsikogiannis, N.; Kougioumtzi, I.; Karapantzos, I.; Huang, H.; et al. Treatment of non-small cell lung cancer (NSCLC). J. Thorac. Dis. 2013, 5, S389–S396. [Google Scholar] [CrossRef]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar] [CrossRef]
- Uramoto, H.; Tanaka, F. Prediction of recurrence after complete resection in patients with NSCLC. Anticancer. Res. 2012, 32, 3953–3960. [Google Scholar]
- Zhang, Y.; Oikonomou, A.; Wong, A.; Haider, M.A.; Khalvati, F. Radiomics-based Prognosis Analysis for Non-Small Cell Lung Cancer. Sci. Rep. 2017, 7, srep46349. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coroller, T.P.; Grossmann, P.; Hou, Y.; Rios Velazquez, E.; Leijenaar, R.T.H.; Hermann, G.; Lambin, P.; Haibe-Kains, B.; Mak, R.H.; Aerts, H.J.W.L. CT-based radiomic signature predicts distant metastasis in lung adenocarcinoma. Radiother. Oncol. 2015, 114, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Coroller, T.P.; Agrawal, V.; Huynh, E.; Narayan, V.; Lee, S.W.; Mak, R.H.; Aerts, H.J. Radiomic-Based Pathological Response Prediction from Primary Tumors and Lymph Nodes in NSCLC. J. Thorac. Oncol. 2016, 12, 467–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cong, M.; Feng, H.; Ren, J.-L.; Xu, Q.; Cong, L.; Hou, Z.; Wang, Y.-Y.; Shi, G. Development of a predictive radiomics model for lymph node metastases in pre-surgical CT-based stage IA non-small cell lung cancer. Lung Cancer 2019, 139, 73–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, S.; He, Y.; Allen, B.G.; Buatti, J.M.; Smith, B.J.; Tong, L.; Sun, Z.; Wu, J.; Diehn, M.; Loo, B.W.; et al. Deep segmentation networks predict survival of non-small cell lung cancer. Sci. Rep. 2019, 9, 17286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dou, T.H.; Coroller, T.P.; Van Griethuysen, J.J.M.; Mak, R.H.; Aerts, H.J.W.L. Peritumoral radiomics features predict distant metastasis in locally advanced NSCLC. PLoS ONE 2018, 13, e0206108. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhao, X.; Li, Q.; Xia, W.; Peng, Z.; Zhang, R.; Li, Q.; Jian, J.; Wang, W.; Tang, Y.; et al. Can peritumoral radiomics increase the efficiency of the prediction for lymph node metastasis in clinical stage T1 lung adenocarcinoma on CT? Eur. Radiol. 2019, 29, 6049–6058. [Google Scholar] [CrossRef]
- Khorrami, M.; Khunger, M.; Zagouras, A.; Patil, P.; Thawani, R.; Bera, K.; Rajiah, P.; Fu, P.; Velcheti, V.; Madabhushi, A. Combination of Peri- and Intratumoral Radiomic Features on Baseline CT Scans Predicts Response to Chemotherapy in Lung Adenocarcinoma. Radiol. Artif. Intell. 2019, 1, 2. [Google Scholar] [CrossRef]
- Vaidya, P.; Bera, K.; Gupta, A.; Wang, X.; Corredor, G.; Fu, P.; Beig, N.; Prasanna, P.; Patil, P.D.; Velu, P.D.; et al. CT derived radiomic score for predicting the added benefit of adjuvant chemotherapy following surgery in stage I, II resectable non-small cell lung cancer: A retrospective multicohort study for outcome prediction. Lancet Digit. Health 2020, 2, e116–e128. [Google Scholar] [CrossRef] [Green Version]
- D’Antonoli, T.A.; Farchione, A.; Lenkowicz, J.; Chiappetta, M.; Cicchetti, G.; Martino, A.; Ottavianelli, A.; Manfredi, R.; Margaritora, S.; Bonomo, L.; et al. CT Radiomics Signature of Tumor and Peritumoral Lung Parenchyma to Predict Nonsmall Cell Lung Cancer Postsurgical Recurrence Risk. Acad. Radiol. 2019, 27, 497–507. [Google Scholar] [CrossRef]
- Soille, P. Morphological Image Analysis: Principles and Applications; Springer: Berlin/Heidelberg, Germany, 2013; Available online: https://books.google.co.kr/books?id=ZFzxCAAAQBAJ (accessed on 2 February 2022).
- Garzelli, L.; Goo, J.M.; Ahn, S.Y.; Chae, K.J.; Park, C.M.; Jung, J.; Hong, H. Improving the prediction of lung adenocarcinoma invasive component on CT: Value of a vessel removal algorithm during software segmentation of subsolid nodules. Eur. J. Radiol. 2018, 100, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Hong, H.; Goo, J.M. Ground-glass nodule segmentation in chest CT images using asymmetric multi-phase deformable model and pulmonary vessel removal. Comput. Biol. Med. 2018, 92, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Radiomics Community. Radiomic Features. Available online: https://pyradiomics.readthedocs.io/en/latest/features.html (accessed on 22 December 2021).
