
Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
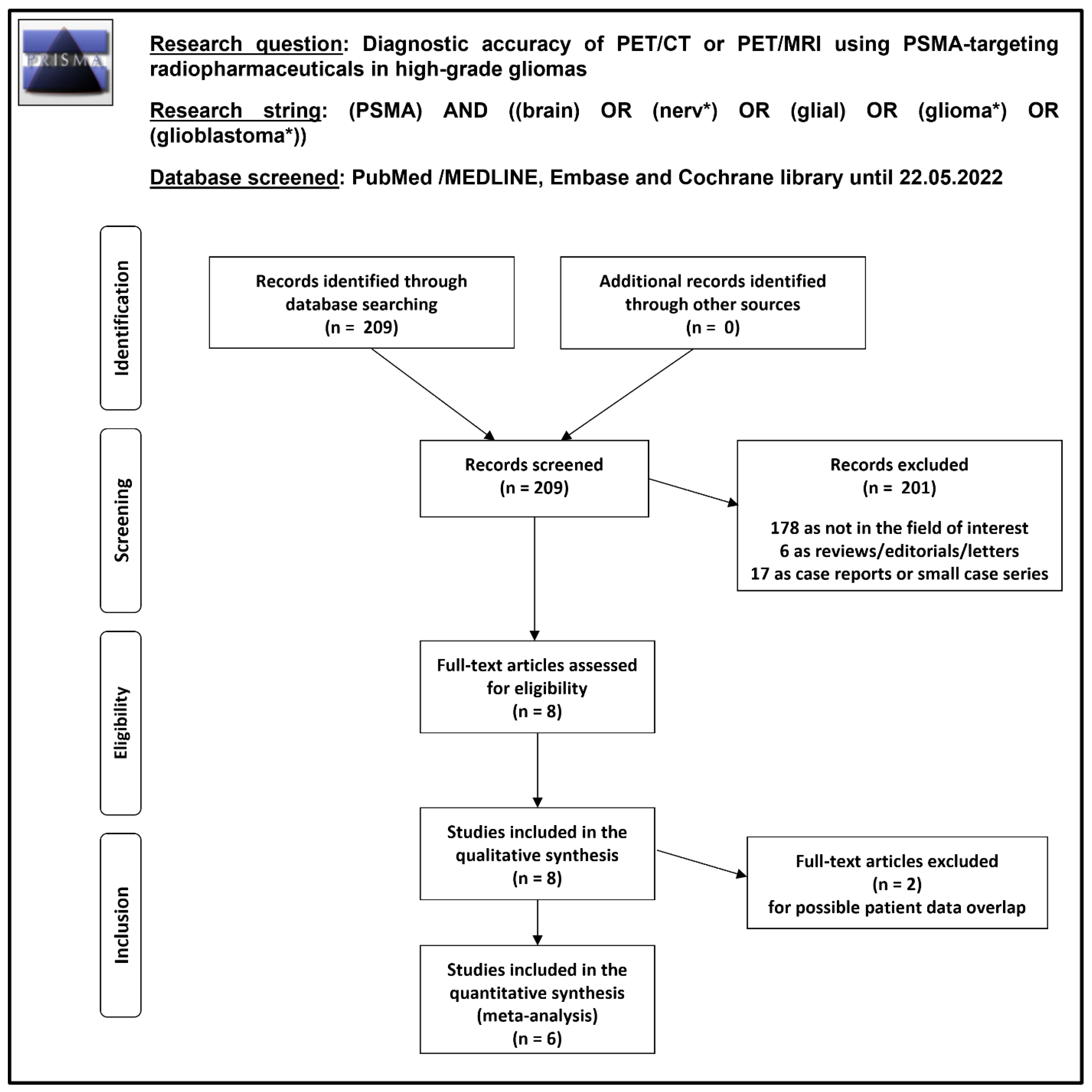
2.2. Literature Search Strategy and Information Sources
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Collection Process and Data Extraction
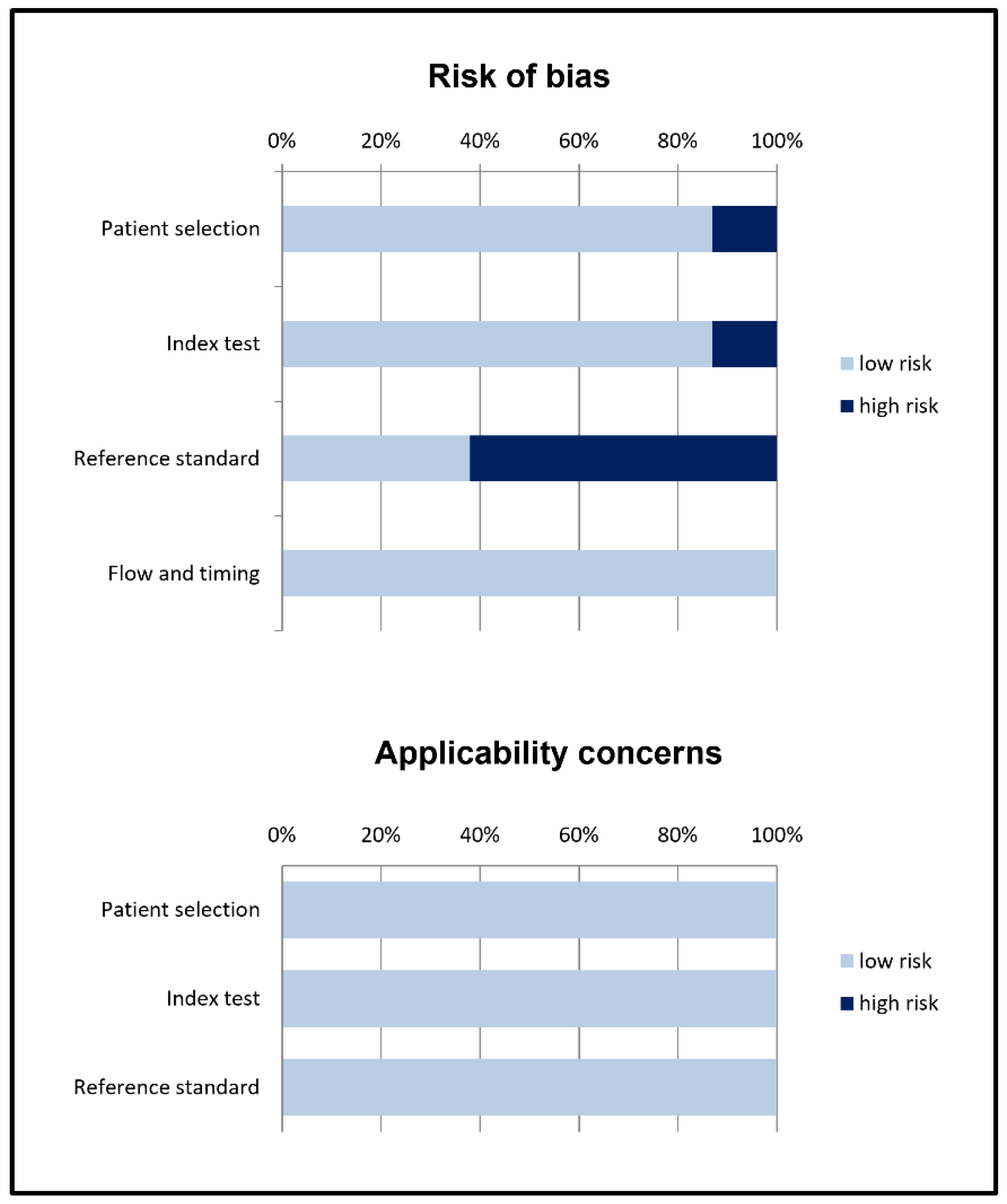
2.6. Quality Assessment
2.7. Statistical Analysis and Diagnostic Accuracy Measures
2.8. Additional Analyses
3. Results
3.1. Literature Search and Study Selection
3.2. Study Characteristics
3.3. Risk of Bias and Applicability
3.4. Results of Individual Studies (Qualitative Synthesis)
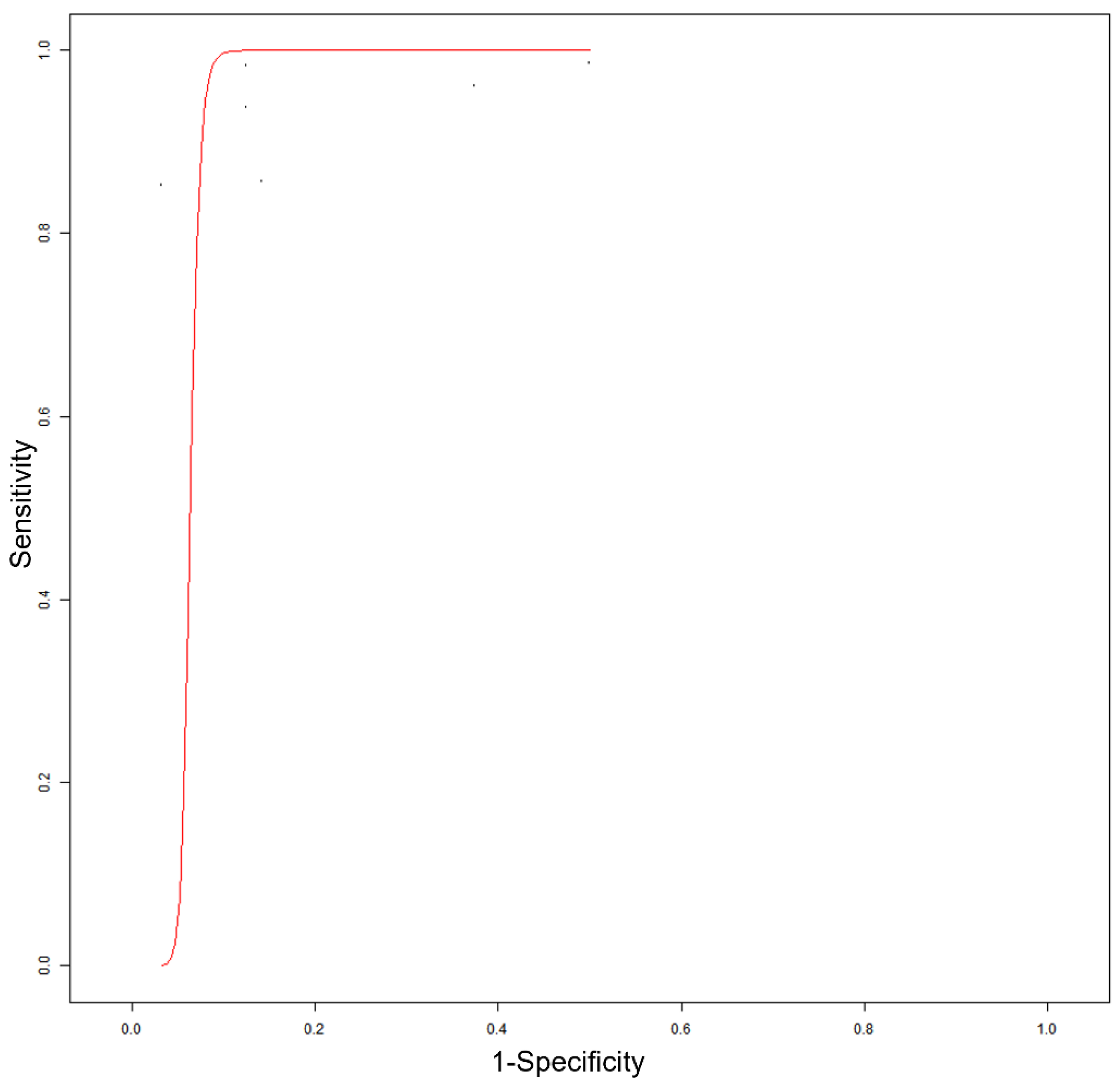
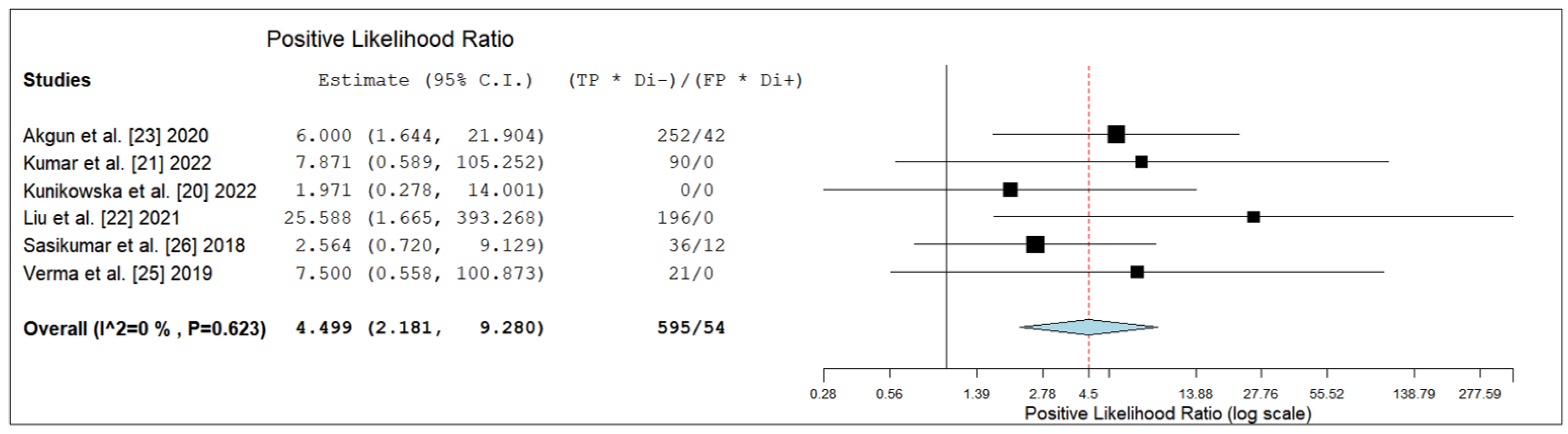
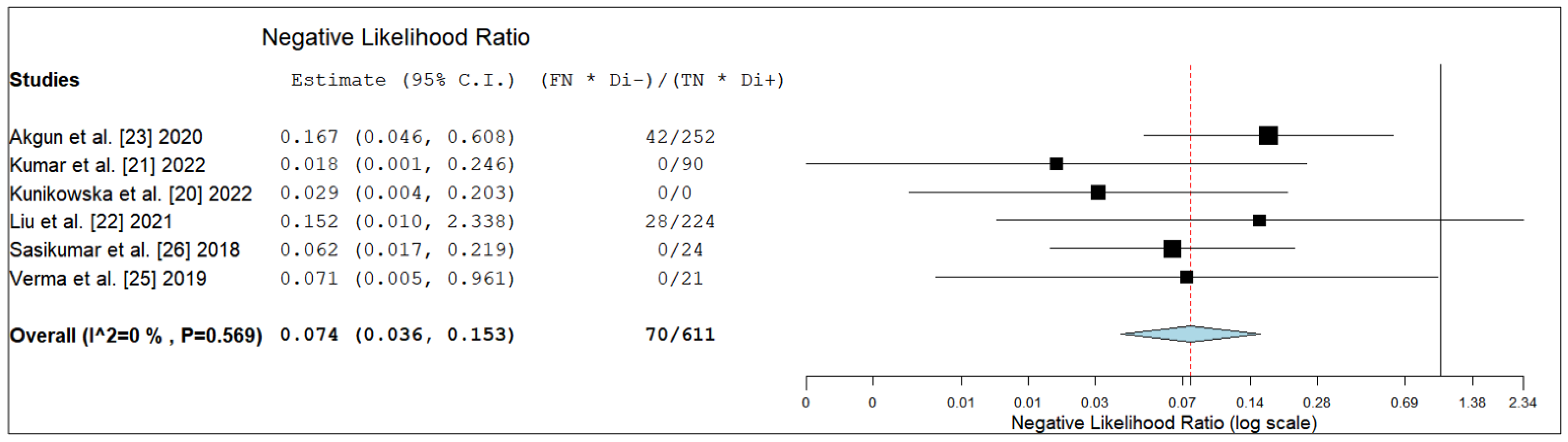
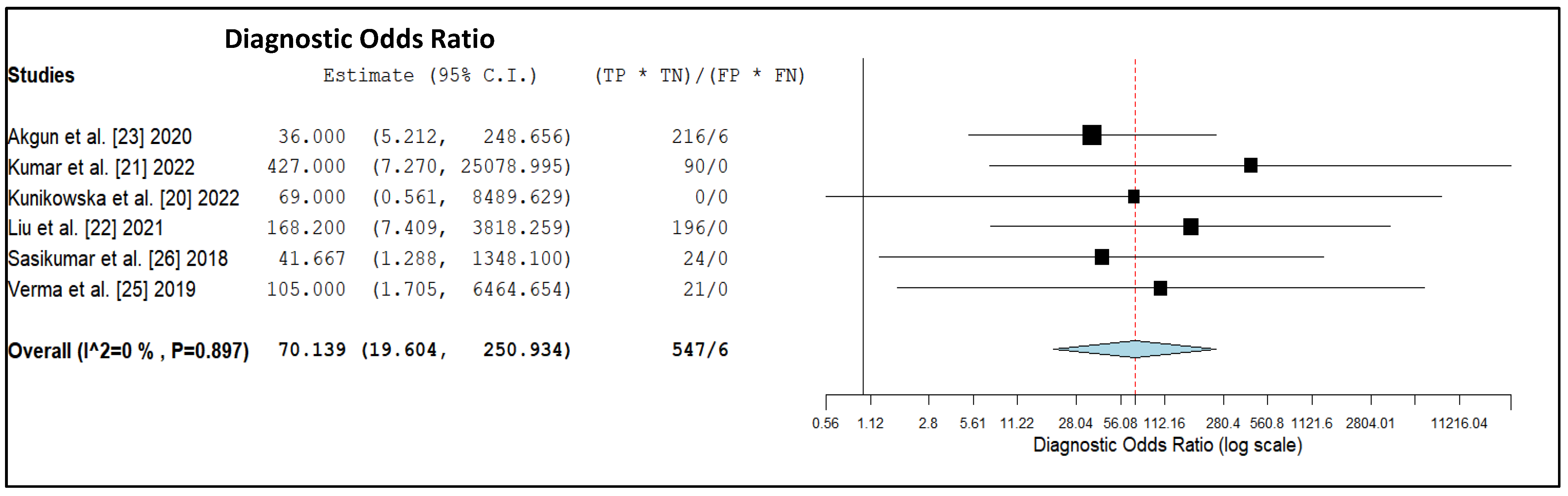
3.5. Meta-Analysis (Quantitative Synthesis)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Francis, S.S.; Ostrom, Q.T.; Cote, D.J.; Smith, T.R.; Claus, E.; Barnholtz-Sloan, J.S. The Epidemiology of Central Nervous System Tumors. Hematol. Oncol. Clin. N. Am. 2022, 36, 23–42. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Komori, T. Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System. Lab. Investig. 2022, 102, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Xue, C.; Ke, X.; Zhou, J. Treatment Response and Prognosis Evaluation in High-Grade Glioma: An Imaging Review Based on MRI. J. Magn. Reason. Imaging 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; la Fougère, C.; Langen, K.J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef] [Green Version]
- Piccardo, A.; Albert, N.L.; Borgwardt, L.; Fahey, F.H.; Hargrave, D.; Galldiks, N.; Jehanno, N.; Kurch, L.; Law, I.; Lim, R.; et al. Joint EANM/SIOPE/RAPNO practice guidelines/SNMMI procedure standards for imaging of paediatric gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2022. ahead of print. [Google Scholar] [CrossRef]
