
The Accelerated Right Ventricular Failure in Fetal Anemia in the Presence of Restrictive Foramen Ovale


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
- In anemia, the heart is usually enlarged globally and equally without disproportion [17].
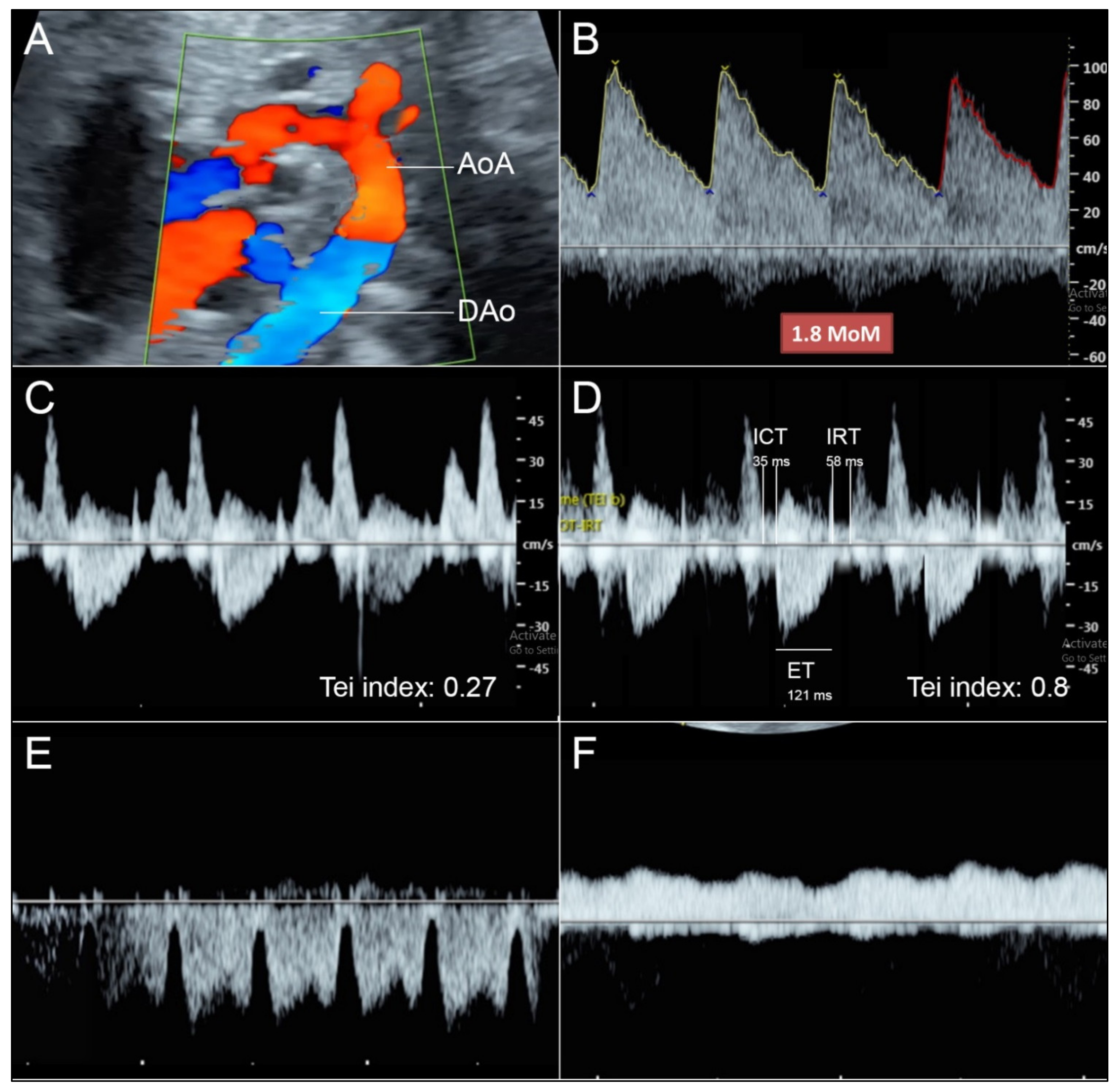
- Reversed flow in aortic arch is commonly seen in hypoplastic left heart or aortic stenosis but in this case the flow crossing the aortic valve shows normal laminar flow.
