
Tuberculosis in Poland: Epidemiological and Molecular Analysis during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
Method for Spacer Oligonucleotide Typing (Spoligotyping)
3. Results
3.1. Sex and Age of Tuberculosis Patients in 2020
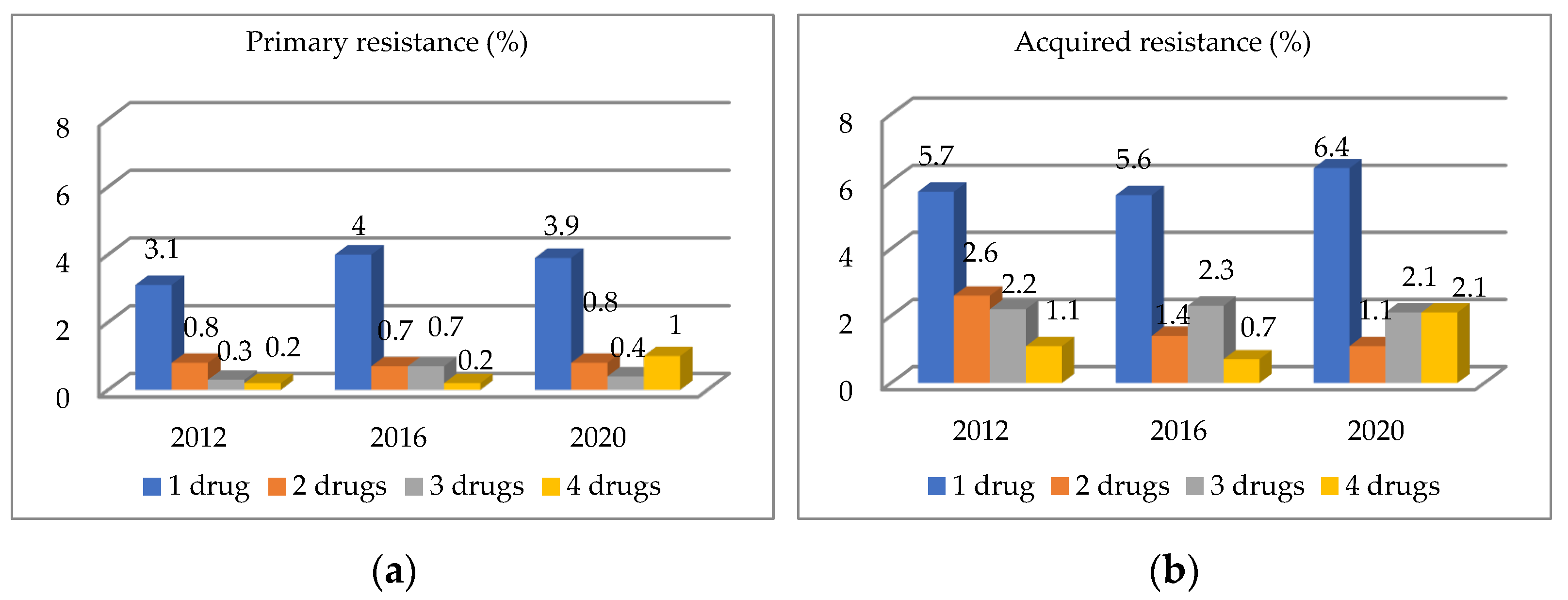
3.2. Analysis of Primary and Acquired Drug Resistance in Authors’ 2020 Study
3.3. Molecular Analysis of Mycobacterium Tuberculosis Strains Resistant to at Least 1 Drug (Compared to 20% of Sensitive Strains), Poland 2020
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021.