- Treglia, G.; Muoio, B.; Trevisi, G.; Mattoli, M.V.; Albano, D.; Bertagna, F.; Giovanella, L. Diagnostic Performance and Prognostic Value of PET/CT with Different Tracers for Brain Tumors: A Systematic Review of Published Meta-Analyses. Int. J. Mol. Sci. 2019, 20, 4669. [Google Scholar] [CrossRef] [Green Version]
- Neels, O.C.; Kopka, K.; Liolios, C.; Afshar-Oromieh, A. Radiolabeled PSMA Inhibitors. Cancers 2021, 13, 6255. [Google Scholar] [CrossRef] [PubMed]
- Mokoala, K.; Lawal, I.; Lengana, T.; Kgatle, M.; Giesel, F.L.; Vorster, M.; Sathekge, M. PSMA Theranostics: Science and Practice. Cancers 2021, 13, 3904. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, S.; Pizzuto, D.A.; Treglia, G. Diagnostic Performance of PET Imaging Using Different Radiopharmaceuticals in Prostate Cancer According to Published Meta-Analyses. Cancers 2020, 12, 2153. [Google Scholar] [CrossRef]
- Zhang, H.; Koumna, S.; Pouliot, F.; Beauregard, J.M.; Kolinsky, M. PSMA Theranostics: Current Landscape and Future Outlook. Cancers 2021, 13, 4023. [Google Scholar] [CrossRef]
- Kaewput, C.; Vinjamuri, S. Update of PSMA Theranostics in Prostate Cancer: Current Applications and Future Trends. J. Clin. Med. 2022, 11, 2738. [Google Scholar] [CrossRef]
- Traub-Weidinger, T.; Poetsch, N.; Woehrer, A.; Klebermass, E.M.; Bachnik, T.; Preusser, M.; Mischkulnig, M.; Kiesel, B.; Widhalm, G.; Mitterhauser, M.; et al. PSMA Expression in 122 Treatment Naive Glioma Patients Related to Tumor Metabolism in 11C-Methionine PET and Survival. J. Pers. Med. 2021, 11, 624. [Google Scholar] [CrossRef] [PubMed]
