

The Role of Thromboprophylaxis in Patients with Portal Vein Thrombosis: A Life-Threatening Complication after Laparoscopic Sleeve Gastrectomy Following 8 Years of Experience in a Bariatric Center of Excellence

Abstract
:1. Introduction
2. Materials and Methods
2.1. Current Anticoagulation Venous Thrombosis Prophylaxis
2.2. PMVT Diagnosis and Treatment
2.3. Statistical Method
3. Results
4. Discussion
- The prolonged use of a liver retractor may result in liver congestion and clot formation [22];
- The ligation of the gastroepiploic and short gastric vessels, resulting in gastric and splenic venous reflux near the splenic vein, could potentially initiate thrombosis, and the thermal effect of energy devices used for ligation can damage the splenic vein via mechanical or thermal effects [1,9,22,23];
- Dehydration is a risk factor for thrombosis [28,29,30,31], especially in LSG patients, due to a reduction in gastric capacity; consequently, in the post-discharge summary for all the LSG patients, we recommend avoiding dehydration and exposure to heat for the first postoperative month and receiving intravenous fluids when they cannot drink 1 L of clear fluid.
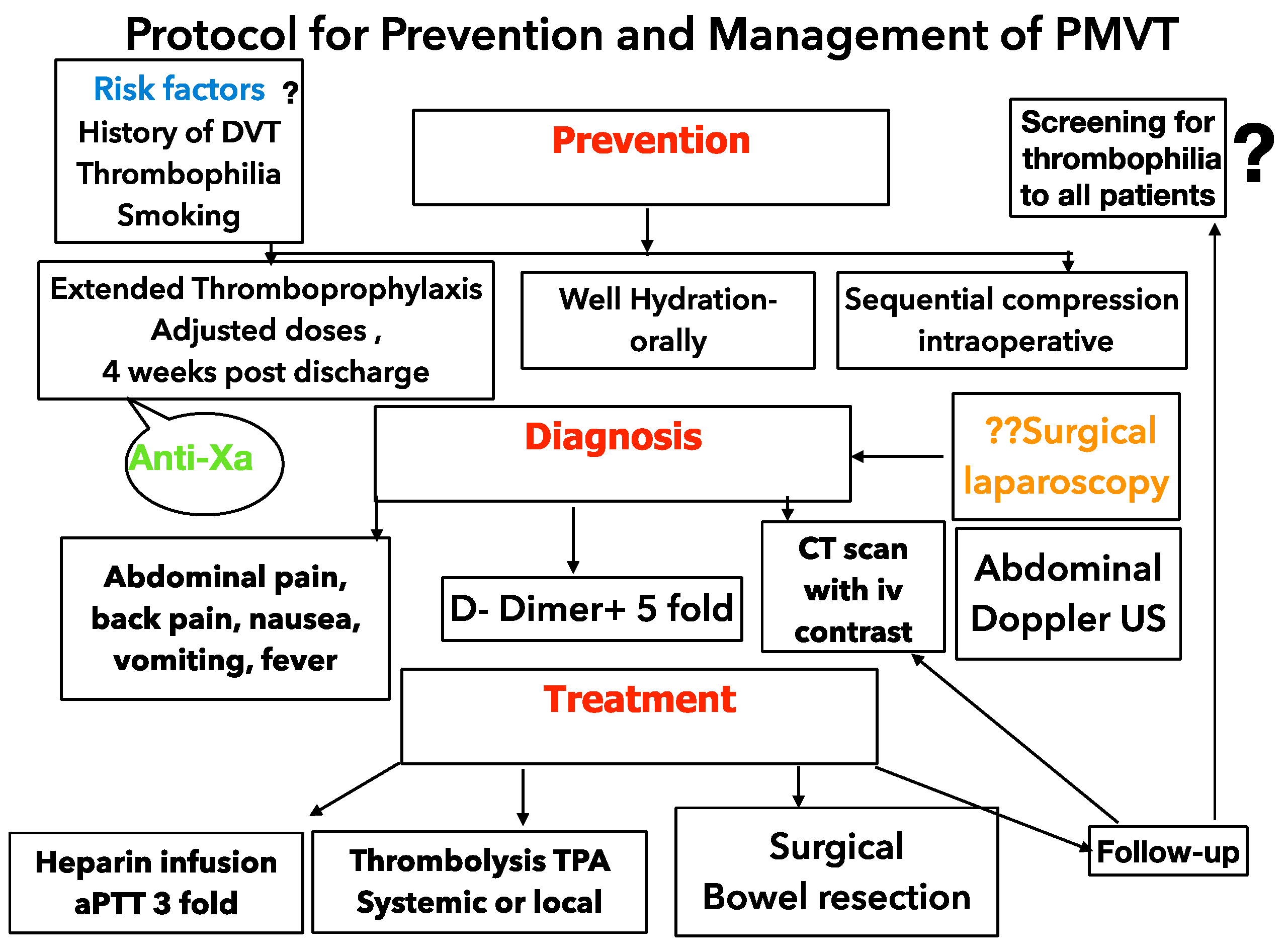
4.1. Treatment
4.2. Prevention
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, A.W.; Rabl, C.; Westphalen, A.C.; Fogarty, P.F.; Posselt, A.M.; Campos, G.M. Portomesenteric Venous Thrombosis After Laparoscopic Surgery: A systematic literature review. Arch. Surg. 2009, 144, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Swartz, D.E.; Felix, E.L. Acute mesenteric venous thrombosis following laparoscopic Roux-en-Y gastric bypass. JSLS 2004, 8, 165–169. [Google Scholar] [PubMed]
- Baixauli, J.; Delaney, C.P.; Senagore, A.J.; Remzi, F.H.; Fazio, V.W. Portal vein thrombosis after laparoscopic sigmoid colectomy for diverticulitis; report of a case. Dis. Colon. Rectum. 2003, 46, 550–553. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Gress, R.E.; Smith, S.C.; Halverson, R.C.; Simper, S.C.; Rosamond, W.D.; LaMonte, M.J.; Stroup, A.M.; Hunt, S.C. Long-term mortality after gastric bypass surgery. N. Engl. J. Med. 2007, 357, 753–761. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, O.; Siejka, J.; Thatigotla, B.; Pham, D.T. A systematic review of portomesenteric vein thrombosis after sleeve gastrectomy. Surg. Obes. Relat. Dis. 2017, 13, 1422–1431. [Google Scholar] [CrossRef]
- Buchwald, H.; Estok, R.; Fahrbach, K.; Banel, D.; Jensen, M.D.; Pories, W.J.; Bantle, J.P.; Sledge, I. Weight and type 2 diabetes after bariatric surgery: Systematic review and meta-analysis. Am. J. Med. 2009, 122, 248–256.e5. [Google Scholar] [CrossRef]
- Goitein, D.; Matter, I.; Raziel, A.; Keida, A.; Hazzan, D.; Rimon, U.; Sakran, N. Portomesenteric thrombosis following laparoscopic bariatric surgery: Incidence, patterns of clinical presentation, and etiology in a bariatric patient population. JAMA Surg. 2013, 148, 340–346. [Google Scholar] [CrossRef]
- Ochner, C.N.; Gibson, C.; Shanik, M.; Goel, V.; Geliebter, A. Changes in neurohormonal gut peptides following bariatric surgery. Int. J. Obes. 2011, 35, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Salinas, J.; Barros, D.; Salgado, N.; Viscido, G.; Funke, R.; Pérez, G.; Pimentel, F.; Boza, C. Portomesenteric vein thrombosis after laparoscopic sleeve gastrectomy. Surg. Endosc. 2014, 28, 1083–1089. [Google Scholar] [CrossRef]
- Plessier, A.; Darwish-Murad, S.; Hernandez-Guerra, M.; Consigny, Y.; Fabris, F.; Trebicka, J.; Heller, J.; Morard, I.; Lasser, L.; Langlet, P.; et al. Acute portal vein thrombosis unrelated to cirrhosis: A prospective multicenter follow-up study. Hepatology 2009, 51, 210–218. [Google Scholar] [CrossRef]
- Godoroja, D.; Copaescu, C. Portal Thrombosis -A Challenging Complication After Sleeve Gastrectomy. In Proceedings of the the 18th World Congress of the International Federation for the Surgery of Obesity & Metabolic Disorders (IFSO), Istanbul, Turkey, 28–31 August 2013; Volume 23, pp. 1017–1243. Available online: http://www.surgicalreview.org/surgeons/data/ (accessed on 26 November 2022).
