
Are We There Yet? The Value of Deep Learning in a Multicenter Setting for Response Prediction of Locally Advanced Rectal Cancer to Neoadjuvant Chemoradiotherapy

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
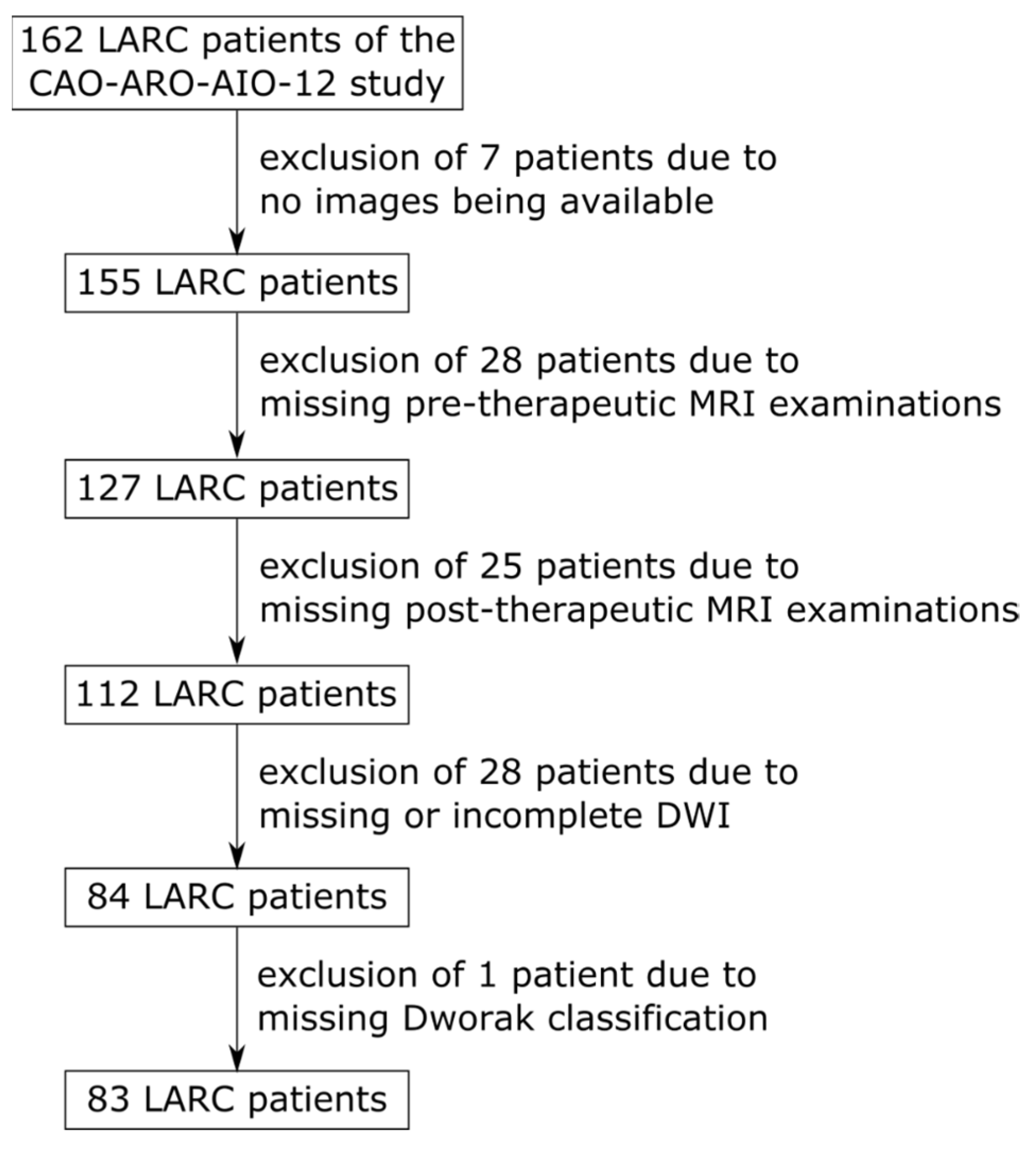
2.1. Patient Cohort
2.2. Image Acquisition and Radiologic Assessment
2.3. Pathological Assessment of Tumor Regression
2.4. Data Processing
2.5. Deep Learning Model
2.6. Training
2.7. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
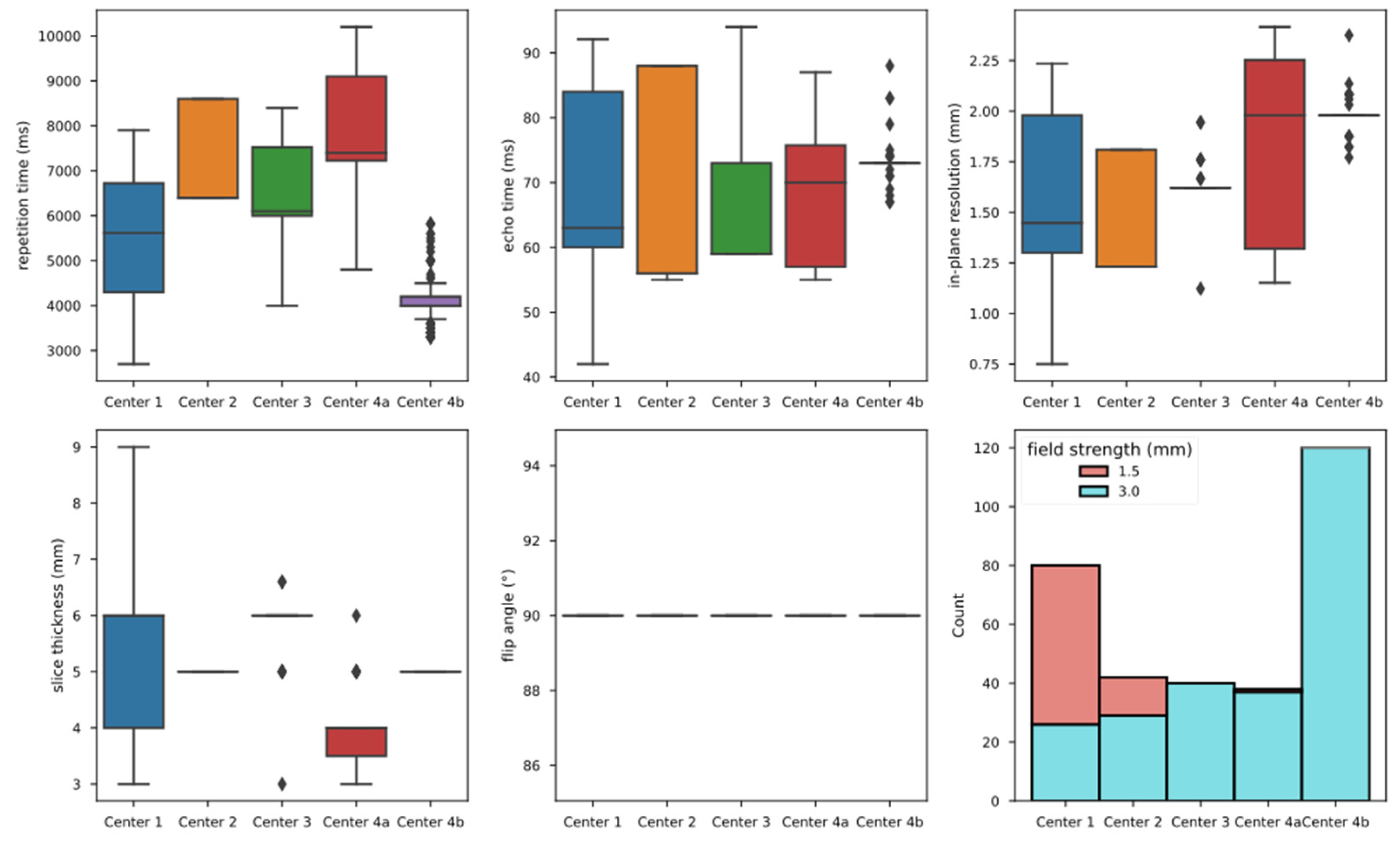
3.2. Imaging Characteristics

3.3. Data Processing
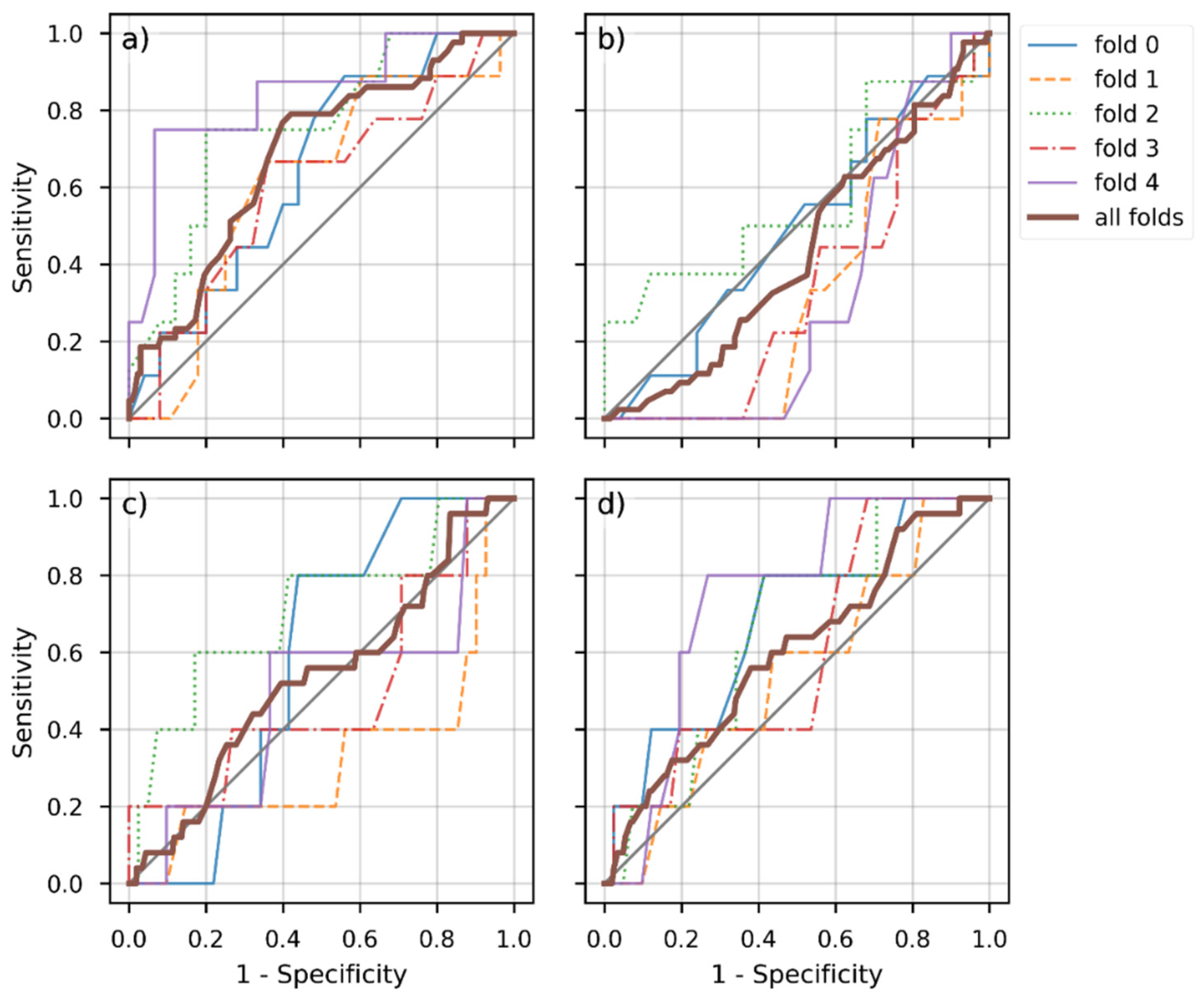
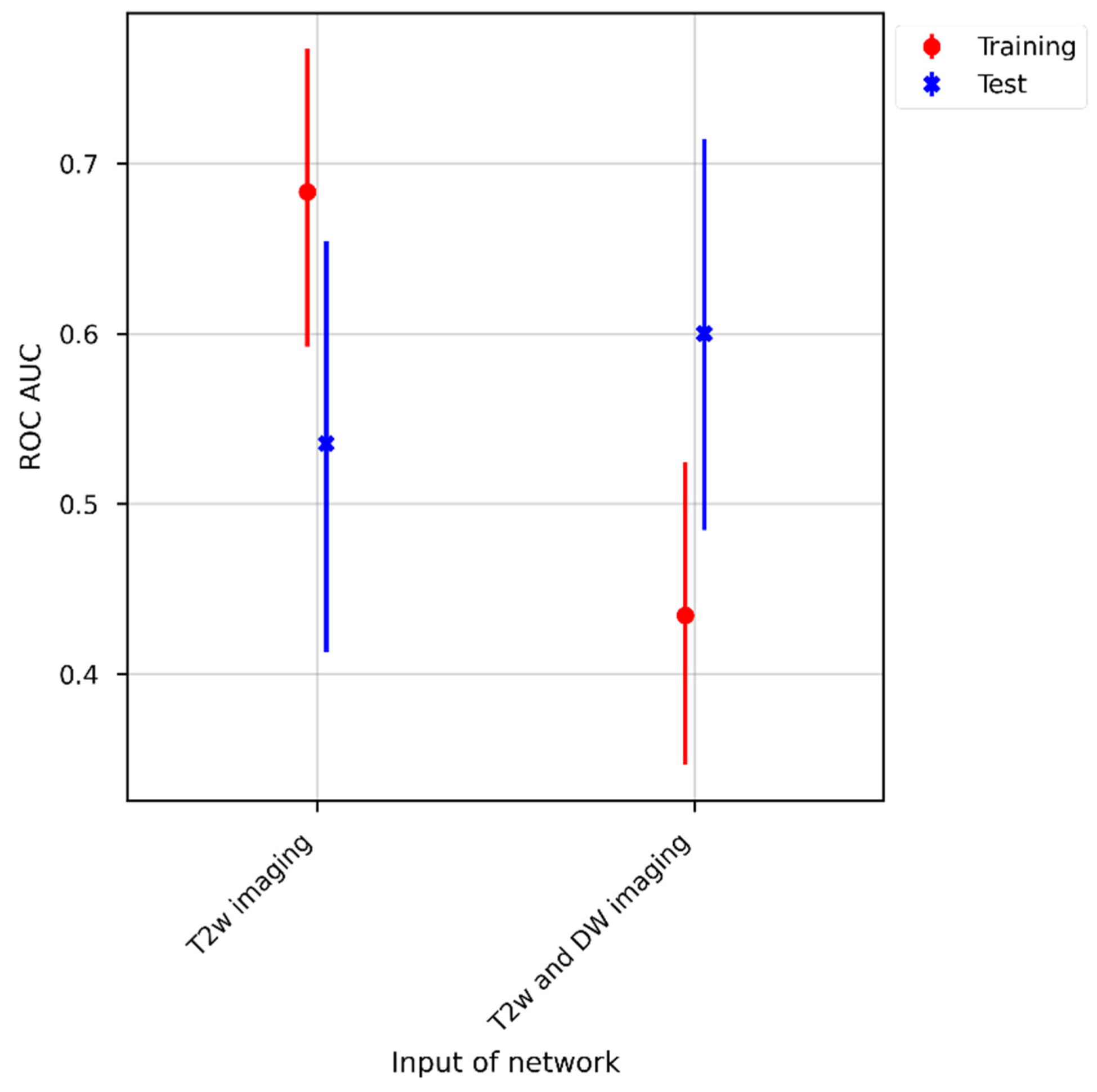
3.4. Model Performance
4. Discussion
- Data quality and uniformity are pivotal features to be addressed in clinical trials involving machine learning, requiring the development of a dedicated pre-processing pipeline.
- If no homogeneous data are available, the sample size for training the DL approach needs to be drastically increased to mitigate artifacts related to image inhomogeneity.
- Translating DL models into potentially useful clinical tools requires cross-center involvement of a multidisciplinary team.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut und die Gesellschaft der epidemiologischen Krebsregister in Deutschland e.V. (Ed.) Krebs in Deutschland für 2017/2018, 13rd ed.; Robert Koch-Institute: Berlin, Germany, 2021. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fokas, E.; Appelt, A.; Glynne-Jones, R.; Beets, G.; Perez, R.; Garcia-Aguilar, J.; Rullier, E.; Joshua Smith, J.; Marijnen, C.; Peters, F.P.; et al. International consensus recommendations on key outcome measures for organ preservation after (chemo)radiotherapy in patients with rectal cancer. Nat. Rev. Clin. Oncol. 2021, 18, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.-M. Using Deep Learning for MRI to Identify Responders to Chemoradiotherapy in Rectal Cancer. Radiology 2020, 296, 65–66. [Google Scholar] [CrossRef]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef]