- Bertagna, F.; Albano, D.; Cerudelli, E.; Gazzilli, M.; Giubbini, R.; Treglia, G. Potential of Radiolabeled PSMA PET/CT or PET/MRI Diagnostic Procedures in Gliomas/Glioblastomas. Curr. Radiopharm. 2020, 13, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Stopa, B.M.; Crowley, J.; Juhász, C.; Rogers, C.M.; Witcher, M.R.; Kiser, J.W. Prostate-Specific Membrane Antigen as Target for Neuroimaging of Central Nervous System Tumors. Mol. Imaging 2022, 2022, 5358545. [Google Scholar] [CrossRef] [PubMed]
- Van de Wiele, C.; Sathekge, M.; de Spiegeleer, B.; de Jonghe, P.J.; Beels, L.; Maes, A. PSMA-Targeting Positron Emission Agents for Imaging Solid Tumors Other Than Non-Prostate Carcinoma: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 4886. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; The PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Kunikowska, J.; Czepczyński, R.; Pawlak, D.; Koziara, H.; Pełka, K.; Królicki, L. Expression of glutamate carboxypeptidase II in the glial tumor recurrence evaluated in vivo using radionuclide imaging. Sci. Rep. 2022, 12, 652. [Google Scholar] [CrossRef]
- Kumar, A.; ArunRaj, S.T.; Bhullar, K.; Haresh, K.P.; Gupta, S.; Ballal, S.; Yadav, M.; Singh, M.; Damle, N.A.; Garg, A.; et al. Ga-68 PSMA PET/CT in recurrent high-grade gliomas: Evaluating PSMA expression in vivo. Neuroradiology 2022, 64, 969–979. [Google Scholar] [CrossRef]
- Liu, D.; Cheng, G.; Ma, X.; Wang, S.; Zhao, X.; Zhang, W.; Yang, W.; Wang, J. PET/CT using (68) Ga-PSMA-617 versus (18) F-fluorodeoxyglucose to differentiate low- and high-grade gliomas. J. Neuroimaging 2021, 31, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Akgun, E.; Akgun, M.Y.; Selçuk, H.H.; Uzan, M.; Sayman, H.B. (68)Ga PSMA PET/MR in the differentiation of low and high grade gliomas: Is (68)Ga PSMA PET/MRI useful to detect brain gliomas? Eur. J. Radiol. 2020, 130, 109199. [Google Scholar] [CrossRef] [PubMed]