- Godoroja, D.D.; Copaescu, C.A.; Agache, M.C.; Biro, P. Impact of retrograde transillumination while securing the airway in obese patients undergoing bariatric surgery. J. Clin. Monit. Comput. 2019, 34, 1069–1077. [Google Scholar] [CrossRef]
- Haematology, Anticoagulation and Thrombosis Committee. Medicines Q&As. 2010. Available online: http://vtepreventionnhsengland.org.uk/images/Thromboprophylaxis%20and%20extreme%20weight.doc (accessed on 26 November 2022).
- Nightingale, C.E.; Margarson, M.P.; Shearer, E.; Redman, J.W.; Lucas, D.N.; Cousins, J.M.; Fox, W.T.A.; Kennedy, N.J.; Venn, P.J.; Skues, M.; et al. Peri-operative management of the obese surgical patient 2015 Association of Anaesthetists of Great Britain and Ireland Society for Obesity and Bariatric Anaesthesia. Anaesthesia 2015, 70, 859–876. [Google Scholar]
- Venclauskas, L.; Maleckas, A.; Arcelus, J.I. European guidelines on perioperative venous thromboembolism prophylaxis Surgery in the obese patient ESA VTE Guidelines Task Force. Eur. J. Anaesthesiol. 2018, 35, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Di Lorenzo, N.; Antoniou, S.A.; Rachel, L.; Batterham Busetto, L.; Godoroja, D.; Iossa, A.; Carrano, F.M.; Agresta, F.; Alarçon, I.; Azran, C.; et al. Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: Update 2020 endorsed by IFSO-EC, EASO and ESPCOP. Sur-Gical Endosc. 2020, 34, 2332–2358. [Google Scholar] [CrossRef] [Green Version]
- Godoroja, D.; Hainarosie, D.; Zaharencu, A.; Copaescu, C. Portal Vein Thrombosis a Rare but Life-threatening Complication after Laparoscopic Sleeve Gastrectomy: A 5 Years Study in a Bariatric Center of Excellence. Chirurgia 2019, 114, 6. [Google Scholar] [CrossRef]
- Shoar, S.; Saber, A.A.; Rubenstein, R.; Safari, S.; Brethauer, S.A.; Al-Thani, H.; Asarian, A.P.; Aminian, A. Portomesentric and splenic vein thrombosis (PMSVT) after bariatric surgery: A systematic review of 110 patients. Surg. Obes. Relat. Dis. 2018, 14, 47–59. [Google Scholar] [CrossRef]
- Rottenstreich, A.; Elazary, R.; Yuval, J.B.; Spectre, G.; Kleinstern, G.; Kalish, Y. Assessment of the procoagulant potential after laparoscopic sleeve gastrectomy: A potential role for extended thromboprophylaxis. Surg. Obes. Relat. Dis. 2018, 14, 1–7. [Google Scholar] [CrossRef]
