
Microbiological and Clinical Findings of SARS-CoV-2 Infection after 2 Years of Pandemic: From Lung to Gut Microbiota
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
3. New Advances in Microbiological Diagnosis of SARS-CoV-2 Infection
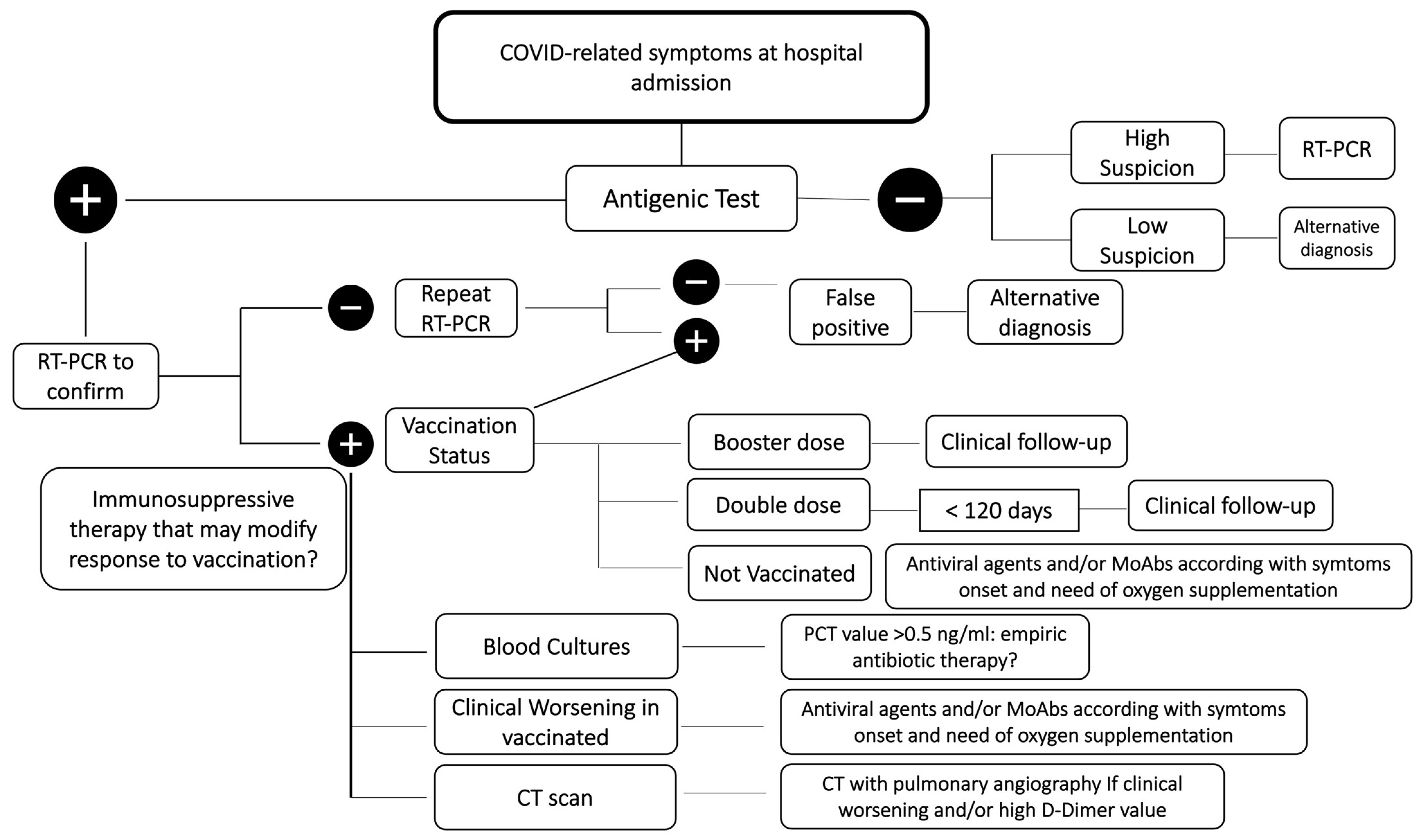
4. Clinical Diagnosis of COVID-19
5. Extrapulmonary Manifestations and the Role of Gut Microbiota in COVID-19
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Bassetti, M.; Vena, A.; Giacobbe, D.R. The novel Chinese coronavirus (2019-nCoV) infections: Challenges for fighting the storm. Eur. J. Clin. Investig. 2020, 50, e13209. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Vena, A.; Giacobbe, D.R.; Di Biagio, A.; Mikulska, M.; Taramasso, L.; De Maria, A.; Ball, L.; Brunetti, I.; Loconte, M.; Patroniti, N.A.; et al. Clinical characteristics, management and in-hospital mortality of patients with coronavirus disease 2019 in Genoa, Italy. Clin. Microbiol. Infect. 2020, 26, 1537–1544. [Google Scholar] [CrossRef]
- Russo, A.; Bellelli, V.; Ceccarelli, G.; Marincola Cattaneo, F.; Bianchi, L.; Pierro, R.; Russo, R.; Steffanina, A.; Pugliese, F.; Mastroianni, C.M.; et al. Comparison Between Hospitalized Patients Affected or Not Affected by Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 72, e1158–e1159. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef]
- Guaman-Bautista, L.P.; Moreta-Urbano, E.; Ona-Arias, C.G.; Torres-Arias, M.; Kyriakidis, N.C.; Malci, K.; Jonguitud-Borrego, N.; Rios-Solis, L.; Ramos-Martinez, E.; Lopez-Cortes, A.; et al. Tracking SARS-CoV-2: Novel Trends and Diagnostic Strategies. Diagnostics 2021, 11, 1981. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, C.Y.; Ko, W.C.; Hsueh, P.R. In vitro diagnostics of coronavirus disease 2019: Technologies and application. J. Microbiol. Immunol. Infect 2021, 54, 164–174. [Google Scholar] [CrossRef]
- Muecksch, F.; Wise, H.; Templeton, K.; Batchelor, B.; Squires, M.; McCance, K.; Jarvis, L.; Malloy, K.; Furrie, E.; Richardson, C.; et al. Longitudinal variation in SARS-CoV-2 antibody levels and emergence of viral variants: A serological analysis. Lancet Microbe 2022, 3, e493–e502. [Google Scholar] [CrossRef]
- Dal-Re, R.; Becker, S.L.; Bottieau, E.; Holm, S. Availability of oral antivirals against SARS-CoV-2 infection and the requirement for an ethical prescribing approach. Lancet Infect. Dis. 2022, 22, e231–e238. [Google Scholar] [CrossRef]
- Garcia-Salguero, C.; Culebras, E.; Merino, P.; Baos, E.; Delgado-Iribarren, A. Usefulness of SARS-CoV-2 antigen test sample as input for SARS-CoV-2 RT-PCR analysis. J. Med. Virol. 2022, 94, 1693–1695. [Google Scholar] [CrossRef]
- Scarcella, S.; Rizzelli, A.; Fontana, A.; Zecca, C.; Pasanisi, G.; Musio, K.; Putignano, A.L.; Aprile, V.; Fedele, A.; Errico, P.; et al. A CLEIA Antigen Assay in Diagnosis and Follow-Up of SARS-CoV-2-Positive Subjects. Microbiol. Spectr. 2022, 10, e0103221. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int (accessed on 21 April 2022).
- Quirino, A.; Marascio, N.; Barreca, G.S.; Gallo, L.; Giancotti, A.; Lamberti, A.G.; Peronace, C.; Trecarichi, E.M.; Fusco, P.; Mazzitelli, M.; et al. SARS-CoV-2: Some Aspects of Molecular Evolution, Cellular Pathogenesis, and Immune System Mechanism Elusion. Appl. Sci. 2021, 11, 11605. [Google Scholar] [CrossRef]
- Bruel, T.; Hadjadj, J.; Maes, P.; Planas, D.; Seve, A.; Staropoli, I.; Guivel-Benhassine, F.; Porrot, F.; Bolland, W.H.; Nguyen, Y.; et al. Serum neutralization of SARS-CoV-2 Omicron sublineages BA.1 and BA.2 in patients receiving monoclonal antibodies. Nat. Med. 2022, 28, 1297–1302. [Google Scholar] [CrossRef]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef]
- Alteri, C.; Cento, V.; Piralla, A.; Costabile, V.; Tallarita, M.; Colagrossi, L.; Renica, S.; Giardina, F.; Novazzi, F.; Gaiarsa, S.; et al. Genomic epidemiology of SARS-CoV-2 reveals multiple lineages and early spread of SARS-CoV-2 infections in Lombardy, Italy. Nat. Commun. 2021, 12, 434. [Google Scholar] [CrossRef]