- Kunikowska, J.; Kuliński, R.; Muylle, K.; Koziara, H.; Królicki, L. 68Ga-Prostate-Specific Membrane Antigen-11 PET/CT: A New Imaging Option for Recurrent Glioblastoma Multiforme? Clin. Nucl. Med. 2020, 45, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Malhotra, G.; Goel, A.; Rakshit, S.; Chandak, A.; Chedda, R.; Banerjee, S.; Asopa, R.V. Differential Uptake of 68Ga-PSMA-HBED-CC (PSMA-11) in Low-Grade Versus High-Grade Gliomas in Treatment-Naive Patients. Clin. Nucl. Med. 2019, 44, e318–e322. [Google Scholar] [CrossRef] [PubMed]
- Sasikumar, A.; Kashyap, R.; Joy, A.; Charan Patro, K.; Bhattacharya, P.; Reddy Pilaka, V.K.; Oommen, K.E.; Pillai, M.R.A. Utility of 68Ga-PSMA-11 PET/CT in Imaging of Glioma-A Pilot Study. Clin. Nucl. Med. 2018, 43, e304–e309. [Google Scholar] [CrossRef]
- Sasikumar, A.; Joy, A.; Pillai, M.R.; Nanabala, R.; Anees, K.M.; Jayaprakash, P.G.; Madhavan, J.; Nair, S. Diagnostic Value of 68Ga PSMA-11 PET/CT Imaging of Brain Tumors-Preliminary Analysis. Clin. Nucl. Med. 2017, 42, e41–e48. [Google Scholar] [CrossRef] [PubMed]
- Uijen, M.J.M.; Derks, Y.H.W.; Merkx, R.I.J.; Schilham, M.G.M.; Roosen, J.; Privé, B.M.; van Lith, S.A.M.; van Herpen, C.M.L.; Gotthardt, M.; Heskamp, S.; et al. PSMA radioligand therapy for solid tumors other than prostate cancer: Background, opportunities, challenges, and first clinical reports. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4350–4368. [Google Scholar] [CrossRef] [PubMed]
- Salas Fragomeni, R.A.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A.; Rowe, S.P. Uptake of Prostate-Specific Membrane Antigen-Targeted 18F-DCFPyL in Cerebral Radionecrosis: Implications for Diagnostic Imaging of High-Grade Gliomas. Clin. Nucl. Med. 2018, 43, e419–e421. [Google Scholar] [CrossRef] [PubMed]
