
Deep Learning for Automatic Detection of Periodic Limb Movement Disorder Based on Electrocardiogram Signals

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. ECG Dataset
2.3. DeepPLM Model
2.4. Implementation
2.5. Evaluation Index
3. Results
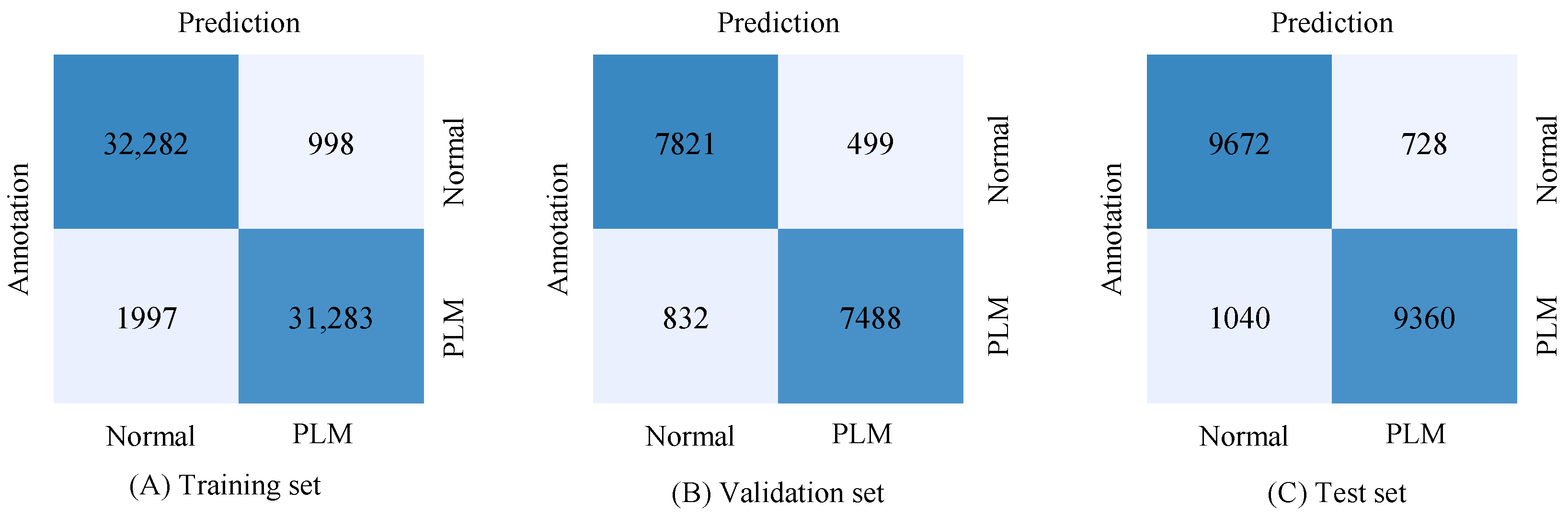
3.1. Performance of the Single-Lead ECG-Based Detection
3.2. Performance of the DeepPLM Model Optimization
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scofield, H.; Roth, T.; Drake, C. Periodic limb movements during sleep: Population prevalence, clinical correlates, and racial differences. Sleep 2008, 31, 1221–1227. [Google Scholar] [PubMed]
- Boivin, D.B.; Montplaisir, J.; Poirier, G. The effects of L-dopa on periodic leg movements and sleep organization in narcolepsy. Clin. Neuropharmacol. 1989, 12, 339–345. [Google Scholar] [CrossRef]
- Lapierre, O.; Montplaisir, J. Polysomnographic features of REM sleep behavior disorder: Development of a scoring method. Neurology 1992, 42, 1371–1374. [Google Scholar] [CrossRef] [PubMed]
- Ancoli-Israel, S.; Kripke, D.F.; Mason, W.; Kaplan, O.J. Sleep apnea and periodic movements in an aging sample. J. Gerontol. 1985, 40, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Wetter, T.C.; Collado-Seidel, V.; Pollmacher, T.; Yassouridis, A.; Trenkwalder, C. Sleep and periodic leg movement patterns in drug-free patients with Parkinson’s disease and multiple system atrophy. Sleep 2000, 23, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.B.; Sillau, S.; Dean, D.A.; Lutsey, P.L.; Redline, S. Periodic limb movements during sleep and prevalent hypertension in the multi-ethnic study of atherosclerosis. Hypertens 2015, 65, 70–77. [Google Scholar] [CrossRef]
- Douglas, N.J.; Thomas, S.; Jan, M.A. Clinical value of polysomnography. Lancet 1992, 339, 347–350. [Google Scholar] [CrossRef]
- Wetter, T.C.; Dirlich, G.; Streit, J.; Trenkwalder, C.; Schuld, A.; Pollmächer, T. An automatic method for scoring leg movements in polygraphic sleep recordings and its validity in comparison to visual scoring. Sleep 2004, 27, 324–328. [Google Scholar] [CrossRef]
- Ferri, R.; Zucconi, M.; Manconi, M.; Bruni, O.; Miano, S.; Plazzi, G.; Ferini-Strambi, L. Computer-assisted detection of nocturnal leg motor activity in patients with restless legs syndrome and periodic leg movements during sleep. Sleep 2005, 28, 998–1004. [Google Scholar] [CrossRef]
- Moore, H.; Leary, E.; Lee, S.Y.; Carrillo, O.; Stubbs, R.; Peppard, P.; Young, T.; Widrow, B.; Mignot, E. Design and validation of a periodic leg movement detector. PLoS ONE 2014, 9, e114565. [Google Scholar]