- Anaclerio, F.; Ferrante, R.; Mandatori, D.; Antonucci, I.; Capanna, M.; Damiani, V.; Tomo, P.D.; Ferrante, R.; Ranaudo, M.; De Laurenzi, V.; et al. Different Strategies for the Identification of SARS-CoV-2 Variants in the Laboratory Practice. Genes 2021, 12, 1428. [Google Scholar] [CrossRef]
- Jian, M.J.; Chung, H.Y.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Lin, D.Y.; Chang, F.Y.; Hung, K.S.; Perng, C.L.; et al. SARS-CoV-2 variants with T135I nucleocapsid mutations may affect antigen test performance. Int. J. Infect. Dis. 2022, 114, 112–114. [Google Scholar] [CrossRef]
- Tzou, P.L.; Tao, K.; Pond, S.L.K.; Shafer, R.W. Coronavirus Resistance Database (CoV-RDB): SARS-CoV-2 susceptibility to monoclonal antibodies, convalescent plasma, and plasma from vaccinated persons. PLoS ONE 2022, 17, e0261045. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Gentilini Cacciola, E.; Borrazzo, C.; Filippi, V.; Bucci, T.; Vullo, F.; Celani, L.; Binetti, E.; Battistini, L.; Ceccarelli, G.; et al. Clinical Characteristics and Outcome of Patients with Suspected COVID-19 in Emergency Department (RESILIENCY Study II). Diagnostics 2021, 11, 1368. [Google Scholar] [CrossRef]
- Falcone, C.; Caracciolo, M.; Correale, P.; Macheda, S.; Vadala, E.G.; La Scala, S.; Tescione, M.; Danieli, R.; Ferrarelli, A.; Tarsitano, M.G.; et al. Can Adenosine Fight COVID-19 Acute Respiratory Distress Syndrome? J. Clin. Med. 2020, 9, 3045. [Google Scholar] [CrossRef] [PubMed]
- Gozzo, L.; Viale, P.; Longo, L.; Vitale, D.C.; Drago, F. The Potential Role of Heparin in Patients With COVID-19: Beyond the Anticoagulant Effect. A Review. Front. Pharmacol. 2020, 11, 1307. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. Hlh Across Speciality Collaboration, U.K. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Munblit, D.; Nekliudov, N.A.; Bugaeva, P.; Blyuss, O.; Kislova, M.; Listovskaya, E.; Gamirova, A.; Shikhaleva, A.; Belyaev, V.; Timashev, P.; et al. Stop COVID Cohort: An Observational Study of 3480 Patients Admitted to the Sechenov University Hospital Network in Moscow City for Suspected Coronavirus Disease 2019 (COVID-19) Infection. Clin. Infect. Dis. 2021, 73, 1–11. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; Moustafa Abo El-Ella, D.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann. Med. 2022, 54, 524–540. [Google Scholar] [CrossRef]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Femy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected With Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef]
- Piersiala, K.; Kakabas, L.; Bruckova, A.; Starkhammar, M.; Cardell, L.O. Acute odynophagia: A new symptom of COVID-19 during the SARS-CoV-2 Omicron variant wave in Sweden. J. Intern. Med. 2022, 292, 154–161. [Google Scholar] [CrossRef]
- Hertanto, D.M.; Sutanto, H.; Lusida, M.I.; Kuntaman, K.; Santoso, D. The genomic and clinical features of the COVID-19 Omicron variant: A narrative review [version 1; peer review: 1 not approved]. F1000Research 2022, 11, 353. [Google Scholar] [CrossRef]
- Hui, K.P.Y.; Ho, J.C.W.; Cheung, M.C.; Ng, K.C.; Ching, R.H.H.; Lai, K.L.; Kam, T.T.; Gu, H.; Sit, K.Y.; Hsin, M.K.Y.; et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Kho, N.; Noble, P.W.; Isonaka, S.; et al. Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance—One Hospital, California, 15 July–23 September 2021, and 21 December 2021–27 January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 217–223. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef]
- Caralis, P. Case Reports of COVID 19 Recurrence. J. Prim. Care Community Health 2021, 12, 2150132720982752. [Google Scholar] [CrossRef]
- Pilz, S.; Chakeri, A.; Ioannidis, J.P.; Richter, L.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Allerberger, F. SARS-CoV-2 re-infection risk in Austria. Eur. J. Clin. Investig. 2021, 51, e13520. [Google Scholar] [CrossRef]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination—Kentucky, May–June 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1081–1083. [Google Scholar] [CrossRef]