- Luo, L.; Li, H.; Wu, Y.; Bai, Z.; Xu, X.; Wang, L.; Mendez-Sanchez, N.; Qi, X. Portal venous system thrombosis after bariatric surgery: A systematic review and meta-analysis. Surgery 2021, 170, 363–372. [Google Scholar] [CrossRef]
- Villagrán, R.; Smith, G.; Rodriguez, W.; Flores, C.; Cariaga, M.; Araya, S.; Yañez, M.; Fuentes, P.; Linares, J.; Zapata, A. Portomesenteric Vein Thrombosis After Laparoscopic Sleeve Gastrectomy: Incidence, Analysis and Follow-Up in 1236 Consecutive Cases. Obes. Surg. 2016, 26, 2555–2561. [Google Scholar] [CrossRef] [Green Version]
- Kemppainen, E.; Kokkola, A.; Sirén, J.; Kiviluoto, T. Superior Mesenteric and Portal Vein Thrombosis following Laparoscopic Nissen Fundoplication. Dig. Surg. 2000, 17, 279–281. [Google Scholar] [CrossRef]
- Denninger, M.H.; Chat, Y.; Casadevall, N.; Hillaire, S.; Guillin, M.-C.; Bezeaud, A.; Erlinger, S.; Briere, J.; Valla, D. Cause of portal or hepatic venous thrombosis in adults: The role of multiple concurrent factors. Hepatology 2000, 31, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Haglund, U.; Norlen, K.; Rasmussen, I.; Barley, R.W.; Flowers, J.L. Complications related to pneumoperitoneum. In Laparoscopic Surgery; Quality Medical Publishing: St. Louis, MO, USA, 1995; pp. 45–48. [Google Scholar]
- Jakimowicz, J.; Stultiëns, G.; Smulders, F. Laparoscopic insufflation of the abdomen reduces portal venous flow. Surg. Endosc. 1998, 12, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Takagi, S. Hepatic and portal vein blood flow during carbon dioxide pneumoperitoneum for laparoscopic hepatecto-my. Surg. Endosc. 1998, 12, 427–431. [Google Scholar] [CrossRef]
- Becattini, C.; Agnelli, G.; Manina, G.; Noya, G.; Rondelli, F. Venous thromboembolism after laparoscopic bariatric surgery for morbid obesity: Clinical burden and prevention. Surg. Obes. Relat. Dis. 2012, 8, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.; Krahenbuhl, L. Effect of laparoscopy on intraabdominal blood flow. Surgery 2001, 129, 385–389. [Google Scholar] [CrossRef]
- Barba, C.A.; Harrington, C.; Loewen, M. Status of venous thromboembolism prophylaxis among bariatric surgeons: Have we changed our practice during the past decade? Surg. Obes. Relat. Dis. 2009, 5, 352–356. [Google Scholar] [CrossRef]
