
Clinical Decision Support System to Detect the Occurrence of Ventilator-Associated Pneumonia in Pediatric Intensive Care

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
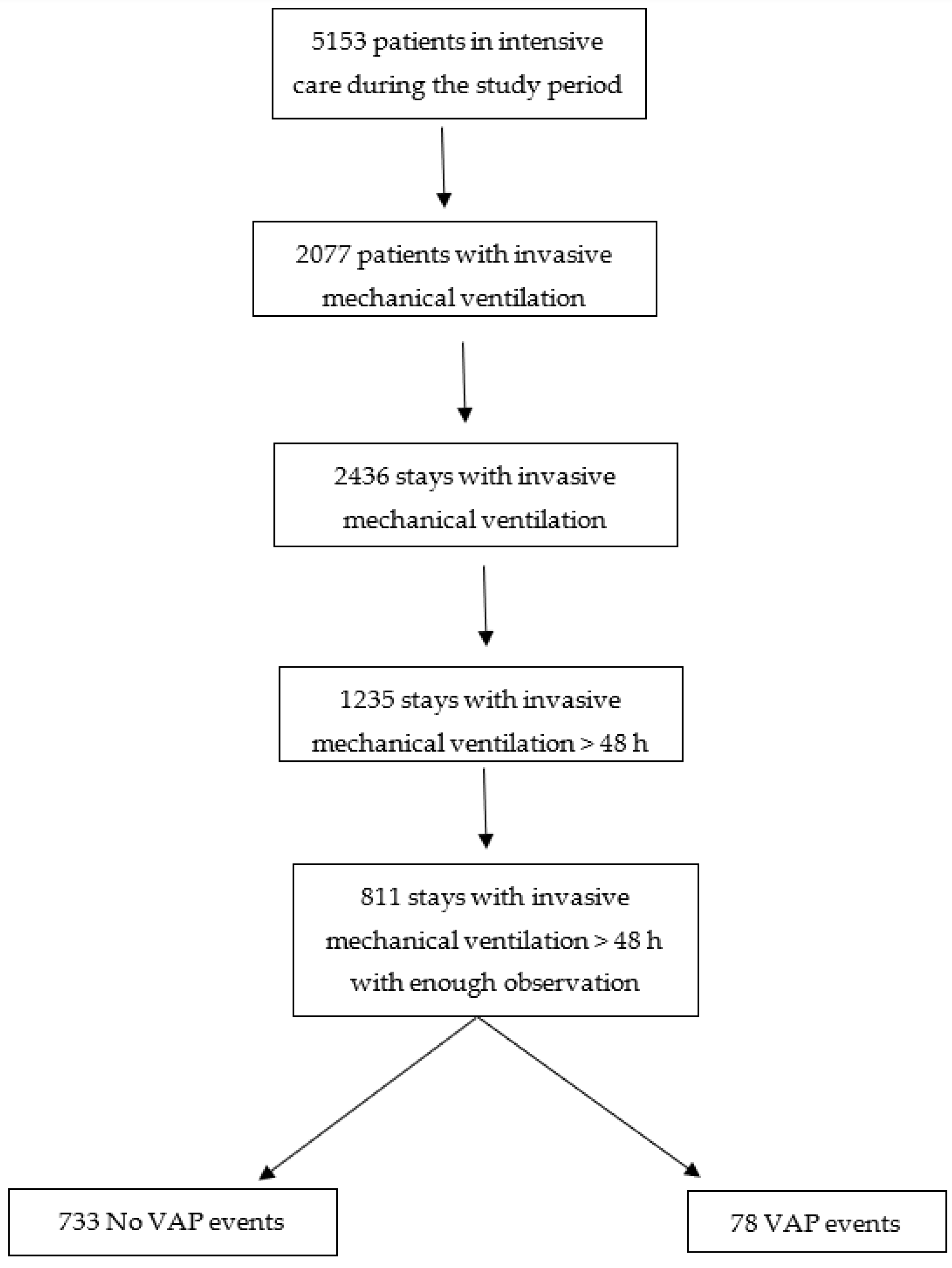
3.1. General Description of the Population
3.2. Missing Data
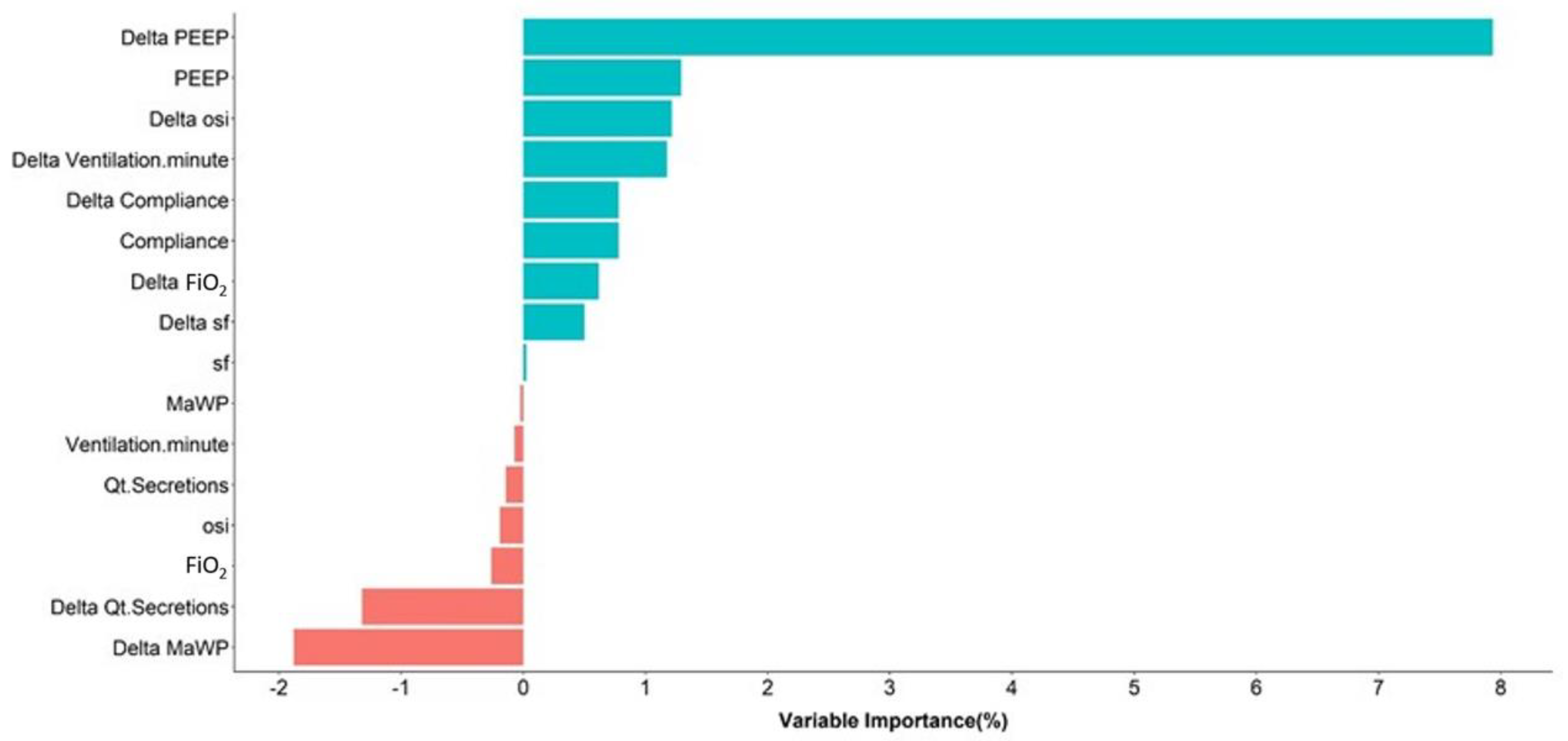
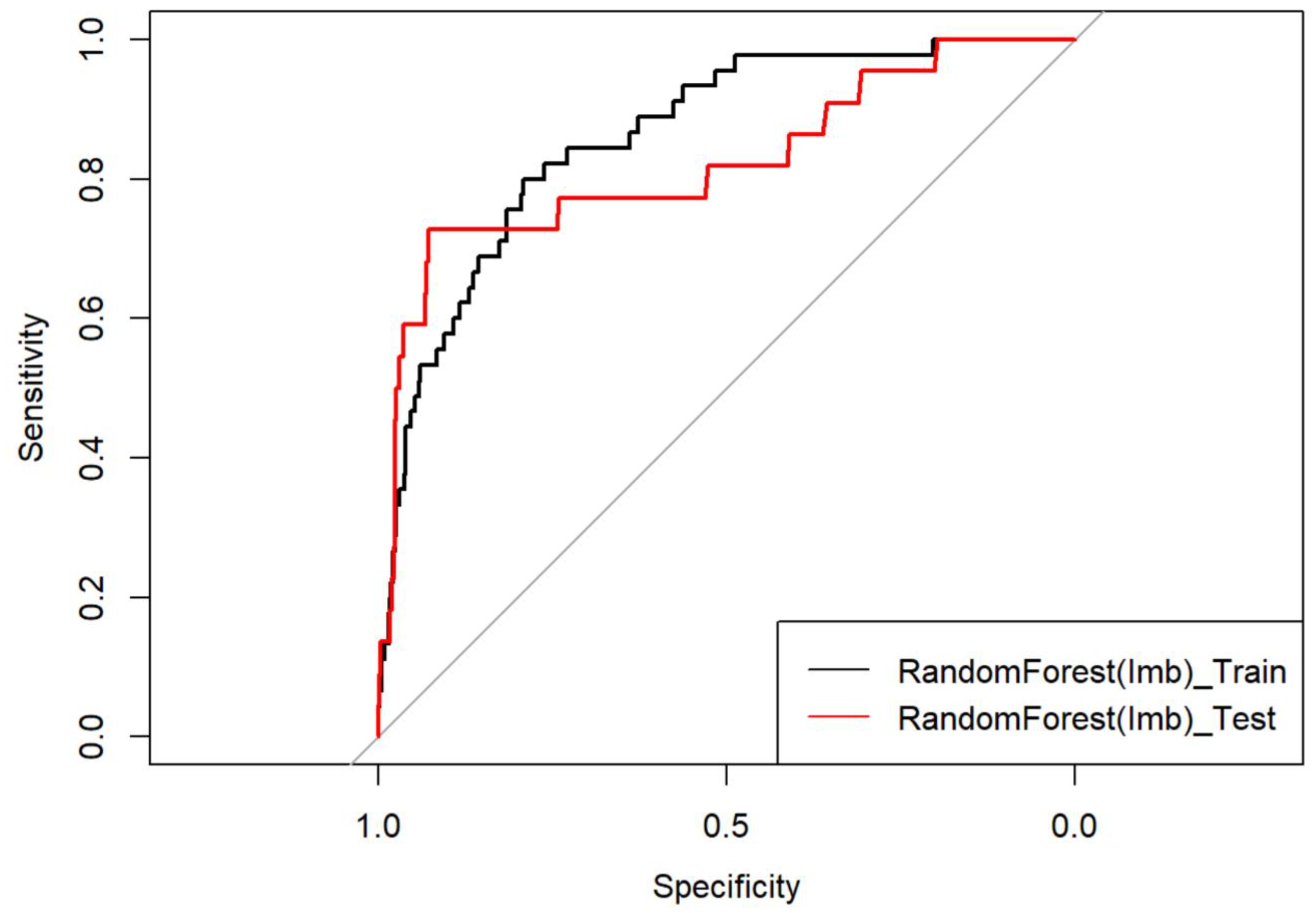
3.3. Results of Training Algorithm
3.4. Performance on Test Dataset
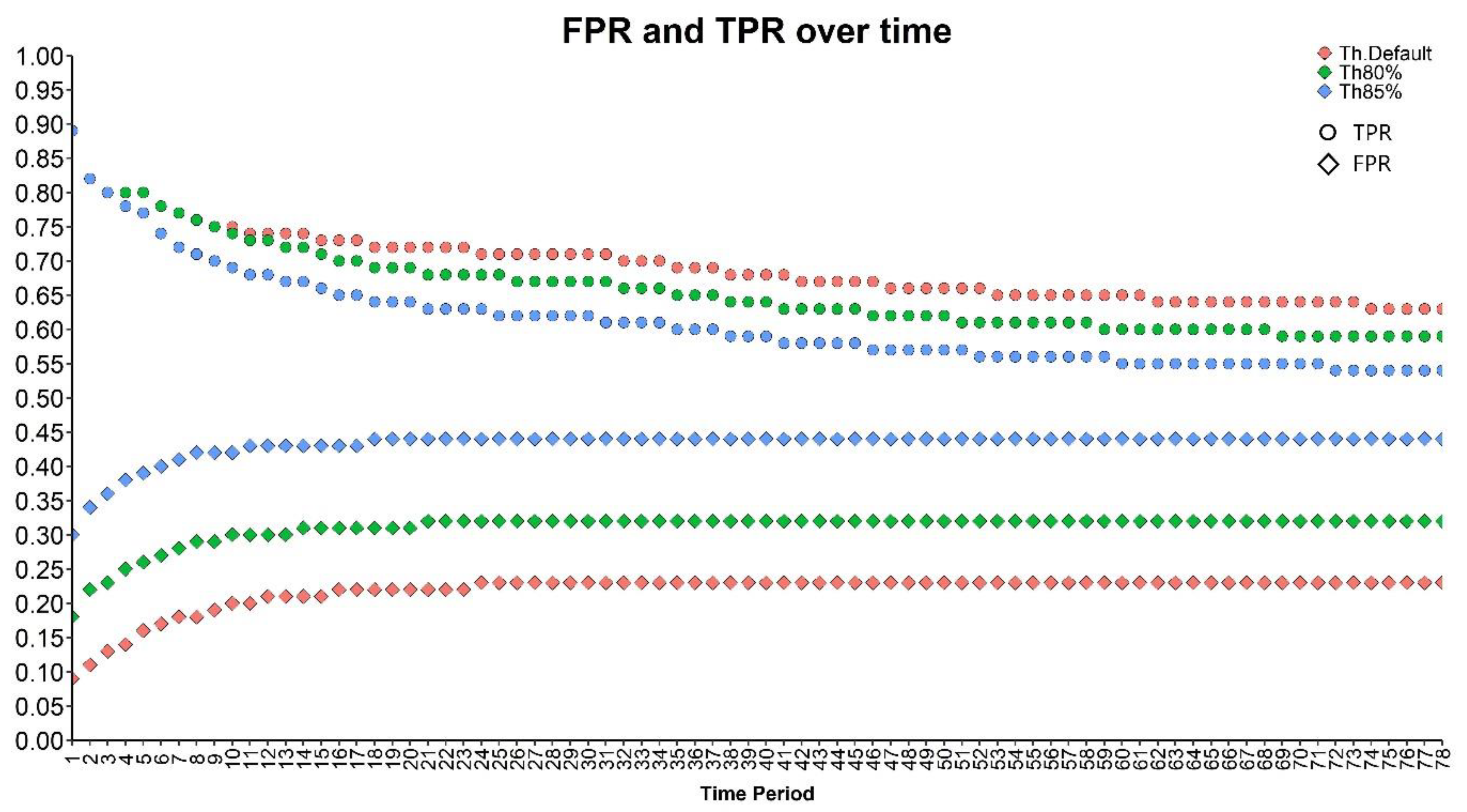
3.5. Per Patient Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | area under the curve |
| CDC | centers for disease control |
| CDSS | clinical decision support systems |
| FiO2 | inspired fraction of oxygen |
| FPR | false positive rates |
| ICCA | Intelligence Critical Care and Anesthesia® |
| MAwP | mean airway pressure |
| OI | oxygenation index |
| OSI | oxygenation and saturation index |
| PaCO2 | partial pressure of carbon dioxide |
| PaO2 | partial pressure of oxygen |
| PELOD-2 | pediatric logistic organ dysfunction score |
| PEEP | positive end-expiratory pressure |
| PICU | pediatric intensive care unit |
| PIM 2 | pediatric index of mortality |
| PIP | peak inspiratory pressure |