- Loos, M.; Quentmeier, P.; Schuster, T.; Nitsche, U.; Gertler, R.; Keerl, A.; Kocher, T.; Friess, H.; Rosenberg, R. Effect of preoperative radio(chemo)therapy on long-term functional outcome in rectal cancer patients: A systematic review and meta-analysis. Ann. Surg. Oncol. 2013, 20, 1816–1828. [Google Scholar] [CrossRef]
- Rouanet, P. Tailored treatment strategy for locally advanced rectal carcinoma: Five-year results of the French phase II, randomized, multicenter GRECCAR4 trial. J. Clin. Oncol. 2020, 38, 4014. [Google Scholar] [CrossRef]
- van der Sande, M.E.; Beets, G.L.; Hupkens, B.J.; Breukink, S.O.; Melenhorst, J.; Bakers, F.C.; Lambregts, D.M.; Grabsch, H.I.; Beets-Tan, R.G.; Maas, M. Response assessment after (chemo)radiotherapy for rectal cancer: Why are we missing complete responses with MRI and endoscopy? Eur. J. Surg. Oncol. 2019, 45, 1011–1017. [Google Scholar] [CrossRef]
- Jang, J.K.; Choi, S.H.; Park, S.H.; Kim, K.W.; Kim, H.J.; Lee, J.S.; Kim, A.Y. MR tumor regression grade for pathological complete response in rectal cancer post neoadjuvant chemoradiotherapy: A systematic review and meta-analysis for accuracy. Eur. Radiol. 2020, 30, 2312–2323. [Google Scholar] [CrossRef]
- Gaa, T.; Neumann, W.; Sudarski, S.; Attenberger, U.I.; Schonberg, S.O.; Schad, L.R.; Zollner, F.G. Comparison of perfusion models for quantitative T1 weighted DCE-MRI of rectal cancer. Sci. Rep. 2017, 7, 12036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudarski, S.; Henzler, T.; Floss, T.; Gaa, T.; Meyer, M.; Haubenreisser, H.; Schoenberg, S.O.; Attenberger, U.I. Variability and Reproducibility of 3(rd)-generation dual-source dynamic volume perfusion CT Parameters in Comparison to MR-perfusion Parameters in Rectal Cancer. Sci. Rep. 2018, 8, 6868. [Google Scholar] [CrossRef] [PubMed]
- Attenberger, U.I.; Ong, M.M.; Rathmann, N.; Doyon, F.; Kienle, P.; Hofheinz, R.D.; Pilz, L.R.; Dinter, D.J.; Schoenberg, S.O.; Hausmann, D. mMRI at 3.0 T as an Evaluation Tool of Therapeutic Response to Neoadjuvant CRT in Patients with Advanced-stage Rectal Cancer. Anticancer Res. 2017, 37, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attenberger, U.I.; Pilz, L.R.; Morelli, J.N.; Hausmann, D.; Doyon, F.; Hofheinz, R.; Kienle, P.; Post, S.; Michaely, H.J.; Schoenberg, S.O.; et al. Multi-parametric MRI of rectal cancer-do quantitative functional MR measurements correlate with radiologic and pathologic tumor stages? Eur. J. Radiol. 