- Ana, T.; Rocha, M.; de Vasconcellos, Â.G.; da Luz Neto, E.R.; Araújo, D.M.; Alves, E.S.; Lopes, A.A. Risk of venous thromboembolism and efficacy of thromboprophylaxis in hospitalized obese medical patients and in obese patients undergoing bariatric surgery. Obes. Surg. 2006, 16, 1645–1655. [Google Scholar]
- Moon, R.C.; Ghanem, M.; Teixeira, A.F.; De La Cruz-Munoz, N.; Young, M.K.; Domkowski, P.; Radecke, J.; Boyce, S.G.; Rosenthal, R.; Menzo, E.L.; et al. Assessing risk factors, presentation, and management of portomesenteric vein thrombosis after sleeve gastrectomy: A multicenter case-control study. Surg. Obes. Relat. Dis. 2018, 14, 478–483. [Google Scholar] [CrossRef]
- Parikh, M.; Somoza, E.; Chopra, A.; Friedman, D.; Chui, P.; Park, J.; Ude-Welcome, A.; Saunders, J.K. Thrombophilia prevalence in patients seeking laparoscopic sleeve gastrectomy: Extended chemoprophylaxis may decrease portal vein thrombosis rate. Surg. Obes. Relat. Dis. 2020, 16, 839–843. [Google Scholar] [CrossRef]
- Parikh, M.; Adelsheimer, A.; Somoza, E.; Saunders, J.K.; Welcome, A.U.; Chui, P.; Ren-Fielding, C.; Kurian, M.; Fielding, G.; Chopra, A.; et al. Factor VIII elevation may contribute o portomesenteric vein thrombosis after lap-aroscopic sleeve gastrectomy: A multicenter review of 40 patients. Surg. Obes. Rel. Dis. 2017, 13, 1835–1839. [Google Scholar] [CrossRef]
- Bee Ming Tan, S.; Greenslade, J.; Martin, D.; Talbot, M.; Loi, K.; Hopkins, G. Portomesenteric vein thrombosis in sleeve gastrectomy: A 10-year review. Surg. Obes. Relat. Dis. 2018, 14, 271–276. [Google Scholar]
- Sheen, C.; Lamparelli, H.; Milne, A.; Green, I.; Ramage, J. Clinical features, diagnosis and outcome of acute portal vein thrombosis. QJM: Int. J. Med. 2000, 93, 531–534. [Google Scholar] [CrossRef] [Green Version]
- Gertsch, P.; Matthews, J.; Lerut, J.; Luder, P.; Blumgart, L.H. Acute Thrombosis of the Splanchnic Veins. Arch. Surg. 1993, 128, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Kairaluoma, M.; Kärkölä, P.; Heikkinen, E.; Huttunen, R.; Mokka, R.; Larmi, T. Mesenteric infarction. Am. J. Surg. 1977, 133, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, M.S.; Kavanagh, P.V.; Chen, M.Y.; Weber, T.M.; Bechtold, R.E. Noninvasive Assessment of Portomesenteric Venous Thrombosis: Current Concepts and Imaging Strategies. J. Comput. Assist. Tomogr. 