- Korzeniewska-Koseła, M. (Ed.) Tuberculosis and Respiratory Tract Diseases in Poland in 2020; Institute of Tuberculosis and Lung Diseases: Warsaw, Poland, 2021. [Google Scholar]
- Zielonka, T.M. Epidemiologia gruźlicy w Polsce—Implikacje w praktyce lekarza rodzinnego. Forum Med. Rodz. 2016, 1, 25–33. [Google Scholar]
- Korzeniewska-Koseła, M. (Ed.) Tuberculosis and Respiratory Tract Diseases in Poland in 2019; Institute of Tuberculosis and Lung Diseases: Warsaw, Poland, 2020. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2017; World Health Organization: Geneva, Switzerland, 2017.
- Augustynowicz-Kopeć, E. The new face of tuberculosis. Acta Med. Pol. 2018, 8, 23–36. [Google Scholar] [CrossRef]
- Kozińska, M.; Brzostek, A.; Krawiecka, D.; Rybczyńska, M.; Zwolska, Z.; Augustynowicz-Kopeć, E. MDR, pre-XDR and XDR drug-resistant tuberculosis in Poland in 2000–2009. Pneumonol. Alergol. Pol. 2011, 79, 278–287. [Google Scholar] [CrossRef]
- Korzeniewska-Koseła, M. (Ed.) Tuberculosis and Respiratory Tract Diseases in Poland in 2012; Institute of Tuberculosis and Lung Diseases: Warsaw, Poland, 2013. [Google Scholar]
- Korzeniewska-Koseła, M. (Ed.) Tuberculosis and Respiratory Tract Diseases in Poland in 2016; Institute of Tuberculosis and Lung Diseases: Warsaw, Poland, 2017. [Google Scholar]
- Kamerbeek, J.; Schouls, L.; Kolk, A.; van Agterveld, M.; van Soolingen, D.; Kuijper, S.; Bunschoten, A.; Molhuizen, A.; Shaw, R.; Goyal, M.; et al. Simultaneous detection and strain differentiation of Mycobacterium tuberculosis for diagnosis and epidemiology. J. Clin. Microbiol. 1997, 35, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Brzostek, A.; Dziadek, J. Molecular genotyping methods in epidemiological investigations of TB infections. Pneumonol. Alergol. Pol. 2012, 80, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Ramazanzadeh, R.; Shakib, P.; Rouhi, S.; Mohammadi, B.; Mohajeri, P.; Borji, S. Molecular epidemiology of Mycobacterium tuberculosis isolates in Iran using spoligotyping. New Microbes New Infect. 2020, 38, 100767. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020.
- Ong, C.W.M.; Migliori, G.B.; Raviglione, M.; MacGregor-Skinner, G.; Sotgiu, G.; Alffenaar, J.W.; Tiberi, S.; Adlhoch, C.; Alonzi, T.; Archuleta, S.; et al. Epidemic and pandemic Vidal infections: Impact on tuberculosis and the lung: A consensus by the World Association for Infectious Diseases and Immunological Disorders (WAidid), Global Tuberculosis Network (GTN), and members of the European Society of Clinical Microbiology and Infectious Diseases Study Group for Mycobacterial Infections (ESGMYC). Eur. Respir. J. 2020, 56, 2001727. [Google Scholar] [CrossRef]
- Gupta, U.; Prakash, A.; Sachdeva, S.; Pangtey, G.S.; Khosla, A.; Aggarwal, R.; Sud, R.; Margekar, S.L. COVID-19 and Tuberculosis: A Meeting of Two Pandemics. J. Assoc Physicians India 2020, 68, 69–72. [Google Scholar]
- Nikolayevskyy, V.; Holicka, Y.; van Soolingen, D.; van der Werf, M.J.; Ködmön, C.; Surkova, E.; Hillemann, D.; Groenheit, R. ERLTB-Net-2 study participants; Cirillo D. Impact of the COVID-19 pandemic on tuberculosis laboratory services in Europe. Eur. Respir. J. 2021, 57, 2003890. [Google Scholar] [CrossRef]
- Migliori, G.B.; Thong, P.M.; Akkerman, O.; Alffenaar, J.W.; Álvarez-Navascués, F.; Assao-Neino, M.M.; Bernard, P.V.; Biala, J.S.; Blanc, F.-X.; Bogorodskaya, E.M.; et al. Worldwide Effects of Coronavirus Disease Pandemic on Tuberculosis Services, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2709–2712. [Google Scholar] [CrossRef] [PubMed]
- Visca, D.; Ong, C.W.M.; Tiberi, S.; Centis, R.; Ambrosio, L.D.; Chen, B.; Mueller, J.; Mueller, P.; Duarte, R.; Dalcolmo, M.; et al. Tuberculosis and COVID-19 interaction: A review of biological, clinical and public health effects. Pulmonology 2021, 27, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Augustynowicz-Kopeć, E.; Zwolska, Z. Epidemiology of tuberculosis in children and some problems of microbiological confirmation. Post. Nauk Med. 2008, 9, 569–577. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019.