- Reversed flow in aortic arch is different from that seen in fetal growth restriction (FGR), which usually shows increased afterload (abnormal umbilical blood flow).
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uzun, O.; Babaoglu, K.; Ayhan, Y.I.; Moselhi, M.; Rushworth, F.; Morris, S.; Beattie, B.; Wiener, J.; Lewis, M.J. Diagnostic ultrasound features and outcome of restrictive foramen ovale in fetuses with structurally normal hearts. Pediatric Cardiol. 2014, 35, 943–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozkaya, V.; Oskovi-Kaplan, Z.A.; Engin-Ustun, Y. Atrial septal aneurysm in pregnancy: Echocardiography and obstetric outcomes. J. Perinat. Med. 2020, 48, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Haddad, S.; Degani, S.; Rahav, D.; Ohel, G. The antenatal diagnosis of fetal atrial septal aneurysm. Gynecol. Obs. Investig. 1996, 41, 27–29. [Google Scholar] [CrossRef]
- Hagen, A.; Albig, M.; Schmitz, L.; Hopp, H.; van Baalen, A.; Becker, R.; Entezami, M. Prenatal diagnosis of isolated foramen ovale obstruction. A report of two cases. Fetal Diagn. Ther. 2005, 20, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Hung, J.H.; Lu, J.H.; Hung, C.Y. Prenatal diagnosis of atrial septal aneurysm. J. Clin. Ultrasound 2008, 36, 51–52. [Google Scholar] [CrossRef]
- Pinette, M.G.; Pan, Y.; Pinette, S.G.; Blackstone, J.; Stubblefield, P.G. Fetal atrial septal aneurysm. Prenatal diagnosis by ultrasonography. J. Reprod. Med. 1997, 42, 459–462. [Google Scholar] [PubMed]
- Ozcelik, N.; Atalay, S.; Tutar, E.; Ekici, F. Prevalence of interatrial septal aneurysm in newborns and their natural course. Pediatric Cardiol. 2006, 27, 343–346. [Google Scholar] [CrossRef]
- Toro, L.; Weintraub, R.G.; Shiota, T.; Sahn, D.J.; Sahn, C.; McDonald, R.W.; Rice, M.J.; Hagen-Ansert, S. Relation between persistent atrial arrhythmias and redundant septum primum flap (atrial septal aneurysm) in fetuses. Am. J. Cardiol. 1994, 73, 711–713. [Google Scholar] [CrossRef]
- Stewart, P.A.; Wladimiroff, J.W. Fetal atrial arrhythmias associated with redundancy/aneurysm of the foramen ovale. J. Clin. Ultrasound 1988, 16, 643–650. [Google Scholar] [CrossRef]
- Channing, A.; Szwast, A.; Natarajan, S.; Degenhardt, K.; Tian, Z.; Rychik, J. Maternal hyperoxygenation improves left heart filling in fetuses with atrial septal aneurysm causing impediment to left ventricular inflow. Ultrasound Obs. Gynecol. 2015, 45, 664–669. [Google Scholar] [CrossRef]
- Santos, A.C.; Branco, M.; Martins, P. Fetal atrial septal aneurysm: A differential diagnosis of aortic arch retrograde flow. BMJ Case Rep. 2020, 13, e232773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.; Zhang, Y.; Han, J.; Liu, X.; Ge, S.; He, Y. Isolated premature restriction or closure of foramen ovale in fetuses: Echocardiographic characteristics and outcome. Echocardiography 2018, 35, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Tongsong, T.; Tongprasert, F.; Srisupundit, K.; Luewan, S. Venous Doppler studies in low-output and high-output hydrops fetalis. Am. J. Obstet. Gynecol. 2010, 203, 488.e1–488.e6. [Google Scholar] [CrossRef] [PubMed]
- Thammavong, K.; Luewan, S.; Wanapirak, C.; Tongsong, T. Ultrasound Features of Fetal Anemia Lessons from Hemoglobin Bart Disease. J. Ultrasound Med. 2021, 40, 659–674. [Google Scholar] [CrossRef] [PubMed]
- Thammavong, K.; Luewan, S.; Jatavan, P.; Tongsong, T. Foetal haemodynamic response to anaemia. ESC Heart Fail. 2020, 7, 3473–3482. [Google Scholar] [CrossRef]