| ROC | receiving operator curve |
| TPR | true positive rates |
| VAE | ventilator-associated event |
| VAP | ventilator-associated pneumonia |
References
- Center for Disease Control. 2018. Available online: https://www.cdc.gov/nhsn/PDFs/pscManual/6pscVAPcurrent.pdf (accessed on 14 September 2023).
- Chastre, J.; Fagon, J.-Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.M.M.; Borromeo, A.R.; Dueño, A.L.; Paragas, E.D.; Ellasus, R.O.; Abalos-Fabia, R.S.; Abriam, J.A.; Sonido, A.E.; Hernandez, M.A.; Generale, A.J.A.; et al. Clinical epidemiology and outcomes of ventilator-associated pneumonia in critically ill adult patients: Protocol for a large-scale systematic review and planned meta-analysis. Syst. Rev. 2019, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Klompas, M.; Luyt, C.-E. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef]
- Tullu, M.S.; Balasubramanian, P. Ventilator-Associated Pneumonia in Pediatric Intensive Care Unit: Correspondence. Indian J. Pediatr. 2015, 82, 662–663. [Google Scholar] [CrossRef]
- Shaath, G.A.; Jijeh, A.; Faruqui, F.; Bullard, L.; Mehmood, A.; Kabbani, M.S. Ventilator-associated pneumonia in children after cardiac surgery. Pediatr. Cardiol. 2014, 35, 627–631. [Google Scholar] [CrossRef]