- Wingfield, T.; Tovar, M.A.; Datta, S.; Saunders, M.J.; Evans, C.A. Addressing social determinants to end tuberculosis. Lancet 2018, 391, 1129–1132. [Google Scholar] [CrossRef]
- Saunders, M.J.; Evans, C.A. Fighting poverty to prevent tuberculosis. Lancet Infect. Dis. 2016, 16, 395–396. [Google Scholar] [CrossRef]
- Wingfield, T.; Boccia, D.; Tovar, M.A.; Gavino, A.; Zevallos, K.; Montoya, R.; Lönnroth, K.; Evans, C.A. Defining catastrophic costs and comparing their importance for adverse tuberculosis outcome with multi-drug resistance: A prospective cohort study, Peru. PLoS Med. 2014, 11, e1001675. [Google Scholar] [CrossRef] [Green Version]
- Saunders, M.J.; Evans, C.A. COVID-19, tuberculosis and poverty: Preventing a perfect storm. Eur. Respir. J. 2020, 56, 2001348. [Google Scholar] [CrossRef]
- Moosazadeh, M.; Nasehi, M.; Bahrampour, A.; Khanjani, N.; Sharafi, S.; Ahmadi, S. Forecasting Tuberculosis Incidence in Iran Using Box-Jenkins Models. Iran. Red. Crescent Med. J. 2014, 16, e11779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merker, M.; Blin, C.; Mona, S.; Duforet-Frebourg, N.; Lecher, S.; Willery, E.; Blum, M.G.; Rüsch-Gerdes, S.; Mokrousov, I.; Aleksic, E.; et al. Evolutionary history and global spread of the Mycobacterium tuberculosis Beijing lineale. Nat. Genet. 2015, 47, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Polea, I.; Trofimovaa, J.; Norvaisaa, I.; Supplyc, P.; Skendersa, G.; Nodievad, A.; Ozerea, I.; Riekstinaa, V.; Igumnovab, V.; Storozenkod, J.; et al. Analysis of Mycobacterium tuberculosis genetic lineages circulating in Riga and Riga region, Latvia, isolated between 2008 and 2012. Infect. Genet Evol. 2020, 78, 104126. [Google Scholar] [CrossRef] [PubMed]
- Toungoussova, O.S.; Sandven, P.; Mariandyshev, A.O.; Nizovtseva, N.I.; Bjune, G.; Caugant, D.A. Spread of drug-resistant Mycobacterium tuberculosis strains of the Beijing genotype in the Archangel Oblast, Russia. J. Clin. Microbiol. 2020, 40, 1930–1937. [Google Scholar] [CrossRef] [Green Version]
- Kruuner, A.; Hoffner, S.E.; Sillastu, H.; Danilovits, M.; Levina, K.; Svenson, S.B.; Ghebremichael, S.; Koivula, T.; Kallenius, G. Spread of drug-resistant pulmonary tuberculosis in Estonia. J. Clin. Microbiol. 2001, 39, 3339–3345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vyazovaya, A.; Mokrousov, I.; Zhuravlev, V.; Solovieva, N.; Otten, T.; Vishnevsky, B.; Narvskaya, O. Dominance of the Beijing genotype among XDR Mycobacterium tuberculosis strains in Russia. Int. J. Mycobacteriol. 2015, 4, 84–85. [Google Scholar] [CrossRef] [Green Version]