2014, 83, 1036–1043. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, S.H.; Lee, S.J.; Jang, K.M.; Rhim, H. Locally advanced rectal cancer: Added value of diffusion-weighted MR imaging for predicting tumor clearance of the mesorectal fascia after neoadjuvant chemotherapy and radiation therapy. Radiology 2011, 260, 771–780. [Google Scholar] [CrossRef]
- Hötker, A.M.; Garcia-Aguilar, J.; Gollub, M.J. Multiparametric MRI of rectal cancer in the assessment of response to therapy: A systematic review. Dis. Colon Rectum 2014, 57, 790–799. [Google Scholar] [CrossRef]
- Mizukami, Y.; Ueda, S.; Mizumoto, A.; Sasada, T.; Okumura, R.; Kohno, S.; Takabayashi, A. Diffusion-weighted magnetic resonance imaging for detecting lymph node metastasis of rectal cancer. World J. Surg. 2011, 35, 895–899. [Google Scholar] [CrossRef]
- Le Bihan, D. Apparent diffusion coefficient and beyond: What diffusion MR imaging can tell us about tissue structure. Radiology 2013, 268, 318–322. [Google Scholar] [CrossRef]
- Intven, M.; Reerink, O.; Philippens, M.E. Diffusion-weighted MRI in locally advanced rectal cancer: Pathological response prediction after neo-adjuvant radiochemotherapy. Strahlenther. Onkol. 2013, 189, 117–122. [Google Scholar] [CrossRef]
- Jung, S.H.; Heo, S.H.; Kim, J.W.; Jeong, Y.Y.; Shin, S.S.; Soung, M.G.; Kim, H.R.; Kang, H.K. Predicting response to neoadjuvant chemoradiation therapy in locally advanced rectal cancer: Diffusion-weighted 3 Tesla MR imaging. J. Magn. Reason. Imaging 2012, 35, 110–116. [Google Scholar] [CrossRef]
- Dzik-Jurasz, A.; Domenig, C.; George, M.; Wolber, J.; Padhani, A.; Brown, G.; Doran, S. Diffusion MRI for prediction of response of rectal cancer to chemoradiation. Lancet 2002, 360, 307–308. [Google Scholar] [CrossRef]
- Cai, G.; Xu, Y.; Zhu, J.; Gu, W.L.; Zhang, S.; Ma, X.J.; Cai, S.J.; Zhang, Z. Diffusion-weighted magnetic resonance imaging for predicting the response of rectal cancer to neoadjuvant concurrent chemoradiation. World J. Gastroenterol. 2013, 19, 5520–5527. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, D.; Monguzzi, L.; Guerra, L.; Deponti, E.; Gardani, G.; Messa, C.; Sironi, S. Response to neoadjuvant therapy in locally advanced rectal cancer: Assessment with diffusion-weighted MR imaging and 18FDG PET/CT. Abdom. Imaging 2012, 37, 1032–1040. [Google Scholar] [CrossRef]