- Green, H.; Yahav, D.; Eliakim-Raz, N.; Karny-Epstein, N.; Kushnir, S.; Shochat, T.; Tadmor, B.; Grossman, A. Risk-factors for re-admission and outcome of patients hospitalized with confirmed COVID-19. Sci. Rep. 2021, 11, 17416. [Google Scholar] [CrossRef]
- Velez-Paez, J.L.; Tercero-Martinez, W.; Jimenez-Alulima, G.; Navarrete-Dominguez, J.; Cornejo-Loor, L.; Castro-Bustamante, C.; Cabanillas-Lazo, M.; Barboza, J.J.; Rodriguez-Morales, A.J. Neutrophil-to-lymphocyte ratio and mean platelet volume in the diagnosis of bacterial infections in COVID-19 patients. A preliminary analysis from Ecuador. Infez. Med. 2021, 29, 530–537. [Google Scholar] [CrossRef]
- Alsaied, T.; Tremoulet, A.H.; Burns, J.C.; Saidi, A.; Dionne, A.; Lang, S.M.; Newburger, J.W.; de Ferranti, S.; Friedman, K.G. Review of Cardiac Involvement in Multisystem Inflammatory Syndrome in Children. Circulation 2021, 143, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Rout, A. Use of Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in COVID-19. J. Clin. Med. Res. 2020, 12, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Trecarichi, E.M.; Mazzitelli, M.; Serapide, F.; Pelle, M.C.; Tassone, B.; Arrighi, E.; Perri, G.; Fusco, P.; Scaglione, V.; Davoli, C.; et al. Clinical characteristics and predictors of mortality associated with COVID-19 in elderly patients from a long-term care facility. Sci. Rep. 2020, 10, 20834. [Google Scholar] [CrossRef]
- Carubbi, F.; Salvati, L.; Alunno, A.; Maggi, F.; Borghi, E.; Mariani, R.; Mai, F.; Paoloni, M.; Ferri, C.; Desideri, G.; et al. Ferritin is associated with the severity of lung involvement but not with worse prognosis in patients with COVID-19: Data from two Italian COVID-19 units. Sci. Rep. 2021, 11, 4863. [Google Scholar] [CrossRef] [PubMed]
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 4080. [Google Scholar] [CrossRef]
- Zhang, J.J.; Cao, Y.Y.; Dong, X.; Wang, B.C.; Liao, M.Y.; Lin, J.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Distinct characteristics of COVID-19 patients with initial rRT-PCR-positive and rRT-PCR-negative results for SARS-CoV-2. Allergy 2020, 75, 1809–1812. [Google Scholar] [CrossRef]
- Domingo, P.; Pomar, V.; Mur, I.; Castellvi, I.; Corominas, H.; de Benito, N. Not all COVID-19 pandemic waves are alike. Clin. Microbiol. Infect. 2021, 27, 1040.e7–1040.e10. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Villar, J.; Anon, J.M.; Ferrando, C.; Aguilar, G.; Munoz, T.; Ferreres, J.; Ambros, A.; Aldecoa, C.; Suarez-Sipmann, F.; Thorpe, K.E.; et al. Efficacy of dexamethasone treatment for patients with the acute respiratory distress syndrome caused by COVID-19: Study protocol for a randomized controlled superiority trial. Trials 2020, 21, 717. [Google Scholar] [CrossRef]
- Petersen, M.W.; Meyhoff, T.S.; Helleberg, M.; Kjaer, M.N.; Granholm, A.; Hjortso, C.J.S.; Jensen, T.S.; Moller, M.H.; Hjortrup, P.B.; Wetterslev, M.; et al. Low-dose hydrocortisone in patients with COVID-19 and severe hypoxia (COVID STEROID) trial-Protocol and statistical analysis plan. Acta Anaesthesiol. Scand. 2020, 64, 1365–1375. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Dequin, P.F.; Heming, N.; Meziani, F.; Plantefeve, G.; Voiriot, G.; Badie, J.; Francois, B.; Aubron, C.; Ricard, J.D.; Ehrmann, S.; et al. Effect of Hydrocortisone on 21-Day Mortality or Respiratory Support Among Critically Ill Patients With COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Derde, L.; Al-Beidh, F.; Annane, D.; Arabi, Y.; Beane, A.; van Bentum-Puijk, W.; Berry, L.; Bhimani, Z.; Bonten, M.; et al. Effect of Hydrocortisone on Mortality and Organ Support in Patients With Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA 2020, 324, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Group, W.H.O.R.E.A.f.C.-T.W.; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Welte, T.; Ambrose, L.J.; Sibbring, G.C.; Sheikh, S.; Mullerova, H.; Sabir, I. Current evidence for COVID-19 therapies: A systematic literature review. Eur. Respir. Rev. 2021, 30, 200384. [Google Scholar] [CrossRef]
- Ko, J.J.; Wu, C.; Mehta, N.; Wald-Dickler, N.; Yang, W.; Qiao, R. A Comparison of Methylprednisolone and Dexamethasone in Intensive Care Patients With COVID-19. J. Intensive Care Med. 2021, 36, 673–680. [Google Scholar] [CrossRef]