- Ericson, J.E.; McGuire, J.; Michaels, M.G.; Schwarz, A.; Frenck, R.; Deville, J.G.; Agarwal, S.; Bressler, A.M.; Gao, J.; Spears, T.; et al. Hospital-acquired Pneumonia and Ventilator-associated Pneumonia in Children: A Prospective Natural History and Case-Control Study. Pediatr. Infect. Dis. J. 2020, 39, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Cirulis, M.M.; Hamele, M.T.; Stockmann, C.R.; Bennett, T.D.; Bratton, S.L. Comparison of the New Adult Ventilator-Associated Event Criteria to the Centers for Disease Control and Prevention Pediatric Ventilator-Associated Pneumonia Definition (PNU2) in a Population of Pediatric Traumatic Brain Injury Patients. Pediatr. Crit. Care Med. 2016, 17, 157–164. [Google Scholar] [CrossRef]
- Chomton, M.; Brossier, D.; Sauthier, M.; Vallières, E.; Dubois, J.; Emeriaud, G.; Jouvet, P. Ventilator-Associated Pneumonia and Events in Pediatric Intensive Care: A Single Center Study. Pediatr. Crit. Care Med. 2018, 19, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Giannini, H.M.; Ginestra, J.C.; Chivers, C.; Draugelis, M.; Hanish, A.; Schweickert, W.D.; Fuchs, B.D.; Meadows, L.; Lynch, M.; Donnelly, P.J.; et