2002, 26, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Delhom, E.; Aufort, S.; Shrembi, V.; Lonjon, J.; Bruel, J.M.; Gallix, B. Acute mesenteric ischemia: Value of cross-sectional imaging. J. Radiol. 2011, 92, 1060–1071. [Google Scholar] [CrossRef]
- Sarin, S.K.; Sollano, J.D.; Chawla, Y.K.; Amarapurkar, D.; Hamid, S.; Hashizume, M.; Jafri, W.; Kumar, A.; Kudo, M.; Lesmana, L.A.; et al. Consensus on extra-hepatic portal vein bstruction. Liver Int. 2006, 26, 512–519. [Google Scholar] [CrossRef]
- Condat, B.; Pessione, F.; Hillaire, S.; Denninger, M.-H.; Guillin, M.-C.; Poliquin, M.; Hadengue, A.; Erlinger, S.; Valla, D. Current outcome of portal vein thrombosis in adults: Risk and benefit of anticoagulant therapy. Gastroenterol 2001, 120, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Sarr, M.G.; Kamath, P.S. Mesenteric venous thrombosis. N. Engl. J. Med. 2001, 345, 1683–1688. [Google Scholar] [CrossRef] [Green Version]
- de Franchis, R. Evolving consensus in portal hypertension report of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J. Hepatol. 2005, 43, 167–176. [Google Scholar] [CrossRef]
- Webster, G.J.M.; Burroughs, A.K.; Riordan, S.M. Review article: Portal vein thrombosis - new insights into aetiology and management. Aliment. Pharmacol. Ther. 2004, 21, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Malkowski, P.; Pawlak, J.; Michalowicz, B.; Szczerban, J.; Wroblewski, T.; Leowska, E.; Krawczyk, M. Thrombolytic treatment of portal thrombosis. Hepatogastroenterology 2003, 50, 2098–2100. [Google Scholar]
- Schäfer, C.; Zundler, J.; Bode, C. Thrombolytic therapy in patients with portal vein thrombosis: Case report and review of the literature. Eur. J. Gastroenterol. Hepatol. 2000, 12, 1141–1145. [Google Scholar] [CrossRef]
- Isik, A.; Wysocki, A.P.; Memiş, U.; Sezgin, E.; Yezhikova, A.; Islambekov, Y. Factors Associated with the Occurrence and Healing of Umbilical Pilonidal Sinus: A Rare Clinical Entity. Adv. Ski. Wound Care 2022, 35, 1–4. [Google Scholar] [CrossRef]