- DeVries, A.F.; Kremser, C.; Hein, P.A.; Griebel, J.; Krezcy, A.; Ofner, D.; Pfeiffer, K.P.; Lukas, P.; Judmaier, W. Tumor microcirculation and diffusion predict therapy outcome for primary rectal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 958–965. [Google Scholar] [CrossRef]
- Musio, D.; De Felice, F.; Magnante, A.L.; Ciolina, M.; De Cecco, C.N.; Rengo, M.; Redler, A.; Laghi, A.; Raffetto, N.; Tombolini, V. Diffusion-weighted magnetic resonance application in response prediction before, during, and after neoadjuvant radiochemotherapy in primary rectal cancer carcinoma. Biomed. Res. Int. 2013, 2013, 740195. [Google Scholar] [CrossRef] [PubMed]
- Monguzzi, L.; Ippolito, D.; Bernasconi, D.P.; Trattenero, C.; Galimberti, S.; Sironi, S. Locally advanced rectal cancer: Value of ADC mapping in prediction of tumor response to radiochemotherapy. Eur. J. Radiol. 2013, 82, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Curvo-Semedo, L.; Lambregts, D.M.; Maas, M.; Beets, G.L.; Caseiro-Alves, F.; Beets-Tan, R.G. Diffusion-weighted MRI in rectal cancer: Apparent diffusion coefficient as a potential noninvasive marker of tumor aggressiveness. J. Magn. Reason. Imaging 2012, 35, 1365–1371. [Google Scholar] [CrossRef]
- Barbaro, B.; Vitale, R.; Valentini, V.; Illuminati, S.; Vecchio, F.M.; Rizzo, G.; Gambacorta, M.A.; Coco, C.; Crucitti, A.; Persiani, R.; et al. Diffusion-weighted magnetic resonance imaging in monitoring rectal cancer response to neoadjuvant chemoradiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 594–599. [Google Scholar] [CrossRef]
- Elmi, A.; Hedgire, S.S.; Covarrubias, D.; Abtahi, S.M.; Hahn, P.F.; Harisinghani, M. Apparent diffusion coefficient as a non-invasive predictor of treatment response and recurrence in locally advanced rectal cancer. Clin. Radiol. 2013, 68, e524–e531. [Google Scholar] [CrossRef]