al. A Machine Learning Algorithm to Predict Severe Sepsis and Septic Shock: Development, Implementation, and Impact on Clinical Practice. Crit. Care Med. 2019, 47, 1485–1492. [Google Scholar] [CrossRef]
- Chen, C.-H.; Lee, Y.-W.; Huang, Y.-S.; Lan, W.-R.; Chang, R.-F.; Tu, C.-Y.; Chen, C.-Y.; Liao, W.-C. Computer-aided diagnosis of endobronchial ultrasound images using convolutional neural network. Comput. Methods Programs Biomed. 2019, 177, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Roggeveen, L.F.; Guo, T.; Driessen, R.H.; Fleuren, L.M.; Thoral, P.; van der Voort, P.H.J.; Girbes, A.R.J.; Bosman, R.J.; Elbers, P. Right Dose, Right Now: Development of AutoKinetics for Real Time Model Informed Precision Antibiotic Dosing Decision Support at the Bedside of Critically Ill Patients. Front. Pharmacol. 2020, 11, 646. [Google Scholar] [CrossRef] [PubMed]
- Lauritsen, S.M.; Kalør, M.E.; Kongsgaard, E.L.; Lauritsen, K.M.; Jørgensen, M.J.; Lange, J.; Thiesson, B. Early detection of sepsis utilizing deep learning on electronic health record event sequences. Artif. Intell. Med. 2020, 104, 101820. [Google Scholar] [CrossRef]