- Li, Q.; Li, W.; Jin, Y.; Xu, W.; Huang, C.; Li, L.; Huang, Y.; Fu, Q.; Chen, L. Efficacy Evaluation of Early, Low-Dose, Short-Term Corticosteroids in Adults Hospitalized with Non-Severe COVID-19 Pneumonia: A Retrospective Cohort Study. Infect. Dis. Ther. 2020, 9, 823–836. [Google Scholar] [CrossRef]
- Chatterjee, K.; Wu, C.P.; Bhardwaj, A.; Siuba, M. Steroids in COVID-19: An overview. Cleve Clin. J. Med. 2020. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Barbieri, G.; Galfo, V.; Russo, A.; Virdis, A.; Forfori, F.; Corradi, F.; Guarracino, F.; Carrozzi, L.; et al. Role of Low-Molecular-Weight Heparin in Hospitalized Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia: A Prospective Observational Study. Open Forum. Infect. Dis. 2020, 7, ofaa563. [Google Scholar] [CrossRef]
- Olender, S.A.; Perez, K.K.; Go, A.S.; Balani, B.; Price-Haywood, E.G.; Shah, N.S.; Wang, S.; Walunas, T.L.; Swaminathan, S.; Slim, J.; et al. Remdesivir for Severe Coronavirus Disease 2019 (COVID-19) Versus a Cohort Receiving Standard of Care. Clin. Infect. Dis. 2021, 73, e4166–e4174. [Google Scholar] [CrossRef]
- Consortium, W.H.O.S.T.; Pan, H.; Peto, R.; Henao-Restrepo, A.M.; Preziosi, M.P.; Sathiyamoorthy, V.; Abdool Karim, Q.; Alejandria, M.M.; Hernandez Garcia, C.; Kieny, M.P.; et al. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Milross, L.; Majo, J.; Cooper, N.; Kaye, P.M.; Bayraktar, O.; Filby, A.; Fisher, A.J. Post-mortem lung tissue: The fossil record of the pathophysiology and immunopathology of severe COVID-19. Lancet Respir. Med. 2022, 10, 95–106. [Google Scholar] [CrossRef]
- Nagele, M.P.; Haubner, B.; Tanner, F.C.; Ruschitzka, F.; Flammer, A.J. Endothelial dysfunction in COVID-19: Current findings and therapeutic implications. Atherosclerosis 2020, 314, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Weckbach, L.T.; Schweizer, L.; Kraechan, A.; Bieber, S.; Ishikawa-Ankerhold, H.; Hausleiter, J.; Massberg, S.; Straub, T.; Klingel, K.; Grabmaier, U.; et al. Association of Complement and MAPK Activation With SARS-CoV-2-Associated Myocardial Inflammation. JAMA Cardiol. 2022, 7, 286–297. [Google Scholar] [CrossRef]
- Ferrara, F.; Vitiello, A. Scientific and pharmacological rationale for the treatment of cardiac damage caused by COVID-19. Discov. Med. 2020, 30, 155–161. [Google Scholar]
- Titi, L.; Magnanimi, E.; Mancone, M.; Infusino, F.; Coppola, G.; Del Nonno, F.; Colombo, D.; Nardacci, R.; Falasca, L.; d’Amati, G.; et al. Fatal Takotsubo syndrome in critical COVID-19 related pneumonia. Cardiovasc. Pathol. 2021, 51, 107314. [Google Scholar] [CrossRef]
- Guglin, M.; Ballut, K.; Ilonze, O.; Jones, M.; Rao, R. Clinical variants of myocardial involvement in COVID-19-positive patients: A cumulative experience of 2020. Heart Fail. Rev. 2022, 27, 1341–1353. [Google Scholar] [CrossRef]
- Bikdeli, B.; Garcia, D.A. In patients hospitalized with COVID-19, therapeutic- vs. prophylactic-dose heparin did not reduce a composite outcome at 28 d. Ann. Intern. Med. 2022, 175, JC16. [Google Scholar] [CrossRef]
- Lee, J.R.; Silberzweig, J.; Akchurin, O.; Choi, M.E.; Srivatana, V.; Lin, J.; Liu, F.; Malha, L.; Lubetzky, M.; Dadhania, D.M.; et al. Characteristics of Acute Kidney Injury in Hospitalized COVID-19 Patients in an Urban Academic Medical Center. Clin. J. Am. Soc. Nephrol. 2021, 16, 284–286. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ikizler, T.A.; Sharma, S.; Mohammed, A. Acute Kidney Injury and Advanced Kidney Disease in the COVID-19 Pandemic: Proceedings From a National Kidney Foundation Symposium. Kidney Med. 2021, 3, 426–432. [Google Scholar] [CrossRef]