- Joye, I.; Deroose, C.M.; Vandecaveye, V.; Haustermans, K. The role of diffusion-weighted MRI and (18)F-FDG PET/CT in the prediction of pathologic complete response after radiochemotherapy for rectal cancer: A systematic review. Radiother. Oncol. 2014, 113, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Jin, C.; Yu, H.; Ke, J.; Ding, P.; Yi, Y.; Jiang, X.; Duan, X.; Tang, J.; Chang, D.T.; Wu, X.; et al. Predicting treatment response from longitudinal images using multi-task deep learning. Nat. Commun. 2021, 12, 1851. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Allgauer, M.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.L.; et al. Randomized Phase II Trial of Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: CAO/ARO/AIO-12. J. Clin. Oncol. 2019, 37, 3212–3222. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02363374 (accessed on 23 June 2022).
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ITK-SNAP. Available online: www.itksnap.org (accessed on 23 June 2022).
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int. J. Colorectal Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [Green Version]
- Lowekamp, B.C.; Chen, D.T.; Ibanez, L.; Blezek, D. The Design of SimpleITK. Front. Neuroinform. 2013, 7, 45. [Google Scholar] [CrossRef] [Green Version]
- Yaniv, Z.; Lowekamp, B.C.; Johnson, H.J.; Beare, R. SimpleITK Image-Analysis Notebooks: A Collaborative Environment for Education and Reproducible Research. J. Digit. Imaging 2018, 31, 290–303. [Google Scholar] [CrossRef] [Green Version]
- Avants, B.B.; Tustison, N.J.; Song, G.; Cook, P.A.; Klein, A.; Gee, J.C. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage 2011, 54, 2033–2044. [Google Scholar] [CrossRef] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Zhang, X.-Y.; Wang, L.; Zhu, H.-T.; Li, Z.-W.; Ye, M.; Li, X.-T.; Shi, Y.-J.; Zhu, H.-C.; Sun, Y.-S. Predicting Rectal Cancer Response to Neoadjuvant Chemoradiotherapy Using Deep Learning of Diffusion Kurtosis MRI. Radiology 2020, 296, 56–64. [Google Scholar] [CrossRef]