- Wulff, A.; Haarbrandt, B.; Tute, E.; Marschollek, M.; Beerbaum, P.; Jack, T. An interoperable clinical decision-support system for early detection of SIRS in pediatric intensive care using openEHR. Artif. Intell. Med. 2018, 89, 10–23. [Google Scholar] [CrossRef]
- Brossier, D.; El Taani, R.; Sauthier, M.; Roumeliotis, N.; Emeriaud, G.; Jouvet, P. Creating a High-Frequency Electronic Database in the PICU: The Perpetual Patient. Pediatr. Crit. Care Med. 2018, 19, e189–e198. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Harhay, M.O.; Lederer, D.J.; Abramson, M.; Adjei, A.A.; Bakker, J.; Ballas, Z.K.; Barreiro, E.; Bell, S.C.; Bellomo, R.; et al. Development and Reporting of Prediction Models: Guidance for Authors From Editors of Respiratory, Sleep, and Critical Care Journals. Crit. Care Med. 2020, 48, 623–633. [Google Scholar] [CrossRef]
- Mack, E.H.; Wheeler, D.S.; Embi, P.J. Clinical decision support systems in the pediatric intensive care unit. Pediatr. Crit. Care Med. 2009, 10, 23–28. [Google Scholar] [CrossRef]
- DesPrez, K.; McNeil, J.B.; Wang, C.; Bastarache, J.A.; Shaver, C.M.; Ware, L.B. Oxygenation Saturation Index Predicts Clinical Outcomes in ARDS. Chest 2017, 152, 1151–1158. [Google Scholar] [CrossRef]