- Mari, G.; Deter, R.L.; Carpenter, R.L.; Rahman, F.; Zimmerman, R.; Moise, K.J., Jr.; Dorman, K.F.; Ludomirsky, A.; Gonzalez, R.; Gomez, R.; et al. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red-cell alloimmunization. Collaborative Group for Doppler Assessment of the Blood Velocity in Anemic Fetuses. N. Engl. J. Med. 2000, 342, 9–14. [Google Scholar] [CrossRef]
- Chankhunaphas, W.; Tongsong, T.; Tongprasert, F.; Srisupundit, K.; Luewan, S.; Traisrisilp, K.; Jatavan, P. Comparison of the Performances of Middle Cerebral Artery Peak Systolic Velocity and Cardiothoracic Diameter Ratio in Predicting Fetal Anemia: Using Fetal Hemoglobin Bart’s Disease as a Study Model. Fetal Diagn. Ther. 2021, 48, 738–745. [Google Scholar] [CrossRef]
- Ramaswamy, P.; Greenstein, G.; Friedman, D.; Burgess, T.; Haberman, S. Enhanced coronary blood flow and abnormal blood flow in the aortic isthmus in severe fetal anemia. Pediatric Cardiol. 2004, 25, 157–159. [Google Scholar] [CrossRef]
- Singh, P.; Swanson, T. Acute and chronic fetal anemia as a result of fetomaternal hemorrhage. Case. Rep. Obs. Gynecol. 2014, 2014, 296463. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, H.M. Response of the fetal heart to changes in load: From hyperplasia to heart failure. Heart 2005, 91, 871–873. [Google Scholar] [CrossRef] [Green Version]
- Nowlen, T.T.; Ayres, N.A.; Kearney, D.L.; Nihill, M.R.; Grifka, R.G. Premature closure of the foramen ovale associated with aortic stenosis, left ventricular dilation with thrombus, and early mortality. Am. J. Cardiol. 2000, 85, 1159–1161. [Google Scholar] [CrossRef]
- Jensen, A.; Roman, C.; Rudolph, A.M. Effects of reducing uterine blood flow on fetal blood flow distribution and oxygen delivery. J. Dev. Physiol. 1991, 15, 309–323. [Google Scholar] [PubMed]
- Itskovitz, J.; LaGamma, E.F.; Rudolph, A.M. Effects of cord compression on fetal blood flow distribution and O2 delivery. Am. J. Physiol. 1987, 252, H100–H109. [Google Scholar] [CrossRef] [PubMed]
- Mäkikallio, K.; Jouppila, P.; Räsänen, J. Retrograde aortic isthmus net blood flow and human fetal cardiac function in placental insufficiency. Ultrasound Obs. Gynecol. 2003, 22, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, A.M. Aortopulmonary transposition in the fetus: Speculation on pathophysiology and therapy. Pediatr. Res. 2007, 61, 375–380. [Google Scholar] [CrossRef] [Green Version]
- Maršál, K. Physiological adaptation of the growth-restricted fetus. Best Pract. Res. Clin. Obs. Gynaecol. 2018, 49, 37–52. [Google Scholar] [CrossRef]
- Rizzo, G.; Arduini, D. Fetal cardiac function in intrauterine growth retardation. Am. J. Obs. Gynecol. 1991, 165, 876–882. [Google Scholar] [CrossRef]
- Duan, A.Q.; Darby, J.R.T.; Soo, J.Y.; Lock, M.C.; Zhu, M.Y.; Flynn, L.V.; Perumal, S.R.; Macgowan, C.K.; Selvanayagam, J.B.; Morrison, J.L.; et al. Feasibility of phase-contrast cine magnetic resonance imaging for measuring blood flow in the sheep fetus. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2019, 317, R780–R792. [Google Scholar] [CrossRef]
- Ryd, D.; Sun, L.; Steding-Ehrenborg, K.; Bidhult, S.; Kording, F.; Ruprecht, C.; Macgowan, C.K.; Seed, M.; Aletras, A.H.; Arheden, H.; et al. Quantification of blood flow in the fetus with cardiovascular magnetic resonance imaging using Doppler ultrasound gating: Validation against metric optimized gating. J. Cardiovasc. Magn. Reson. 2019, 21, 74. [Google Scholar] [CrossRef] [Green Version]