- Huizinga, W.; Poot, D.H.; Guyader, J.M.; Klaassen, R.; Coolen, B.F.; van Kranenburg, M.; van Geuns, R.J.; Uitterdijk, A.; Polfliet, M.; Vandemeulebroucke, J.; et al. PCA-based groupwise image registration for quantitative MRI. Med. Image Anal. 2016, 29, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Schurink, N.W.; van Kranen, S.R.; Roberti, S.; van Griethuysen, J.J.M.; Bogveradze, N.; Castagnoli, F.; El Khababi, N.; Bakers, F.C.H.; de Bie, S.H.; Bosma, G.P.T.; et al. Sources of variation in multicenter rectal MRI data and their effect on radiomics feature reproducibility. Eur. Radiol. 2022, 32, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, S.B.; Palombo, M.; Khoo, C.S.; Tax, C.M.W.; Tanno, R.; Alexander, D.C. Multi-stage Prediction Networks for Data Harmonization. In Medical Image Computing and Computer Assisted Intervention–MICCAI 2019; Springer: Cham, Switzerland, 2019; pp. 411–419. [Google Scholar]
- Cackowski, S.; Barbier, E.L.; Dojat, M.; Christen, T. ImUnity: A generalizable VAE-GAN solution for multicenter MR image harmonization. arXiv 2021, arXiv:2109.06756. [Google Scholar]
- Glocker, B.; Robinson, R.; Castro, D.C.; Dou, Q.; Konukoglu, E. Machine learning with multi-site imaging data: An empirical study on the impact of scanner effects. arXiv 2019, arXiv:1910.04597. [Google Scholar]
- Dutta, S.; Gros, E. Evaluation of the impact of deep learning architectural components selection and dataset size on a medical imaging task. In Medical Imaging 2018: Imaging Informatics for Healthcare, Research, and Applications; SPIE: Bellingham, WA, USA, 2018; Volume 10579. [Google Scholar]
- Raj, A.; Tollens, F.; Hansen, L.; Golla, A.-K.; Schad, L.R.; Nörenberg, D.; Zöllner, F.G. Deep Learning-Based Total Kidney Volume Segmentation in Autosomal Dominant Polycystic Kidney Disease Using Attention, Cosine Loss, and Sharpness Aware Minimization. Diagnostics 2022, 12, 1159. [Google Scholar] [CrossRef] [PubMed]
- Kohli, M.D.; Summers, R.M.; Geis, J.R. Medical Image Data and Datasets in the Era of Machine Learning—Whitepaper from the 2016 C-MIMI Meeting Dataset Session. J. Digit. Imaging 2017, 30, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Willemink, M.J.; Koszek, W.A.; Hardell, C.; Wu, J.; Fleischmann, D.; Harvey, H.; Folio, L.R.; Summers, R.M.; Rubin, D.L.; Lungren, M.P. Preparing Medical Imaging Data for Machine Learning. Radiology 2020, 295, 4–15. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Cohort | Validation Cohort | Test Cohort | Significant Differences | |||