- Slater, A.; Shann, F.; Pearson, G.; Paediatric Index of Mortality (PIM) Study Group. PIM2: A revised version of the Paediatric Index of Mortality. Intensive Care Med. 2003, 29, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Leteurtre, S.; Duhamel, A.; Salleron, J.; Grandbastien, B.; Lacroix, J.; Leclerc, F.; Groupe Francophone de Réanimation et d’Urgences Pédiatriques (GFRUP). PELOD-2: An update of the PEdiatric logistic organ dysfunction score. Crit. Care Med. 2013, 41, 1761–1773. [Google Scholar] [CrossRef]
- Sauthier, M.; Landry-Hould, F.; Leteurtre, S.; Kawaguchi, A.; Emeriaud, G.; Jouvet, P. Comparison of the Automated Pediatric Logistic Organ Dysfunction-2 Versus Manual Pediatric Logistic Organ Dysfunction-2 Score for Critically Ill Children. Pediatr. Crit. Care Med. 2020, 21, e160–e169. [Google Scholar] [CrossRef]
- Breiman, L. Breiman and Cutler’s Random Forests for Classification and Regression, R package version 4.6-14 [Internet]. 2018. Available online: https://cran.r-project.org/web/packages/randomForest/randomForest.pdf (accessed on 14 September 2023).