- Karadas, O.; Ozturk, B.; Sonkaya, A.R. A prospective clinical study of detailed neurological manifestations in patients with COVID-19. Neurol. Sci. 2020, 41, 1991–1995. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Holmes, E.A.; Harrison, P.J. Depression and anxiety disorders during the COVID-19 pandemic: Knowns and unknowns. Lancet 2021, 398, 1665–1666. [Google Scholar] [CrossRef]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients With COVID-19: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Beckers, E.; Mustin, V.; Ducarme, M.; Journe, F.; Marchant, A.; Jouffe, L.; Barillari, M.R.; Cammaroto, G.; et al. Prevalence and 6-month recovery of olfactory dysfunction: A multicentre study of 1363 COVID-19 patients. J. Intern. Med. 2021, 290, 451–461. [Google Scholar] [CrossRef]
- Al-Namaeh, M. Ocular manifestations of COVID-19. Ther. Adv. Ophthalmol. 2022, 14, 25158414221083374. [Google Scholar] [CrossRef]
- Kaya, G.; Kaya, A.; Saurat, J.H. Clinical and Histopathological Features and Potential Pathological Mechanisms of Skin Lesions in COVID-19: Review of the Literature. Dermatopathology 2020, 7, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Dastoli, S.; Mignogna, C.; Bennardo, L.; Lio, E.; Pelle, M.C.; Trecarichi, E.M.; Pereira, B.I.; Nistico, S.P.; Torti, C. Histopathology and immunophenotyping of late onset cutaneous manifestations of COVID-19 in elderly patients: Three case reports. World J. Clin. Cases 2021, 9, 5744–5751. [Google Scholar] [CrossRef]
- Gottlieb, M.; Long, B. Dermatologic manifestations and complications of COVID-19. Am. J. Emerg. Med. 2020, 38, 1715–1721. [Google Scholar] [CrossRef]
- Zeng, W.; Qi, K.; Ye, M.; Zheng, L.; Liu, X.; Hu, S.; Zhang, W.; Tang, W.; Xu, J.; Yu, D.; et al. Gastrointestinal symptoms are associated with severity of coronavirus disease 2019: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 168–176. [Google Scholar] [CrossRef]
- Cheung, K.S.; Hung, I.F.N.; Chan, P.P.Y.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.H.; Tam, A.R.; et al. Gastrointestinal Manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Zhang, X.; Tang, C.; Tian, D.; Hou, X.; Yang, Y. Management of Digestive Disorders and Procedures Associated With COVID-19. Am. J. Gastroenterol. 2020, 115, 1153–1155. [Google Scholar] [CrossRef] [PubMed]
- Kaafarani, H.M.A.; El Moheb, M.; Hwabejire, J.O.; Naar, L.; Christensen, M.A.; Breen, K.; Gaitanidis, A.; Alser, O.; Mashbari, H.; Bankhead-Kendall, B.; et al. Gastrointestinal Complications in Critically Ill Patients With COVID-19. Ann. Surg. 2020, 272, e61–e62. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Tong, Z.; Ma, Z.; Luo, L.; Tang, Y.; Teng, Y.; Yu, H.; Meng, H.; Peng, C.; Zhang, Q.; et al. Gastrointestinal Bleeding, but Not Other Gastrointestinal Symptoms, Is Associated With Worse Outcomes in COVID-19 Patients. Front. Med. 2021, 8, 759152. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, L.; Xue, L.; Liu, L.; Yan, X.; Yan, X.; Huang, S.; Zhang, B.; Xu, T.; Li, C.; et al. Risk factors of liver injury in patients with coronavirus disease 2019 in Jiangsu, China: A retrospective, multi-center study. J. Med. Virol. 2021, 93, 3305–3311. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Scagnolari, C.; Pugliese, F.; Mastroianni, C.M.; d’Ettorre, G. Probiotics and COVID-19. Lancet Gastroenterol. Hepatol. 2020, 5, 721–722. [Google Scholar] [CrossRef]
- Wander, P.; Epstein, M.; Bernstein, D. COVID-19 Presenting as Acute Hepatitis. Am. J. Gastroenterol. 2020, 115, 941–942. [Google Scholar] [CrossRef] [PubMed]
- El Moheb, M.; Naar, L.; Christensen, M.A.; Kapoen, C.; Maurer, L.R.; Farhat, M.; Kaafarani, H.M.A. Gastrointestinal Complications in Critically Ill Patients With and Without COVID-19. JAMA 2020, 324, 1899–1901. [Google Scholar] [CrossRef]
- Round, J.L.; Mazmanian, S.K. The gut microbiota shapes intestinal immune responses during health and disease. Nat. Rev. Immunol. 2009, 9, 313–323. [Google Scholar] [CrossRef]
- Francino, M.P. Early development of the gut microbiota and immune health. Pathogens 2014, 3, 769–790. [Google Scholar] [CrossRef]
- Zhao, N.; Wang, S.; Li, H.; Liu, S.; Li, M.; Luo, J.; Su, W.; He, H. Influence of Novel Highly Pathogenic Avian Influenza A (H5N1) Virus Infection on Migrating Whooper Swans Fecal Microbiota. Front. Cell Infect. Microbiol. 2018, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef]