|---|---|---|---|---|---|---|
| Characteristic | Center 1 | Center 2 | Center 3 | Center 4a | Center 4b | |
| Acquisition (years) | 2015–2018 | 2016–2017 | 2015–2017 | 2015–2017 | 2009–2013 | 0.00 |
| Age (mean ± std) | 60 ± 10 | 61 ± 11 | 60 ± 6 | 66 ± 6 | 64 ± 11 | 0.07 |
| Sex | 0.15 | |||||
| Male | 26 | 14 | 8 | 9 | 37 | |
| Female | 11 | 6 | 7 | 2 | 9 | |
| Pre-nCRT T-stage (MRI) | 0.02 | |||||
| T0 | 0 | 0 | 0 | 0 | 0 | |
| T1 | 0 | 0 | 0 | 0 | 0 | |
| T2 | 3 | 0 | 2 | 0 | 8 | |
| T3 | 28 | 1 | 11 | 5 | 38 | |
| T4 | 4 | 0 | 1 | 0 | 0 | |
| Not specified | 2 | 19 | 1 | 6 | 0 | |
| Pre-nCRT N-stage (MRI) | 0.00 | |||||
| N- | 2 | 2 | 0 | 1 | 25 | |
| N+ | 35 | 18 | 15 | 10 | 21 | |
| CRM (initial staging) | 0.06 | |||||
| Minimal distance to mesorectal fascia (MRF) in mm | 12 ± 9 | 2 ± 5 | 3 ± 3 | |||
| MRF involvement | 2 | 0 | 0 | 2 | 7 | |
| Not specified | 13 | 20 | 0 | 9 | 0 | |
| Tumor location | 0.0 | |||||
| lower third | 18 | 5 | 5 | 4 | 10 | |
| middle third | 13 | 9 | 10 | 5 | 25 | |
| upper third | 0 | 0 | 0 | 0 | 11 | |
| location not specified | 6 | 6 | 0 | 2 | 0 | |
| Post-nCRT T-stage (MRI) | 0.03 | |||||
| T0 | 1 | 0 | 3 | 0 | 0 | |
| T1 | 2 | 0 | 1 | 0 | 2 | |
| T2 | 13 | 0 | 1 | 0 | 27 | |
| T3 | 17 | 0 | 10 | 0 | 17 | |
| T4 | 4 | 0 | 0 | 1 | 0 | |
| Not specified | 0 | 20 | 0 | 10 | 0 | |
| Post-nCRT N-stage (MRI) | 0.68 | |||||
| N− | 17 | 0 | 2 | 0 | 39 | |
| N+ | 20 | 0 | 13 | 2 | 5 | |
| Not specified | 0 | 20 | 0 | 9 | 2 | |
| pCR | 0.15 | |||||
| pCR | 7 | 9 | 1 | 2 | 5 | |
| Non-pCR | 30 | 11 | 14 | 9 | 41 | |
| Time in days (mean ± std) | ||||||
| Initial Staging to OP | 146 ± 12 | 146 ± 11 | 142 ± 8 | 177 ± 35 | 123 ± 20 | 0.0 |
| Post-nCRT MRI to OP | 13 ± 10 | 7 ± 3 | 8 ± 3 | 32 ± 15 | 29 ± 14 | 0.0 |
| Vendor | Model Name | Tesla | Number of Patients before nCRT | Number of Patients after nCRT | |
|---|---|---|---|---|---|
| Center 1 | Siemens | Prisma_fit | 3.0 | 6 | 18 |
| Siemens | Avanto | 1.5 | 14 | 0 | |
| Siemens | Avanto_fit | 1.5 | 2 | 14 | |
| Siemens | SymphonyTim | 1.5 | 12 | 1 | |
| Siemens | Aera | 1.5 | 1 | 3 | |
| Siemens | Espree | 1.5 | 0 | 1 | |
| Philips | Ingenia | 1.5 | 1 | 0 | |