- Available online: https://cran.r-project.org/web/packages/randomForestSRC/randomForestSRC.pdf (accessed on 14 September 2023).
- Chen, C.; Liaw, A.; Breiman, L. Using Random Forest to Learn Imbalanced Data; University of California: Los Angeles, CA, USA, 2004. [Google Scholar]
- Ishwaran, H. Fast Unified Random Forests for Survival, Regression, and Classification (RF-SRC). R Package Version 2.9.3. [Internet]. 2020. Available online: https://cran.rproject.org/web/packages/randomForestSRC/randomForestSRC.pdf (accessed on 14 September 2023).
- Kuhn, M. Training on Classification and Regression, R Package Version 6.0.86. Available online: https://cran.r-project.org/web/packages/caret/caret.pdf (accessed on 14 September 2023).
- Cernada, M.; Aguar, M.; Brugada, M.; Gutiérrez, A.; López, J.L.; Castell, M.; Vento, M. Ventilator-associated pneumonia in newborn infants diagnosed with an invasive bronchoalveolar lavage technique: A prospective observational study. Pediatr. Crit. Care Med. 2013, 14, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Elward, A.M.; Warren, D.K.; Fraser, V.J. Ventilator-associated pneumonia in pediatric intensive care unit patients: Risk factors and outcomes. Pediatrics 2002, 109, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Sajedi, M. VAP-Predictive-Model, GitHub repository [Internet]. 2021. Available online: https://github.com/SajediM/VAP-Predictive-Model (accessed on 30 September 2020).
- Jouvet, P.A.; Payen, V.; Gauvin, F.; Emeriaud, G.; Lacroix, J. Weaning children from mechanical ventilation with a computer-driven protocol: A pilot trial. Intensive Care Med. 2013, 39, 919–925. [Google Scholar] [CrossRef]
- Zaglam, N.; Jouvet, P.; Flechelles, O.; Emeriaud, G.; Cheriet, F. Computer-aided diagnosis system for the Acute Respiratory Distress Syndrome from chest radiographs. Comput. Biol. Med. 2014, 52, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Mazo, C.; Kearns, C.; Mooney, C.; Gallagher, W.M. Clinical Decision Support Systems in Breast Cancer: A Systematic Review. Cancers 2020, 12, 369. [Google Scholar] [CrossRef] [PubMed]
- Ostropolets, A.; Zhang, L.; Hripcsak, G. A scoping review of clinical decision support tools that generate new knowledge to support decision making in real time. J. Am. Med. Inform. Assoc. 2020, 27, 1968–1976. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population Characteristics | Global Population (N: 827) | VAP Patients (N: 77) | No VAP Patients (N: 750) | p: |
|---|---|---|---|---|
| Weight (kg) | 15.8 ± 1.6 | 20.99 ± 2.7 | 15.25 ± 0.7 | 0.01 |
| Age (days) | 1308 ± 1904 | 1806 ± 250 | 1256 ± 69 | 0.02 |
| Gender male (%) | 475 (57%) | 41 (53%) | 434 (58%) | 0.4 |
| Pelod 2 score | 10.1 ± 4.8 | 10.4 ± 0.6 | 9.9 ± 0.2 | 0.47 |