- Roycroft, E.; O’Toole, R.F.; Fitzgibbon, M.M.; Montgomery, L.; O’Meara, M.; Downes, P.; Jackson, S.; O’Donnell, J.; Laurenson, I.F.; McLaughlin, A.M.; et al. Molecular epidemiology of multi- and extensively-drug-resistant Mycobacterium tuberculosis in Ireland, 2001–2014. J. Inf. Secur. 2018, 76, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Andrés, M.; Göhring-Zwacka, E.; Fiebig, L.; Priwitzer, M.; Richter, E.; Rüsch-Gerdes, S.; Haas, W.; Niemann, S.; Brodhun, B. Integration of molecular typing results into tuberculosis surveillance in Germany-A pilot study. PLoS ONE 2017, 12, e0188356. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex | Total | Number of Cases in Age Groups (Years) | ||||||
|---|---|---|---|---|---|---|---|---|
| 0–14 | 15–24 | 25–34 | 35–44 | 45–54 | 55–64 | 65+ | ||
| Male | 1087 (8 no data) | 2 | 38 | 108 | 205 | 259 | 283 | 184 |
| 0.18% | 3.49% | 9.93% | 18.85% | 23.82% | 26.03% | 16.92% | ||
| Female | 296 (1 no data) | 3 | 25 | 36 | 58 | 54 | 47 | 72 |
| 1.01% | 8.44% | 12.16% | 19.59% | 18.24% | 15.88% | 24.32% | ||
| Total | 1383 (9 no data) | 5 | 63 | 144 | 263 | 313 | 330 | 256 |
| 0.36% | 4.55% | 10.41% | 19.02% | 22.63% | 23.86% | 18.51% | ||
| Year | Total | Female | Male | |
|---|---|---|---|---|
| Own studies | 2012 | 4136 | 1185 (28.7%) | 2951 (71.3%) |
| 2016 | 3591 | 990 (27.6%) | 2601 (72.4%) | |
| 2020 | 1383 | 296 (21.4%) | 1087 (78.6%) | |
| Registered in the NTR | 2012 | 5070 | 1509 (29.8%) | 3561 (70.2%) |
| 2016 | 4619 | 1311 (28.4%) | 3308 (71.6%) | |
| 2020 | 2655 | 630 (23.7%) | 2025 (76.3%) |
| Year | Total | New TB Cases | Relapse TB Cases | |
|---|---|---|---|---|
| Own studies (n = 8938) | 2012 | 4136 | 3596 (87%) | 540 (13%) |
| 2016 | 3441 | 3012 (87.5%) | 429 (12.5%) | |
| 2020 | 1361 | 1174 (86.3%) | 187 (13.7%) | |
| Registered in the NTR (n = 12,344) | 2012 | 5070 | 4475 (88.3%) | 595 (11.7%) |
| 2016 | 4619 | 4106 (89%) | 513 (11%) | |
| 2020 | 2655 | 2268 (85.4%) | 387 (14.6%) |
| Primary Drug Resistance | Acquired Drug Resistance | |
|---|---|---|
| % (n) | % (n) | |
| Total | 100 (1174) | 100 (187) |
| Sensitive | 93.87 (1102) | 87.7 (164) |
| Resistant | 6.13 (72) | 12.3 (23) |
| 1 drug | 3.92 (46) | 6.42 (12) |
| S | 1.62 (19) | 2.14 (4) |
| I | 2.13 (25) | 2.14 (4) |
| R | 0.17 (2) | 2.14 (4) |
| E | 0 (0) | 0 (0) |
| I + R + other | 1.62 (19) | 5.35 (10) |
| IR | 0.17 (2) | 1.07 (2) |
| IRS | 042 (5) | 1.6 (3) |
| IRE | 0 (0) | 0.53 (1) |
| IRES | 1.02 (12) | 2.14 (4) |
| I + other | 0.6 (7) | 0.53 (1) |
| IS | 0.6 (7) | 0 (0) |
| IES | 0 (0) | 0.53 (1) |