- Seed, M.; van Amerom, J.F.; Yoo, S.J.; Al Nafisi, B.; Grosse-Wortmann, L.; Jaeggi, E.; Jansz, M.S.; Macgowan, C.K. Feasibility of quantification of the distribution of blood flow in the normal human fetal circulation using CMR: A cross-sectional study. J. Cardiovasc. Magn. Reson. 2012, 14, 79. [Google Scholar] [CrossRef] [Green Version]
- Prsa, M.; Sun, L.; van Amerom, J.; Yoo, S.J.; Grosse-Wortmann, L.; Jaeggi, E.; Macgowan, C.; Seed, M. Reference ranges of blood flow in the major vessels of the normal human fetal circulation at term by phase-contrast magnetic resonance imaging. Circ. Cardiovasc. Imaging 2014, 7, 663–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamurthy, U.; Yadav, B.K.; Jella, P.K.; Haacke, E.M.; Hernandez-Andrade, E.; Mody, S.; Yeo, L.; Hassan, S.S.; Romero, R.; Neelavalli, J. Quantitative Flow Imaging in Human Umbilical Vessels in Utero Using Nongated 2D Phase Contrast MRI. J. Magn. Reson. Imaging 2018, 48, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Al Nafisi, B.; van Amerom, J.F.; Forsey, J.; Jaeggi, E.; Grosse-Wortmann, L.; Yoo, S.J.; Macgowan, C.K.; Seed, M. Fetal circulation in left-sided congenital heart disease measured by cardiovascular magnetic resonance: A case-control study. J. Cardiovasc. Magn. Reson. 2013, 15, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porayette, P.; van Amerom, J.F.; Yoo, S.J.; Jaeggi, E.; Macgowan, C.K.; Seed, M. MRI shows limited mixing between systemic and pulmonary circulations in foetal transposition of the great arteries: A potential cause of in utero pulmonary vascular disease. Cardiol. Young 2015, 25, 737–744. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.; Luo, Y.; Zeng, S.; Zhou, J.; Xu, G.; Yang, J. Evaluation of fetal foramen ovale blood flow by pulsed Doppler ultrasonography combined with spatiotemporal image correlation: To define the normal reference range of fetal foramen ovale blood volume for each gestational age: A cross-sectional study. Cardiovasc. Ultrasound 2021, 19, 18. [Google Scholar] [CrossRef]
- Quartermain, M.D.; Cohen, M.S.; Dominguez, T.E.; Tian, Z.; Donaghue, D.D.; Rychik, J. Left ventricle to right ventricle size discrepancy in the fetus: The presence of critical congenital heart disease can be reliably predicted. J. Am. Soc. Echocardiogr. 2009, 22, 1296–1301. [Google Scholar] [CrossRef]
- Ferraz, M.M.; Araújo, F.D.V.; Carvalho, P.R.N.; Sá, R.A.M. Aortic Isthmus Doppler Velocimetry in Fetuses with Intrauterine Growth Restriction: A Literature Review. Rev. Bras. Ginecol. Obs. 2020, 42, 289–296. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luewan, S.; Tongprasert, F.; Srisupundit, K.; Tongsong, T. The Accelerated Right Ventricular Failure in Fetal Anemia in the Presence of Restrictive Foramen Ovale. Diagnostics 2022, 12, 1646. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071646
Luewan S, Tongprasert F, Srisupundit K, Tongsong T. The Accelerated Right Ventricular Failure in Fetal Anemia in the Presence of Restrictive Foramen Ovale. Diagnostics. 2022; 12(7):1646. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071646
Chicago/Turabian StyleLuewan, Suchaya, Fuanglada Tongprasert, Kasemsri Srisupundit, and Theera Tongsong. 2022. "The Accelerated Right Ventricular Failure in Fetal Anemia in the Presence of Restrictive Foramen Ovale" Diagnostics 12, no. 7: 1646. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071646