- Goldberger, J.; Roweis, S.; Hinton, G.; Salakhutdinov, R. Neighbourhood Components Analysis. In Advances in Neural Information Processing Systems 17: Proceedings of the 2004 Conference; MIT Press: Cambridge, MA, USA, 2004. [Google Scholar]
- Hilden, J.; Glasziou, P. Regret graphs, diagnostic uncertainty and Youden’s Index. Stat. Med. 1996, 15, 969–986. [Google Scholar] [CrossRef]
- Boser, B.E.; Guyon, I.M.; Vapnik, V.N. A training algorithm for optimal margin classifiers. In Proceedings of the Fifth Annual Workshop on Computational Learning Theory, Pittsburgh, PA, USA, 27–29 July 1992; pp. 144–152. [Google Scholar] [CrossRef]
- Ho, T.K. The random subspace method for constructing decision forests. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 20, 832–844. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 12: Survival analysis. Crit. Care 2004, 8, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2018, 17, 168–192. [Google Scholar] [CrossRef]
- Bashir, U.; Siddique, M.M.; Mclean, E.; Goh, V.; Cook, G.J. Imaging Heterogeneity in Lung Cancer: Techniques, Applications, and Challenges. Am. J. Roentgenol. 2016, 207, 534–543. [Google Scholar] [CrossRef]
- Lubner, M.G.; Smith, A.D.; Sandrasegaran, K.; Sahani, D.V.; Pickhardt, P.J. CT Texture Analysis: Definitions, Applications, Biologic Correlates, and Challenges. Radiographics 2017, 37, 1483–1503. [Google Scholar] [CrossRef]
- Kadota, K.; Nitadori, J.; Sima, C.S.; Ujiie, H.; Rizk, N.P.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J. Thorac. Oncol. 2015, 10, 806–814. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total (n = 217) | Non-Recurrence (n = 103) | Recurrence (n = 114) | |
|---|---|---|---|---|
| Age | 73.14 (62–89) | 72 | 74.3 | |
| Gender | ||||
| Male | 212 (98%) | 99 | 113 | |
| Female | 5 (2%) | 4 | 1 | |
| Histology | ||||
| Adenocarcinomas | 89 (41%) | 47 | 42 | |
| Squamous cell carcinomas | 128 (59%) | 56 | 72 | |
| T stage 1 | ||||
| T1 | 90 (41%) | 56 | 34 | |
| T2 | 113 (52%) | 43 | 70 | |
| T3 | 14 (6%) | 4 | 10 | |
| N stage 1 | ||||
| N0 | 122 (56%) | 71 | 51 | |
| N1 | 56 (26%) | 21 | 35 | |
| N2 | 39 (18%) | 11 | 28 | |
| Categories | Sub-Categories | Features |
|---|---|---|
| Intensity | Histogram Statistics (7) | mean, std, min, max, skewness, kurtosis, entropy |
| Histogram Percentile (5) | 5%, 25%, 50%, 75%, 95% | |
| Texture | GLCM features (14) | mean and std dev pairs of ASM, contrast, sum average, sum variance, sum entropy, entropy, difference entropy |
| GLRLM features (22) | mean and std dev pairs of short and long run emphasis, low and high gray-level emphasis, non-uniformity, run percentage, etc. | |
| LBP features (10) | local binary patterns using 10 visual descriptors. | |
| Shape | Size and Roundness (11) | area/perimeter ratio, convex area, eccentricity, Euler number, major-minor axis ratio, major axis length, minor axis length, area, perimeter, curvature |
| Classifier | ACC | SEN | SPEC | AUC | Classifier | ACC | SEN | SPEC | AUC | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T stage and N stage | 58.61 | 68.73 | 47.49 | 0.60 | Intratumoral radiomic features | 63.23 | 70.82 | 55.03 | 0.64 | ||
| Peritumoral radiomic features | 3 mm | 61.32 | 67.64 | 54.33 | 0.66 | Combined radiomic features | 3 mm | 62.68 | 67.16 | 57.65 | 0.65 |
| 6 mm | 57.70 | 65.10 | 49.59 | 0.59 | 6 mm | 60.18 | 68.27 | 51.23 | 0.66 | ||
| 9 mm | 58.60 | 68.04 | 48.14 | 0.62 | 9 mm | 62.78 | 66.64 | 58.65 | 0.66 | ||
| 12 mm | 58.60 | 64.90 | 51.59 | 0.63 | 12 mm | 58.05 | 63.36 | 51.99 | 0.64 | ||
| 15 mm | 57.58 | 59.72 | 55.04 | 0.58 | 15 mm | 58.68 | 64.85 | 51.92 | 0.65 | ||
| 18 mm | 58.09 | 64.94 | 50.36 | 0.61 | 18 mm | 60.78 | 66.63 | 54.40 | 0.65 | ||