| LSP/SNP-Based | Spoligotype Family | Lineage | SIT | Isolates in Study |
|---|---|---|---|---|
| East Asian | Beijing | 1 | 14 | |
| 265 | 8 | |||
| Euro-American | T | T1 | 53 | 8 |
| T4 | 139 | 6 | ||
| T5 | 44 | 2 | ||
| T1 | 558 | 2 | ||
| unique | 4 | |||
| Haarlem | H1 | 47 | 3 | |
| H3 | 50 | 2 | ||
| H3 | 36 | 2 | ||
| H4 | 262 | 2 | ||
| unique | 9 | |||
| LAM | LAM9 | 42 | 2 | |
| unique | 3 | |||
| URAL | unique | 6 | ||
| Indo-Oceanic | EAI | unique | 2 | |
| Unregistered | 7 | |||
| LSP/SNP-Based | Spoligotype Family | Lineage | SIT | Isolates in Study |
|---|---|---|---|---|
| East Asian | Beijing | 1 | 14 | |
| unique | 1 | |||
| Euro-American | T | T1 | 53 | 35 |
| T5 | 44 | 6 | ||
| T4 | 40 | 3 | ||
| T4 | 139 | 3 | ||
| T5 | 254 | 3 | ||
| T1 | 2 | 3 | ||
| T3 | 37 | 3 | ||
| T1 | 462 | 2 | ||
| T5 | 68 | 2 | ||
| T1 | 191 | 2 | ||
| unique | 15 | |||
| Haarlem | H3 | 50 | 21 | |
| H1 | 47 | 17 | ||
| H3 | 36 | 5 | ||
| H1 | 382 | 3 | ||
| H4 | 262 | 3 | ||
| H4 | 35 | 3 | ||
| H1 | 51 | 2 | ||
| unique | 10 | |||
| LAM | LAM9 | 42 | 5 | |
| unique | 4 | |||
| URAL | 46 | 3 | ||
| 237 | 3 | |||
| 124 | 2 | |||
| 602 | 2 | |||
| unique | 7 | |||
| S | 34 | 2 | ||
| X | unique | 3 | ||
| East-African-Indian | CAS | CAS1 | 26 | 5 |
| unique | 5 | |||
| Indo-Oceanic | EAI | unique | 3 | |
| Unregistered | 52 | |||
| Year | TB Primary/Acquired | Number of Patients Studied | Number of Patients with Resistant Mycobacteria (%) | Number of Patients with MDR (%) |
|---|---|---|---|---|
| 2012 | P | 3596 | 157 (4.4%) | 20 (0.6%) |
| W | 540 | 63 (11.7%) | 24 (4.4%) | |
| 2016 | P | 3012 | 168 (5.6%) | 32 (1.1%) |
| W | 429 | 43 (10%) | 18 (4.2%) | |
| 2020 | P | 1174 | 72 (6.1%) | 19 (1.6%) |
| W | 187 | 23 (12.3%) | 10 (5.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkowska-Tatar, D.; Zabost, A.; Kozińska, M.; Augustynowicz-Kopeć, E. Tuberculosis in Poland: Epidemiological and Molecular Analysis during the COVID-19 Pandemic. Diagnostics 2022, 12, 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081883
Borkowska-Tatar D, Zabost A, Kozińska M, Augustynowicz-Kopeć E. Tuberculosis in Poland: Epidemiological and Molecular Analysis during the COVID-19 Pandemic. Diagnostics. 2022; 12(8):1883. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081883
Chicago/Turabian StyleBorkowska-Tatar, Dagmara, Anna Zabost, Monika Kozińska, and Ewa Augustynowicz-Kopeć. 2022. "Tuberculosis in Poland: Epidemiological and Molecular Analysis during the COVID-19 Pandemic" Diagnostics 12, no. 8: 1883. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081883