- Giron, L.B.; Dweep, H.; Yin, X.; Wang, H.; Damra, M.; Goldman, A.R.; Gorman, N.; Palmer, C.S.; Tang, H.Y.; Shaikh, M.W.; et al. Plasma Markers of Disrupted Gut Permeability in Severe COVID-19 Patients. Front. Immunol. 2021, 12, 686240. [Google Scholar] [CrossRef]
- McCarty, M.F.; Lerner, A. Perspective: Prospects for Nutraceutical Support of Intestinal Barrier Function. Adv. Nutr. 2021, 12, 316–324. [Google Scholar] [CrossRef] [PubMed]
- d’Ettorre, G.; Ceccarelli, G.; Marazzato, M.; Campagna, G.; Pinacchio, C.; Alessandri, F.; Ruberto, F.; Rossi, G.; Celani, L.; Scagnolari, C.; et al. Challenges in the Management of SARS-CoV-2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Front. Med. 2020, 7, 389. [Google Scholar] [CrossRef]
- Al Bander, Z.; Nitert, M.D.; Mousa, A.; Naderpoor, N. The Gut Microbiota and Inflammation: An Overview. Int. J. Environ. Res. Public Health 2020, 17, 7618. [Google Scholar] [CrossRef]
- Liu, Q.; Mak, J.W.Y.; Su, Q.; Yeoh, Y.K.; Lui, G.C.Y.; Ng, S.S.S.; Zhang, F.; Li, A.Y.; Lu, W.; Hui, D.S.C.; et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut 2022, 71, 544–552. [Google Scholar] [CrossRef]
- Mizutani, T.; Ishizaka, A.; Koga, M.; Ikeuchi, K.; Saito, M.; Adachi, E.; Yamayoshi, S.; Iwatsuki-Horimoto, K.; Yasuhara, A.; Kiyono, H.; et al. Correlation Analysis between Gut Microbiota Alterations and the Cytokine Response in Patients with Coronavirus Disease during Hospitalization. Microbiol. Spectr. 2022, 10, e01689-21. [Google Scholar] [CrossRef]
- Vestad, B.; Ueland, T.; Lerum, T.V.; Dahl, T.B.; Holm, K.; Barratt-Due, A.; Kåsine, T.; Dyrhol-Riise, A.M.; Stiksrud, B.; Tonby, K.; et al. Respiratory dysfunction three months after severe COVID-19 is associated with gut microbiota alterations. J. Intern. Med. 2022, 291, 801–812. [Google Scholar] [CrossRef]
- Brumfield, K.D.; Leddy, M.; Usmani, M.; Cotruvo, J.A.; Tien, C.T.; Dorsey, S.; Graubics, K.; Fanelli, B.; Zhou, I.; Registe, N.; et al. Microbiome Analysis for Wastewater Surveillance during COVID-19. mBio 2022, 13, e00591-22. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Saito, M.; Tamura, A.; Prawisuda, D.; Mizutani, T.; Yotsuyanagi, H. The human microbiome and COVID-19: A systematic review. PLoS ONE 2021, 16, e0253293. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, I.; Chung, M.; Angel, L.; Tsay, J.J.; Wu, B.G.; Yeung, S.T.; Krolikowski, K.; Li, Y.; Duerr, R.; Schluger, R.; et al. Microbial signatures in the lower airways of mechanically ventilated COVID-19 patients associated with poor clinical outcome. Nat. Microbiol. 2021, 6, 1245–1258. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Aliberti, S.; Barisione, E.; Centanni, S.; De Rosa, F.G.; Di Marco, F.; Gori, A.; Granata, G.; Mikulska, M.; et al. Balancing evidence and frontline experience in the early phases of the COVID-19 pandemic: Current position of the Italian Society of Anti-infective Therapy (SITA) and the Italian Society of Pulmonology (SIP). Clin. Microbiol. Infect. 2020, 26, 880–894. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S.; Cherian, S.; Brealey, D.; Cutler, S.; King, C.; Killick, C.; Richards, O.; Cheema, Y.; Bailey, C.; et al. Prevalence of phenotypes of acute respiratory distress syndrome in critically ill patients with COVID-19: A prospective observational study. Lancet Respir. Med. 2020, 8, 1209–1218. [Google Scholar] [CrossRef]
- Falcone, M.; Bassetti, M.; Tiseo, G.; Giordano, C.; Nencini, E.; Russo, A.; Graziano, E.; Tagliaferri, E.; Leonildi, A.; Barnini, S.; et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit. Care 2020, 24, 29. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Iacovelli, A.; Restuccia, G.; Ceccarelli, G.; Giordano, A.; Farcomeni, A.; Morelli, A.; Venditti, M. Predictors of outcome in ICU patients with septic shock caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin. Microbiol. Infect. 2016, 22, 444–450. [Google Scholar] [CrossRef]
- Bassetti, M.; Vena, A.; Giacobbe, D.R.; Falcone, M.; Tiseo, G.; Giannella, M.; Pascale, R.; Meschiari, M.; Digaetano, M.; Oliva, A.; et al. Ceftolozane/Tazobactam for Treatment of Severe ESBL-Producing Enterobacterales Infections: A Multicenter Nationwide Clinical Experience (CEFTABUSE II Study). Open Forum. Infect. Dis. 2020, 7, ofaa139. [Google Scholar] [CrossRef]