- Carvelli, L.; Olesen, A.N.; Brink-Kjær, A.; Leary, E.B.; Peppard, P.E.; Mignot, E.; Sørensen, H.B.D.; Jennum, P. Design of a deep learning model for automatic scoring of periodic and non-periodic leg movements during sleep validated against multiple human experts. Sleep Med. 2020, 69, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Rauhala, E.; Virkkala, J.; Himanen, S.L. Periodic limb movement screening as an additional feature of Emfit sensor in sleep-disordered breathing studies. J. Neurosci. Methods 2009, 178, 157–161. [Google Scholar] [CrossRef] [PubMed]
- King, M.A.; Jaffre, M.O.; Morrish, E.; Shneerson, J.M.; Smith, I.E. The validation of a new actigraphy system for the measurement of periodic leg movements in sleep. Sleep Med. 2005, 6, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Prill, T.; Fahrenberg, J. Simultaneous assessment of posture and limb movements (e.g., periodic leg movements) with calibrated multiple accelerometry. Physiol. Meas. 2006, 27, N47–N53. [Google Scholar] [CrossRef]
- Ferber, R.; Millman, R.; Coppola, M.; Fleetham, J.; Murray, C.F.; Iber, C.; McCall, W.V.; Nino-Murcia, G.; Pressman, M.; Sanders, M. Portable recording in the assessment of obstructive sleep apnea. ASDA standards of practice. Sleep 1994, 17, 378–392. [Google Scholar] [CrossRef]
- Blank, J.B.; Cawthon, P.M.; Carrion-Petersen, M.L.; Harper, L.; Johnson, J.P.; Mitson, E.; Delay, R.R. Overview of recruitment for the osteoporotic fractures in men study (MrOS). Contemp. Clin. Trial. 2005, 26, 557–568. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-time patient-specific ECG classification by 1-D convolutional neural networks. IEEE Trans. Biomed. Eng. 2016, 63, 664–675. [Google Scholar] [CrossRef]
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. Int. Conf. Mach. Learn. 2015, 37, 448–456. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A Simple Way to Prevent Neural Networks from Overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Agostinelli, F.; Hoffman, M.; Sadowski, P.; Baldi, P. Learning activation functions to improve deep neural networks. arXiv 2014, arXiv:1412.6830. [Google Scholar]
- Dey, D.; Chaudhuri, S.; Munshi, S. Obstructive sleep apnoea detection using convolutional neural network based deep learning framework. Biomed. Eng. Lett. 2018, 8, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Sak, H.; Senior, A.; Beaufays, F. Long short-term memory based recurrent neural network architectures for large vocabulary speech recognition. arXiv 2014, arXiv:1402.1128. [Google Scholar]
- Chung, J.; Gulcehre, C.; Cho, K.; Bengio, Y. Empirical evaluation of gated recurrent neural networks on sequence modeling. arXiv 2014, arXiv:1412.3555. [Google Scholar]
- Nair, V.; Hinton, G.E. Rectified linear units improve restricted boltzmann machines. In Proceedings of the 27th International Conference on Machine Learning, Haifa, Israel, 21–24 June 2010. [Google Scholar]
- Chollet, F. Keras. 2015. Available online: http://keras.io/ (accessed on 7 June 2016).