| Siemens | Spectra | 3.0 | 1 | 0 | |
| Center 2 | Siemens | Skyra | 3.0 | 17 | 10 |
| Siemens | Avanto | 1.5 | 3 | 10 | |
| Center 3 | Siemens | Prisma_fit | 3.0 | 11 | 9 |
| Siemens | Skyra | 3.0 | 4 | 6 | |
| Center 4a | Siemens | Skyra | 3.0 | 4 | 8 |
| Siemens | TrioTim | 3.0 | 6 | 3 | |
| Siemens | Avanto | 1.5 | 1 | 0 | |
| Center 4b | Siemens | TrioTim | 1.5 | 46 | 46 |
| Training T2w | Test T2w | Training DWI | Test DWI | |
|---|---|---|---|---|
| Slice thickness (mm) | 3.3 ± 0.5 | 3.1 ± 0.2 | 5.1 ± 1.1 | 5.0 ± 0.0 |
| Repetition time (ms) | 4994.9 ± 1913.5 | 3971.5 ± 708.1 | 6463.1 ± 1539.1 | 4121.9 ± 562.7 |
| Pixel bandwidth (Hz) | 215.9 ± 48.9 | 201.6 ± 8.8 | 1792.5 ± 351.6 | 1735.0 ± 8.3 |
| Flip angle (°) | 137.0 ± 16.5 | 148.7 ± 5.6 | 90.0 ± 0.0 | 90.0 ± 0.0 |
| Echo time (ms) | 97.8 ± 14.5 | 101.9 ± 4.7 | 67.2 ± 13.4 | 73.2 ± 2.2 |
| Field strength (T) | 2.5 ± 0.7 | 3.0 ± 0.0 | 2.5 ± 0.7 | 3.0 ± 0.0 |
| In-plane resolution (mm) | 0.6 ± 0.2 | 0.6 ± 0.0 | 1.6 ± 0.4 | 2.0 ± 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wichtmann, B.D.; Albert, S.; Zhao, W.; Maurer, A.; Rödel, C.; Hofheinz, R.-D.; Hesser, J.; Zöllner, F.G.; Attenberger, U.I. Are We There Yet? The Value of Deep Learning in a Multicenter Setting for Response Prediction of Locally Advanced Rectal Cancer to Neoadjuvant Chemoradiotherapy. Diagnostics 2022, 12, 1601. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071601
Wichtmann BD, Albert S, Zhao W, Maurer A, Rödel C, Hofheinz R-D, Hesser J, Zöllner FG, Attenberger UI. Are We There Yet? The Value of Deep Learning in a Multicenter Setting for Response Prediction of Locally Advanced Rectal Cancer to Neoadjuvant Chemoradiotherapy. Diagnostics. 2022; 12(7):1601. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071601
Chicago/Turabian StyleWichtmann, Barbara D., Steffen Albert, Wenzhao Zhao, Angelika Maurer, Claus Rödel, Ralf-Dieter Hofheinz, Jürgen Hesser, Frank G. Zöllner, and Ulrike I. Attenberger. 2022. "Are We There Yet? The Value of Deep Learning in a Multicenter Setting for Response Prediction of Locally Advanced Rectal Cancer to Neoadjuvant Chemoradiotherapy" Diagnostics 12, no. 7: 1601. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071601