- Bassetti, M.; Castaldo, N.; Cattelan, A.; Mussini, C.; Righi, E.; Tascini, C.; Menichetti, F.; Mastroianni, C.M.; Tumbarello, M.; Grossi, P.; et al. Ceftolozane/tazobactam for the treatment of serious Pseudomonas aeruginosa infections: A multicentre nationwide clinical experience. Int. J. Antimicrob. Agents 2019, 53, 408–415. [Google Scholar] [CrossRef]
- Russo, A.; Falcone, M.; Gutierrez-Gutierrez, B.; Calbo, E.; Almirante, B.; Viale, P.L.; Oliver, A.; Ruiz-Garbajosa, P.; Gasch, O.; Gozalo, M.; et al. Predictors of outcome in patients with severe sepsis or septic shock due to extended-spectrum beta-lactamase-producing Enterobacteriaceae. Int. J. Antimicrob. Agents 2018, 52, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, A.; Bassetti, M.; Ceccarelli, G.; Carannante, N.; Losito, A.R.; Bartoletti, M.; Corcione, S.; Granata, G.; Santoro, A.; Giacobbe, D.R.; et al. Bloodstream infections caused by carbapenem-resistant Acinetobacter baumannii: Clinical features, therapy and outcome from a multicenter study. J. Infect. 2019, 79, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Giuliano, S.; Ceccarelli, G.; Alessandri, F.; Giordano, A.; Brunetti, G.; Venditti, M. Comparison of Septic Shock Due to Multidrug-Resistant Acinetobacter baumannii or Klebsiella pneumoniae Carbapenemase-Producing, K. pneumoniae in Intensive Care Unit Patients. Antimicrob. Agents Chemother. 2018, 62, e02562-17. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Marincola Cattaneo, F.; Brunetti, G.; Picciarella, A.; Russo, R.; Hallgass, M.E.; Sabetta, F. Clinical features and outcome of difficult-to-treat infections in a high-intensity medical care ward. Minerva Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Russo, A.; Righi, E.; Dolso, E.; Merelli, M.; D’Aurizio, F.; Sartor, A.; Curcio, F. Role of procalcitonin in bacteremic patients and its potential use in predicting infection etiology. Expert Rev. Anti. Infect. Ther. 2019, 17, 99–105. [Google Scholar] [CrossRef]
- Bassetti, M.; Russo, A.; Righi, E.; Dolso, E.; Merelli, M.; D’Aurizio, F.; Sartor, A.; Curcio, F. Role of procalcitonin in predicting etiology in bacteremic patients: Report from a large single-center experience. J. Infect. Public Health 2020, 13, 40–45. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; Carnelutti, A.; Graziano, E.; Russo, A. Multidrug-resistant Klebsiella pneumoniae: Challenges for treatment, prevention and infection control. Expert Rev. Anti-Infect. Ther. 2018, 16, 749–761. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; Vena, A.; Graziano, E.; Russo, A.; Peghin, M. Risk stratification and treatment of ICU-acquired pneumonia caused by multidrug- resistant/extensively drug-resistant/pandrug-resistant bacteria. Curr. Opin. Crit. Care 2018, 24, 385–393. [Google Scholar] [CrossRef]
- Bassetti, M.; Russo, A.; Carnelutti, A.; La Rosa, A.; Righi, E. Antimicrobial resistance and treatment: An unmet clinical safety need. Expert Opin. Drug Saf. 2018, 17, 669–680. [Google Scholar] [CrossRef]
- Alessandri, F.; Pugliese, F.; Angeletti, S.; Ciccozzi, M.; Russo, A.; Mastroianni, C.M.; d’Ettorre, G.; Venditti, M.; Ceccarelli, G. Procalcitonin in the Assessment of Ventilator Associated Pneumonia: A Systematic Review. Adv. Exp. Med. Biol. 2021, 1323, 103–114. [Google Scholar]
- Russo, A.; Gavaruzzi, F.; Ceccarelli, G.; Borrazzo, C.; Oliva, A.; Alessandri, F.; Magnanimi, E.; Pugliese, F.; Venditti, M. Multidrug-resistant Acinetobacter baumannii infections in COVID-19 patients hospitalized in intensive care unit. Infection 2022, 50, 83–92. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Test Name | Technology | Manufacturer | Specimen | Sensitivity% (95%; C.I.) | Specificity% (95%; C.I.) | TAT (min) | Reference |
|---|---|---|---|---|---|---|---|
| Molecular assay | |||||||
| ARGENE SARSCOV-2 RGENE (RdRp, N, E) | Two triplex PCR | bioMe’rieux (France) | Nasopharyngeal swabs | NA | NA | 3–4 h | Lai C-C et al., 2021 [8] |