- TensorFlow. Available online: https://www.tensorflow.org/ (accessed on 7 April 2021).
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar] [CrossRef]
- Ferri, R.; Novelli, L.; Bruni, O. Periodic Limb Movement Disorder. Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Ferri, R.; Koo, B.B.; Picchietti, D.L.; Fulda, S. Periodic leg movements during sleep: Phenotype, neurophysiology, and clinical significance. Sleep Med. 2017, 31, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Haba-Rubio, J.; Marti-Soler, H.; Tobback, N.; Andries, D.; Marques-Vidal, P.; Vollenweider, P.; Preisig, M.; Heinzer, R. Clinical significance of periodic limb movements during sleep: The HypnoLaus study. Sleep Med. 2018, 41, 45–50. [Google Scholar] [CrossRef]
- Hwang, S.R.; Hwang, S.W.; Chen, J.C.; Hwang, J.H. Association of periodic limb movements during sleep and Parkinson disease: A retrospective clinical study. Medicine 2019, 98, e18444. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Normal | PLM |
|---|---|---|
| Subjects (N) | 26 | 26 |
| Age (years) | 76.12 ± 5.51 | 76.08 ± 5.11 |
| Periodic leg movement index (per hour) | 2.46 ± 4.16 | 57.88 ± 30.27 |
| Body mass index (kg/m2) | 27.92 ± 3.12 | 29.15 ± 3.89 |
| Sleep efficiency (%) | 74.35 ± 10.93 | 73.00 ± 11.34 |
| Smoking status, n (%) | ||
| Never Past | 12 (47.15%) 14 (53.85%) | 12 (56.0%) 14 (40.0%) |
| Blood pressure | ||
| Systolic Diastolic | 127.57 ± 12.82 66.85 ± 5.66 | 127.35 ± 19.08 68.81 ± 7.35 |
| Datasets | Normal | PLM | Total |
|---|---|---|---|
| Training set | 33,280 | 33,280 | 66,560 |
| Validation set | 8320 | 8320 | 16,640 |
| Test set | 10,400 | 10,400 | 20,800 |
| Total | 52,000 | 52,000 | 104,000 |
| Datasets | Segment | Precision | Recall | F1-Score | Accuracy |
|---|---|---|---|---|---|
| Training set | Normal | 0.94 | 0.97 | 0.96 | 0.89 |
| PLM | 0.97 | 0.94 | 0.96 | ||
| Validation set | Normal | 0.90 | 0.94 | 0.92 | 0.92 |
| PLM | 0.94 | 0.90 | 0.92 | ||
| Test set | Normal | 0.90 | 0.93 | 0.92 | 0.92 |
| PLM | 0.93 | 0.90 | 0.92 |
| Authors (Year of Publication) | No. of Subjects | Signal | Method | Results (F1-Score) |
|---|---|---|---|---|
| Wetter et al. (2004) [8] | 24 | EMG | EMG-based analytical method | 0.63 |
| Ferri et al. (2005) [9] | 30 | EMG | Computer-assisted detection method | 0.72 |
| Moore et al. (2014) [10] | 1833 | EMG, ECG | Ten-step PLM detection method | 0.79 |
| Carvelli et al. (2020) [11] | 800 | EMG | CNN–LSTM model | 0.85 |
| This work | 52 | ECG | CNN–LSTM model | 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urtnasan, E.; Park, J.-U.; Lee, J.-H.; Koh, S.-B.; Lee, K.-J. Deep Learning for Automatic Detection of Periodic Limb Movement Disorder Based on Electrocardiogram Signals. Diagnostics 2022, 12, 2149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092149
Urtnasan E, Park J-U, Lee J-H, Koh S-B, Lee K-J. Deep Learning for Automatic Detection of Periodic Limb Movement Disorder Based on Electrocardiogram Signals. Diagnostics. 2022; 12(9):2149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092149
Chicago/Turabian StyleUrtnasan, Erdenebayar, Jong-Uk Park, Jung-Hun Lee, Sang-Baek Koh, and Kyoung-Joung Lee. 2022. "Deep Learning for Automatic Detection of Periodic Limb Movement Disorder Based on Electrocardiogram Signals" Diagnostics 12, no. 9: 2149. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092149