- Lazzarin, G.; Di Furia, M.; Romano, L.; Di Sibio, A.; Di Giacomo, C.; Lombardi, L.; Giuliani, A.; Schietroma, M.; Pessia, B.; Carlei, F.; et al. Endoscopic Double-Pigtail Catheter (EDPC) Internal Drainage as First-Line Treatment of Gastric Leak: A Case Series during Laparoscopic Sleeve Gastrectomy Learning Curve for Morbid Obesity. Minim. Invasive Surg. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- LeGrand, B.; Rodgers, G.M.; Cottam, D.; Zaveri, H.; Drury, C.; Surve, A. Portal vein thrombosis after laparoscopic sleeve gas-trectomy:presentation and management. Surg. Relat. Dis. 2016, 12, 1787–1794. [Google Scholar]
- Karaman, K.; Aziret, M.; Bal, A.; Öter, V.; Ercan, M.; Bostancı, E.B. Porto-mesenteric venous thrombosis after laparoscopic sleeve gastrectomy: A case report and systematic review of the 104 cases. Obes. Res. Clin. Pract. 2018, 12, 317–325. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Weight | 50–100 kg | 100–150 kg | Over 150 kg |
|---|---|---|---|
| Dalteparine | 5000 UI | 5000 UI BID | 7500 UI BID |
| Enoxaparine | 40 mg/day | 40 mg BID | 60 mg BID |
| Number of Patients | 5154 |
| Age, median (IQR) (years) | 40 (31–49) |
| BMI, median (IQR) (kg/m2) | 39.4 (34.95–44.55) |
| Male (n-%) | 1565–30.4% |
| Female (n-%) | 3589–69.6% |
| ASAI (n-%) | 413 (8%) |
| ASA II (n-%) | 4000 (77,6%) |
| ASAIII (n-%) | 680(13,1%) |
| ASAIV (n-%) | 61 (1.2%) |
| Patient | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Age | 29 | 40 | 37 | 55 |
| Sex | M | M | M | M |
| BMI (kg/m2) | 50.2 | 38 | 44 | 55,2 |
| Weight (kg) | 160 | 115 | 127 | 146 |
| Time of surgery (min) | 135 | 95 | 60 | 124 |
| Intra-abdominal pressure (mmHg) | 15 | 15 | 15 | 15 |
| History or risk factors of thrombophilia/ DVT | Smoking, hypertension | Double antiplatelet therapy after myocardial infarction and angioplasty | DVT with bilateral PE with anticoagulation–warfarin and antiplatelet therapy | Smoking, hypertension |
| Days after LSG | 12 | 60 | 8 | 34 |
| LMWH prophylaxis for 21 days | Dalteparine 7500 ui sc BID | Dalteparine 5000 ui BID | Enoxaparine 80 mg BID(therapeutic range for 8 days) | Enoxaparine (60 mg BID) |
| Clinical signs | Abdominal pain, nausea, vomiting | Diffuse abdominal pain (epigastrium) nausea, constipation | Altered general state, severe tachycardia BP100/60, fever, cold sweating, diffuse abdominal pain, tenderness in left and right hypochondrium and lumbar, nausea, vomiting, fulminant evolution to shock, lactate (>15 mmol/L) | Abdominal pain, fever, nausea |