| Allplex 2019-nCoV assay Target genes (E, N and RdRp) | Multiplex real-time PCR | Seegene (Korea) | Sputum, nasopharyngeal swab, nasopharyngeal aspirate, bronchoalveolar lavage, throat swab | 98.2 (95%; 90.3–100.0) | 100 (95%; 94.9–100.0) | 110 | Zhou Y et al., 2021 [3] |
| TaqPath COVID-19 high throughput combo Target genes (S, N) | Multiplex real-time PCR | Thermo Fisher Scientific (USA) | Saliva, nasal, nasopharyngeal samples | 100 (95%; 97.9–100.0) | 100 (95%; 98.6–100) | Can run up to 8000 reactions per day | Zhou Y et al., 2021 [3] |
| Xpert Xpress SARS-CoV-2 Target genes (N2, E) | RT-PCR (point of care) | Cepheid (USA) | Nasopharyngeal swabs, nasal aspirate | 99 (95%; 97.0–99.0) | 97 (95%; 95.0–98.0) | 45 | Lai C-C et al., 2021 [8] |
| ID NOW COVID-19 assay Target gene (RdpRp) | Isothermal nucleic acid amplification | Abbot (USA) | Nasopharyngeal and nasal swabs | 95.0% | 97.9% | ≤13 | Lai C-C et al., 2021 [8] |
| iAMP COVID-19 detection kit Target genes (N, ORF1ab) | Isothermal real-time fluorescent reverse transcription | Atilia BioSystems (USA) | Nasopharyngeal, oropharyngeal swabs | NA | NA | 90 | Guaman-Bautista et al., 2021 [7] |
| Agilent SARS-CoV-2 qRT-PCR Dx Kit Target genes (N1 and N2) | Real-time reverse transcription-polymerase chain reaction | Agilent | Nasopharyngeal, nasal and oropharyngeal swabs | 95.0% | NA | 90 | CDC |
| Syndromic test | |||||||
| BiofireFilmarrayRP.-2.1 Target genes (RdRp, N, E) | Multiplex real-time PCR | bioMérieux (France) | Nasopharyngeal swabs | 98.4 (NA) | 98.9 (NA) | 45 | Lai C-C et al., 2021 [8]; https://www.fda.gov |
| QIAstat-Dx Respiratory 2019-nCoV Panel (22 targets) (RdRp, E) | Multiplex real-time PCR | QIAGEN (Netherlands) | Nasopharyngeal swabs | 97.2 (NA) | 96.1 (NA) | <70 min | Lai C-C et al., 2021 [8]; https://www.qiagen.com |
| Serological assay | |||||||
| SARS-CoV-2 IgG (CMIA) IgG | Chemiluminescent microparticle immunoassay | Abbott Laboratories, IL, USA | Serum or plasma | 3–7 days after symptom onset: 25.0 8–13 days: 86.1 >14 days: 100 | 99.6–100 | NA | Lai C-C et al., 2021 [8] |
| Elecsys Anti-SARSCoV-2 (ECLIA) Total antibody (including IgG) | Electrochemiluminescence | Roche Diagnostics Basel, Switzerland | Serum or plasma | 0–6 days aftersymptom onset: 65.5 7–13 days: 88.1 >14 days: 100 | 99.8 | 18 min | Lai C-C et al., 2021 [8] |
| Anti-SARS-CoV-2 ELISA (EIA) IgA and IgG | Immunoenzymatic | EUROIMMUN AG (Germany) | Serum | NA | NA | 2–3 h/96 samples | Lai C-C et al., 2021 [8] |
| LIAISON SARS-CoV-2 S1/S2 IgG (CLIA) IgG | Chemiluminescence | DiaSorin | Serum | 97.56 | 99.3 | 35 | Zhou Y et al., 2021 [8] |
| Platelia SARS-CoV-2 total antibody assay (ELISA) Total antibody | Immunoenzymatic | Bio-Rad | Serum | 100.0 | 99.6 | NA | Zhou Y et al., 2021 [8] |
| Access SARS-CoV-2 IgG(CLIA) | Chemiluminescence | Beckman Coulter, Inc. | Serum | 96.8 | 99.6 | NA | Guaman-Bautista LP., et al., 2021 [7] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, A.; Serapide, F.; Quirino, A.; Tarsitano, M.G.; Marascio, N.; Serraino, R.; Rotundo, S.; Matera, G.; Trecarichi, E.M.; Torti, C. Microbiological and Clinical Findings of SARS-CoV-2 Infection after 2 Years of Pandemic: From Lung to Gut Microbiota. Diagnostics 2022, 12, 2143. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092143
Russo A, Serapide F, Quirino A, Tarsitano MG, Marascio N, Serraino R, Rotundo S, Matera G, Trecarichi EM, Torti C. Microbiological and Clinical Findings of SARS-CoV-2 Infection after 2 Years of Pandemic: From Lung to Gut Microbiota. Diagnostics. 2022; 12(9):2143. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092143
Chicago/Turabian StyleRusso, Alessandro, Francesca Serapide, Angela Quirino, Maria Grazia Tarsitano, Nadia Marascio, Riccardo Serraino, Salvatore Rotundo, Giovanni Matera, Enrico Maria Trecarichi, and Carlo Torti. 2022. "Microbiological and Clinical Findings of SARS-CoV-2 Infection after 2 Years of Pandemic: From Lung to Gut Microbiota" Diagnostics 12, no. 9: 2143. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092143