| 21 mm | 57.75 | 69.24 | 44.99 | 0.60 | 21 mm | 59.67 | 60.32 | 58.96 | 0.64 | ||
| 24 mm | 58.75 | 67.93 | 48.52 | 0.60 | 24 mm | 61.86 | 66.60 | 56.68 | 0.65 | ||
| 27 mm | 58.06 | 70.98 | 43.76 | 0.60 | 27 mm | 62.43 | 71.48 | 52.47 | 0.64 | ||
| 30 mm | 56.49 | 69.93 | 41.57 | 0.60 | 30 mm | 60.57 | 67.48 | 53.01 | 0.64 | ||
| Group | Tumor Size Criteria (cm) | Number of Patients (n = 217) (Recurrence/Non-Recurrence) | Median Tumor Size (cm) |
|---|---|---|---|
| Group 1 | <3 cm | 88 patients (35/53) | 2.22 cm (±0.48) |
| Group 2 | ≥3 cm and <5 cm | 83 patients (53/30) | 3.77 cm (±0.59) |
| Group 3 | ≥5 cm | 46 patients (26/20) | 6.78 cm (±1.8) |
| (a) | Group 1 (tumor size < 3cm) | |||||
| Classifier | ACC | SEN | SPEC | AUC | ||
| Intratumoral radiomic features | 53.70 | 39.92 | 59.25 | 0.47 | ||
| Peritumoral radiomic features | 3 mm | 58.81 | 52.58 | 65.24 | 0.61 | |
| 12 mm | 61.24 | 58.11 | 66.62 | 0.67 | ||
| Combined radiomic features | 21 mm | 66.2 | 53.94 | 80.78 | 0.70 | |
| 24 mm | 62.02 | 57.12 | 69.98 | 0.67 | ||
| (b) | Group 2 (3 cm ≤ tumor size < 5 cm) | |||||
| Classifier | ACC | SEN | SPEC | AUC | ||
| Intratumoral radiomic features | 75.96 | 85.13 | 49.29 | 0.68 | ||
| Peritumoral radiomic features | 18 mm | 66.44 | 73.59 | 55.95 | 0.70 | |
| 27 mm | 71.48 | 80.51 | 58.81 | 0.73 | ||
| Combined radiomic features | 3 mm | 70.43 | 83.14 | 47.81 | 0.75 | |
| 6 mm | 65.11 | 76.88 | 44.43 | 0.72 | ||
| (c) | Group 3 (5 cm ≤ tumor size) | |||||
| Classifier | ACC | SEN | SPEC | AUC | ||
| Intratumoral radiomic features | 63.40 | 82.67 | 42.50 | 0.63 | ||
| Peritumoral radiomic features | 3 mm | 61.86 | 82.00 | 32.50 | 0.66 | |
| 24 mm | 61.45 | 86.83 | 27.50 | 0.55 | ||
| Combined radiomic features | 3 mm | 61.73 | 83.67 | 42.50 | 0.71 | |
| 6 mm | 51.30 | 84.33 | 15.00 | 0.64 | ||
| Intratumoral Radiomic Features | |
| Category (#n) | Feature |
| Intensity (2) | Histogram 25% Percentile |
| Histogram 5% Percentile | |
| Texture (8) | GLCM Sum Variance |
| GLRLM Long Run Emphasis | |
| GLRLM Long Run High Gray-level Emphasis | |
| GLRLM Long Run Low Gray-level Emphasis | |
| GLRLM Low Gray-level Emphasis (std) | |
| GLRLM Short Run Emphasis (std) | |
| GLRLM Long Run High Gray-level Emphasis (std) | |
| LBP #08 | |
| Shape (3) | Major Axis Length |
| Major-minor Axis Length Ratio | |
| Convex Area | |
| Peritumoral Radiomic Features | |
| Category (#n) | Feature |
| Intensity (5) | Histogram 75% Percentile |
| Histogram 95% Percentile | |
| Histogram Std | |
| Histogram Min | |
| Histogram Mean | |
| Texture (4) | GLCM ASM (std) |
| GLRLM Long Run High Gray-level Emphasis | |
| GLRLM Run Percentage (std) | |
| GLRLM Short Run Low Gray-level Emphasis (std) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Jung, J.; Hong, H.; Kim, B.-S. Prediction of Two-Year Recurrence-Free Survival in Operable NSCLC Patients Using Radiomic Features from Intra- and Size-Variant Peri-Tumoral Regions on Chest CT Images. Diagnostics 2022, 12, 1313. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061313
Lee S, Jung J, Hong H, Kim B-S. Prediction of Two-Year Recurrence-Free Survival in Operable NSCLC Patients Using Radiomic Features from Intra- and Size-Variant Peri-Tumoral Regions on Chest CT Images. Diagnostics. 2022; 12(6):1313. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061313
Chicago/Turabian StyleLee, Soomin, Julip Jung, Helen Hong, and Bong-Seog Kim. 2022. "Prediction of Two-Year Recurrence-Free Survival in Operable NSCLC Patients Using Radiomic Features from Intra- and Size-Variant Peri-Tumoral Regions on Chest CT Images" Diagnostics 12, no. 6: 1313. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12061313