- Sácha, P.; Zámecník, J.; Barinka, C.; Hlouchová, K.; Vícha, A.; Mlcochová, P.; Hilgert, I.; Eckschlager, T.; Konvalinka, J. Expression of glutamate carboxypeptidase II in human brain. Neuroscience 2007, 144, 1361–1372. [Google Scholar] [CrossRef]
- Holzgreve, A.; Biczok, A.; Ruf, V.C.; Liesche-Starnecker, F.; Steiger, K.; Kirchner, M.A.; Unterrainer, M.; Mittlmeier, L.; Herms, J.; Schlegel, J.; et al. PSMA Expression in Glioblastoma as a Basis for Theranostic Approaches: A Retrospective, Correlational Panel Study Including Immunohistochemistry, Clinical Parameters and PET Imaging. Front. Oncol. 2021, 11, 646387. [Google Scholar] [CrossRef] [PubMed]
- Kunikowska, J.; Charzyńska, I.; Kuliński, R.; Pawlak, D.; Maurin, M.; Królicki, L. Tumor uptake in glioblastoma multiforme after IV injection of [177Lu]Lu-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1605–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Ballal, S.; Yadav, M.P.; ArunRaj, S.T.; Haresh, K.P.; Gupta, S.; Damle, N.A.; Garg, A.; Tripathi, M.; Bal, C. 177Lu-/68Ga-PSMA Theranostics in Recurrent Glioblastoma Multiforme: Proof of Concept. Clin. Nucl. Med. 2020, 45, e512–e513. [Google Scholar] [CrossRef]
- Kirchner, M.A.; Holzgreve, A.; Brendel, M.; Orth, M.; Ruf, V.C.; Steiger, K.; Pötter, D.; Gold, L.; Unterrainer, M.; Mittlmeier, L.M.; et al. PSMA PET Imaging in Glioblastoma: A Preclinical Evaluation and Theranostic Outlook. Front. Oncol. 2021, 11, 774017. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Hetzheim, H.; Kratochwil, C.; Benesova, M.; Eder, M.; Neels, O.C.; Eisenhut, M.; Kübler, W.; Holland-Letz, T.; Giesel, F.L.; et al. The Theranostic PSMA Ligand PSMA-617 in the Diagnosis of Prostate Cancer by PET/CT: Biodistribution in Humans, Radiation Dosimetry, and First Evaluation of Tumor Lesions. J. Nucl. Med. 2015, 56, 1697–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors [Ref.] | Year | Country | Study Design/Number of Centers Involved | Funding Sources |