| Dimers at admission ng/ml | 5400 | 7500 | 100,000 | 4400 |
| Doppler ultrasound | Partial PVT | Partial PVT | Complete PVT | Partial PVT |
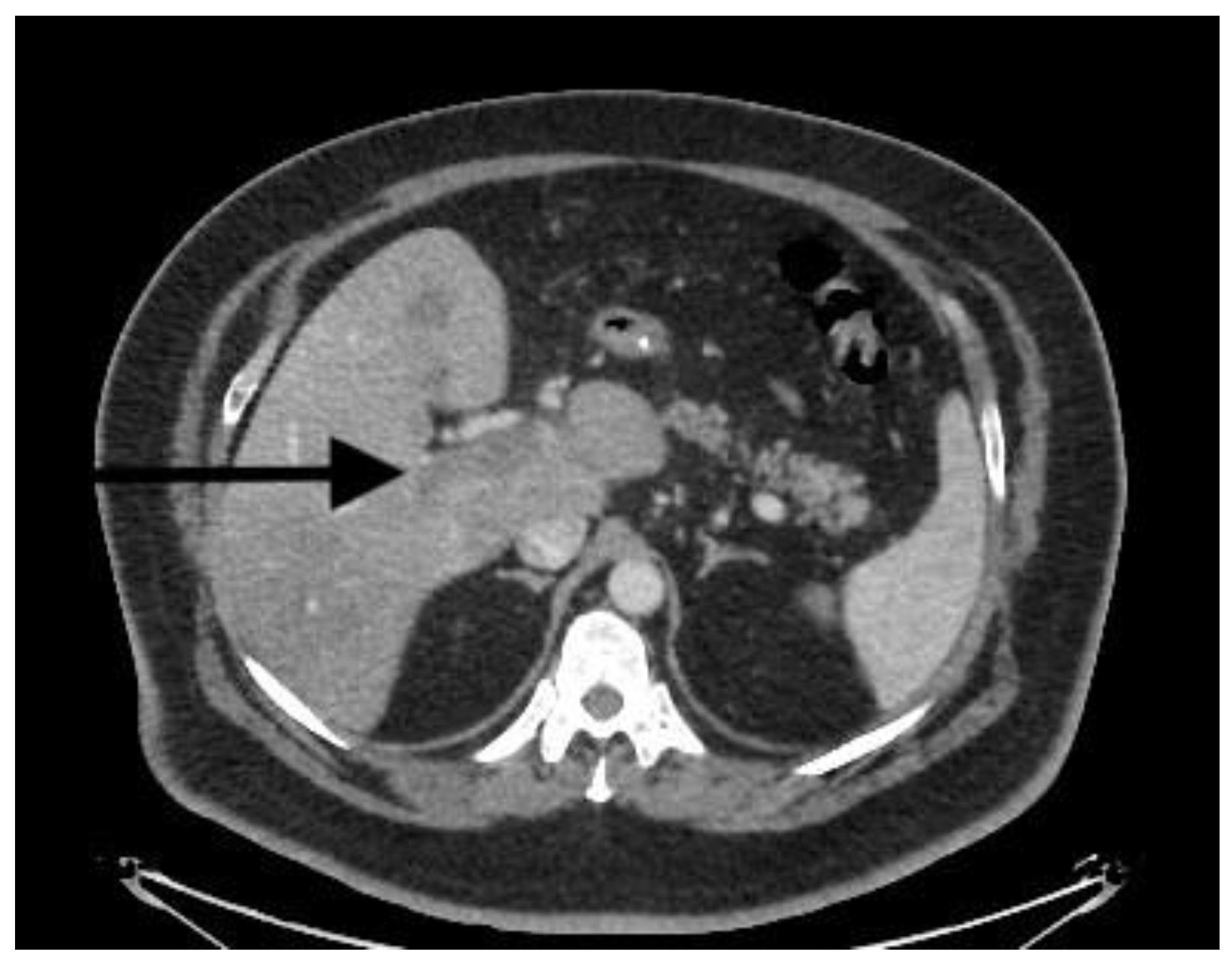
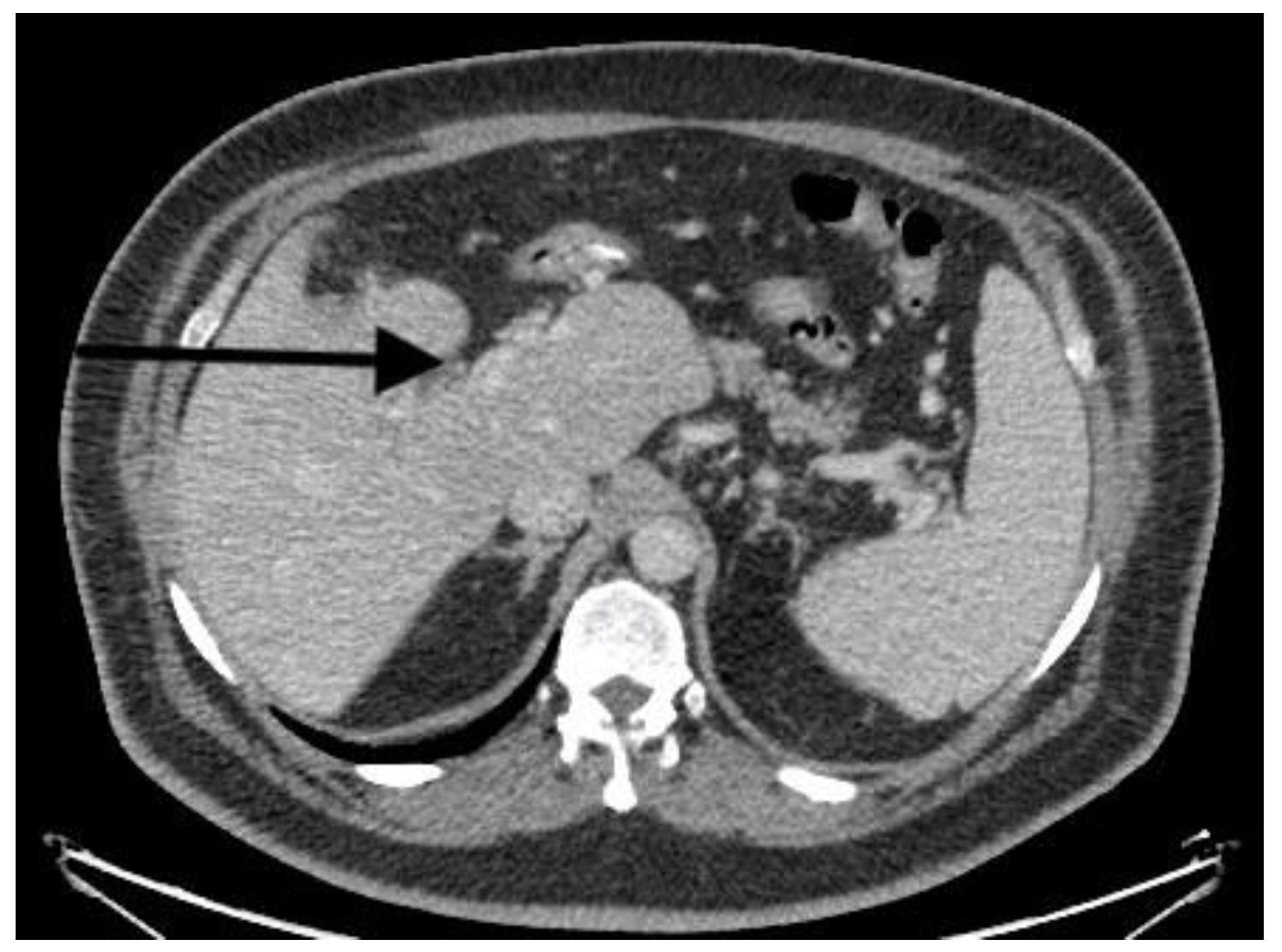
| CT scan | Nonocclusive PVT, posterior right branch, and partial superior mesenteric vein | Nonocclusive PVT, right branch, and partial superior mesenteric vein | Extensive occlusive, portal, splenic, and mesenteric thrombosis; ascites evidence of small-bowel hypoperfusion | Partial PVT |
| Heparin infusion | 12 days (aPTT 2,5X) | 3 days (aPTT 2,5X) | 2 h | 3 days, then LMWH for 5 days |
| Long-term anticoagulation | Apixaban (5 mg BD) | Warfarin (INR) | - | Apixaban (5 mg BD) |
| Thrombolysis tPA | no | no | no | no |
| Surgery | no | no | no | no |
| Hospital stay (days) | 13 | 6 | 2 h | 8 |
| Mortality | no | no | yes | no |
| Follow-up | Clot regression, no recurrence of PMVT | Clot regression, no recurrence of PMVT | - | Clot regression, no recurrence of PMVT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godoroja-Diarto, D.; Copaescu, C.; Rusu, E.; Constantin, A. The Role of Thromboprophylaxis in Patients with Portal Vein Thrombosis: A Life-Threatening Complication after Laparoscopic Sleeve Gastrectomy Following 8 Years of Experience in a Bariatric Center of Excellence. Diagnostics 2023, 13, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13010043
Godoroja-Diarto D, Copaescu C, Rusu E, Constantin A. The Role of Thromboprophylaxis in Patients with Portal Vein Thrombosis: A Life-Threatening Complication after Laparoscopic Sleeve Gastrectomy Following 8 Years of Experience in a Bariatric Center of Excellence. Diagnostics. 2023; 13(1):43. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13010043
Chicago/Turabian StyleGodoroja-Diarto, Daniela, Catalin Copaescu, Elena Rusu, and Alina Constantin. 2023. "The Role of Thromboprophylaxis in Patients with Portal Vein Thrombosis: A Life-Threatening Complication after Laparoscopic Sleeve Gastrectomy Following 8 Years of Experience in a Bariatric Center of Excellence" Diagnostics 13, no. 1: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13010043