| Pelod 2 mortality risk (%) | 0.3 ± 0.3 | 0.3 ± 0.1 | 0.2 ± 0.01 | 0.15 |
| Bronchoscopie (%) | 70 (8%) | 14 (18%) | 56 (8%) | 0.04 |
| Neuromuscular blocker (%) | 279 (34%) | 43 (55%) | 236 (31%) | <0.0001 |
| Mechanical Ventilation duration (days) | 12.5 ± 30.9 | 29.3 ± 5.1 | 10.9 ± 1.5 | <0.0001 |
| PICU length of stay (days) | 26.1 ± 52.5 | 48.3 ± 7.1 | 23.4 ± 1.8 | <0.0001 |
| Survival rate (%) | 740 (90%) | 65 (84%) | 675 (90%) | 0.16 |
| Train and Test Groups Characteristics | Test Group (n: 261) | Train Group (n: 572) | p: |
|---|---|---|---|
| Weight (kg) | 16.9 ± 1.3 | 15.6 ± 0.8 | 0.40 |
| Age (days) | 1387 ± 129 | 1268 ± 84 | 0.43 |
| Gender male, (n, %) | 146 (60) | 284 (58) | 0.69 |
| Pelod 2 score | 10.4 ± 0.2 | 9.7 ± 0.5 | 0.16 |
| Pelod 2 mortality risk (%) | 0.3 ± 0.1 | 0.2 ± 0.1 | 0.13 |
| Proportion of VAP patients (n, %) | 25 (10) | 50 (10) | 0.99 |
| Length of mechanical ventilation before VAP (days) | 9.9 ± 2.7 | 9.6 ± 1.9 | 0.66 |
| Length of mechanical ventilation duration (days) | 12.1 ± 1.6 | 11.2 ± 1.1 | 0.64 |
| PICU length of stay (days) | 21.3 ± 2.4 | 22.3 ± 2.0 | 0.81 |
| Threshold | Specificity | Sensitivity |
|---|---|---|
| 0.41 | 0.79 | 0.80 |
| 0.29 | 0.64 | 0.87 |
| 0.25 | 0.58 | 0.91 |
| 0.22 | 0.52 | 0.96 |
| Threshold | Specificity | Sensitivity |
|---|---|---|
| 0.41 | 0.797 | 0.73 |
| 0.28 | 0.66 | 0.77 |
| 0.25 | 0.59 | 0.77 |
| 0.22 | 0.53 | 0.82 |
| G1 | G2 | |||||
|---|---|---|---|---|---|---|
| ER.Pred | ER.Pred.th80 | ER.Pred.th85 | ER.Pred | ER.Pred.th80 | ER.Pred.th85 | |
| All | 11.56 | 19.60 | 31.66 | 79.59 | 83.67 | 95.92 |
| VAP | 23.08 | 23.08 | 23.08 | 66.67 | 66.67 | 88.89 |
| NoVAP | 10.75 | 19.35 | 32.26 | 82.50 | 87.50 | 97.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rambaud, J.; Sajedi, M.; Al Omar, S.; Chomtom, M.; Sauthier, M.; De Montigny, S.; Jouvet, P. Clinical Decision Support System to Detect the Occurrence of Ventilator-Associated Pneumonia in Pediatric Intensive Care. Diagnostics 2023, 13, 2983. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13182983
Rambaud J, Sajedi M, Al Omar S, Chomtom M, Sauthier M, De Montigny S, Jouvet P. Clinical Decision Support System to Detect the Occurrence of Ventilator-Associated Pneumonia in Pediatric Intensive Care. Diagnostics. 2023; 13(18):2983. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13182983
Chicago/Turabian StyleRambaud, Jerome, Masoumeh Sajedi, Sally Al Omar, Maryline Chomtom, Michael Sauthier, Simon De Montigny, and Philippe Jouvet. 2023. "Clinical Decision Support System to Detect the Occurrence of Ventilator-Associated Pneumonia in Pediatric Intensive Care" Diagnostics 13, no. 18: 2983. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13182983