|---|---|---|---|---|
| Akgun et al. [23] | 2020 | Turkey | Prospective/bicentric | None declared |
| Kumar et al. [21] | 2022 | India | Prospective/monocentric | None declared |
| Kunikowska et al. [20] | 2022 | Poland | Not reported/monocentric | None declared |
| Kunikowska et al. [24] | 2020 | Poland | Not reported/monocentric | None declared |
| Liu et al. [22] | 2021 | China | Retrospective/monocentric | Natural Science Foundation of China |
| Sasikumar et al. [26] | 2018 | India | Prospective/bicentric | None declared |
| Sasikumar et al. [27] | 2017 | India | Not reported/monocentric | None declared |
| Verma et al. [25] | 2019 | India | Not reported/monocentric | None declared |
| Authors [Ref.] | Sample Size (Gliomas) | Mean/Median Age (Years) | Male % | Type of Glioma (Grade II/III/IV) | Clinical Setting | Prior Imaging |
|---|---|---|---|---|---|---|
| Akgun et al. [23] | 35 | mean: 59.5 | 49% | 14/6/15 | HGG vs. LGG | MRI |
| Kumar et al. [21] | 33 | median: 37 | 67% | 0/12/21 | suspicious recurrence of HGG | MRI |
| Kunikowska et al. [20] | 34 | mean: 44.5 | 65% | 0/6/28 | suspicious recurrence of HGG | MRI |
| Kunikowska et al. [24] | 15 | mean: 44 | 67% | 0/0/15 | suspicious recurrence of HGG | MRI |
| Liu et al. [22] | 30 | mean: 50 | 43% | 14/4/12 | HGG vs. LGG | MRI and [18F]FDG PET/CT |
| Sasikumar et al. [26] | 15 | median: 50 | 80% | 1/3/11 | initial diagnosis or suspicious recurrence of HGG | MRI |
| Sasikumar et al. [27] | 6 | mean: 40 | 60% | 0/0/6 | initial diagnosis or suspicious recurrence of HGG | MRI and [18F]FDG PET/CT |
| Verma et al. [25] | 10 | mean: 52 | 80% | 3/0/7 | HGG vs. LGG | MRI and [18F]FDG PET/CT |
| Authors [Ref.] | Tracer | Hybrid Imaging | Tomograph | Injected Activity | Time from Injection to Acquisition (Minutes) | Image Analysis |
|---|---|---|---|---|---|---|
| Akgun et al. [23] | [68Ga]Ga-PSMA-11 | PET/MRI | SIGNA (GE) | 150.6 ± 31.8 MBq | 57.5 ± 3.53 | visual and semi-quantitative (SUVmax, SUVpeak, SUVmean) |
| Kumar et al. [21] | [68Ga]Ga-PSMA-11 | PET/CT + fusion with MRI | Biograph mCT (Siemens) | 148–185 MBq | 60 | visual and semi-quantitative (SUVmax, SUVmean, TBR, TV) |
| Kunikowska et al. [20] | [68Ga]Ga-PSMA-11 | PET/CT + fusion with MRI | Biograph 64 TruePoint (Siemens) | 2 MBq/kg | 60 | visual and semi-quantitative (SUVmax, SUVmean, TBR, TLR, TV) |
| Kunikowska et al. [24] | [68Ga]Ga-PSMA-11 | PET/CT + fusion with MRI | Biograph 64 TruePoint (Siemens) | 2 MBq/kg | 60 | visual and semi-quantitative (SUVmax, SUVmean, TBR, TLR, TV) |
| Liu et al. [22] | [68Ga]Ga-PSMA-617 | PET/CT + correlation with MRI | Biograph 40 (Siemens) | 1.8–2.2 MBq/kg | 60 | visual and semi-quantitative (SUVmax, SUVmean, TBR) |
| Sasikumar et al. [26] | [68Ga]Ga-PSMA-11 | PET/CT | Biograph 6 TruePoint (Siemens) or Gemini GLX (Philips) | NR | 45–60 | visual and semi-quantitative (SUVmax, TBR) |
| Sasikumar et al. [27] | [68Ga]Ga-PSMA-11 | PET/CT | Biograph 6 TruePoint (Siemens) | 100 ± 19 MBq | 60 | visual and semi-quantitative (SUVmax, TBR) |
| Verma et al. [25] | [68Ga]Ga-PSMA-11 | PET/CT | Gemini TOF (Philips) | NR | NR | visual and semi-quantitative (SUVmax and TBR) |
| Authors [Ref.] | Reference Standard | TP | FP | TN | FN | Sen | Spe | PPV | NPV | Acc |
|---|---|---|---|---|---|---|---|---|---|---|
| Akgun et al. [23] | Histology | 18 | 2 | 12 | 3 | 85.7% | 85.7% | 90% | 80% | 85.7% |
| Kumar et al. [21] | Histology or clinical/imaging FU | 30 | 0 | 3 | 0 | 100% | 100% | 100% | 100% | 100% |
| Kunikowska et al. [20] | Histology or clinical/imaging FU | 34 | 0 | 0 | 0 | 100% | NC | 100% | NC | 100% |
| Kunikowska et al. [24] * | Histology or clinical/imaging FU | 15 | 0 | 0 | 0 | 100% | NC | 100% | NC | 100% |
| Liu et al. [22] | Histology | 14 | 0 | 14 | 2 | 87.5% | 100% | 100% | 87.5% | 93.3% |
| Sasikumar et al. [26] | Histology or clinical/imaging FU | 12 | 1 | 2 | 0 | 100% | 66.7% | 92.3% | 100% | 93.3% |
| Sasikumar et al. [27] * | Histology or clinical/imaging FU | 5 | 0 | 1 | 0 | 100% | 100% | 100% | 100% | 100% |
| Verma et al. [25] | Histology | 7 | 0 | 3 | 0 | 100% | 100% | 100% | 100% | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muoio, B.; Albano, D.; Dondi, F.; Bertagna, F.; Garibotto, V.; Kunikowska, J.; Piccardo, A.; Annunziata, S.; Espeli, V.; Migliorini, D.; et al. Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis. Diagnostics 2022, 12, 1665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071665
Muoio B, Albano D, Dondi F, Bertagna F, Garibotto V, Kunikowska J, Piccardo A, Annunziata S, Espeli V, Migliorini D, et al. Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis. Diagnostics. 2022; 12(7):1665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071665
Chicago/Turabian StyleMuoio, Barbara, Domenico Albano, Francesco Dondi, Francesco Bertagna, Valentina Garibotto, Jolanta Kunikowska, Arnoldo Piccardo, Salvatore Annunziata, Vittoria Espeli, Denis Migliorini, and et al. 2022. "Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis" Diagnostics 12, no. 7: 1665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071665