

Diagnostic Algorithm Based on Machine Learning to Predict Complicated Appendicitis in Children Using CT, Laboratory, and Clinical Features
Abstract
:1. Introduction
2. Theory, Equipment, and Methods
2.1. Patient
2.2. Laboratory and Clinical Findings
2.3. CT Acquisition
2.4. Image Analysis
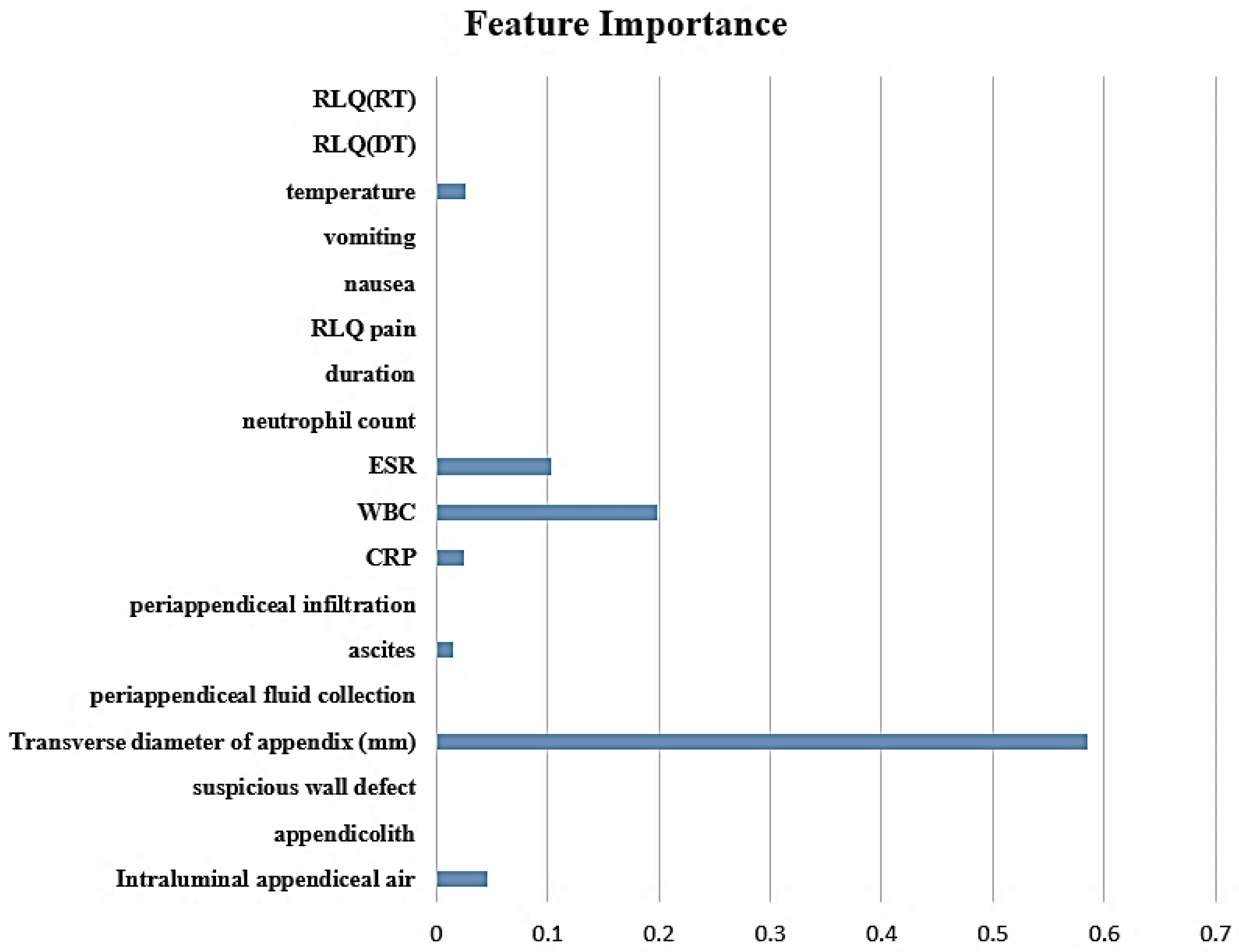
2.5. Feature Selection and Constructing Decision Tree Model
2.6. Statistical Analysis
3. Results
3.1. Baseline Character
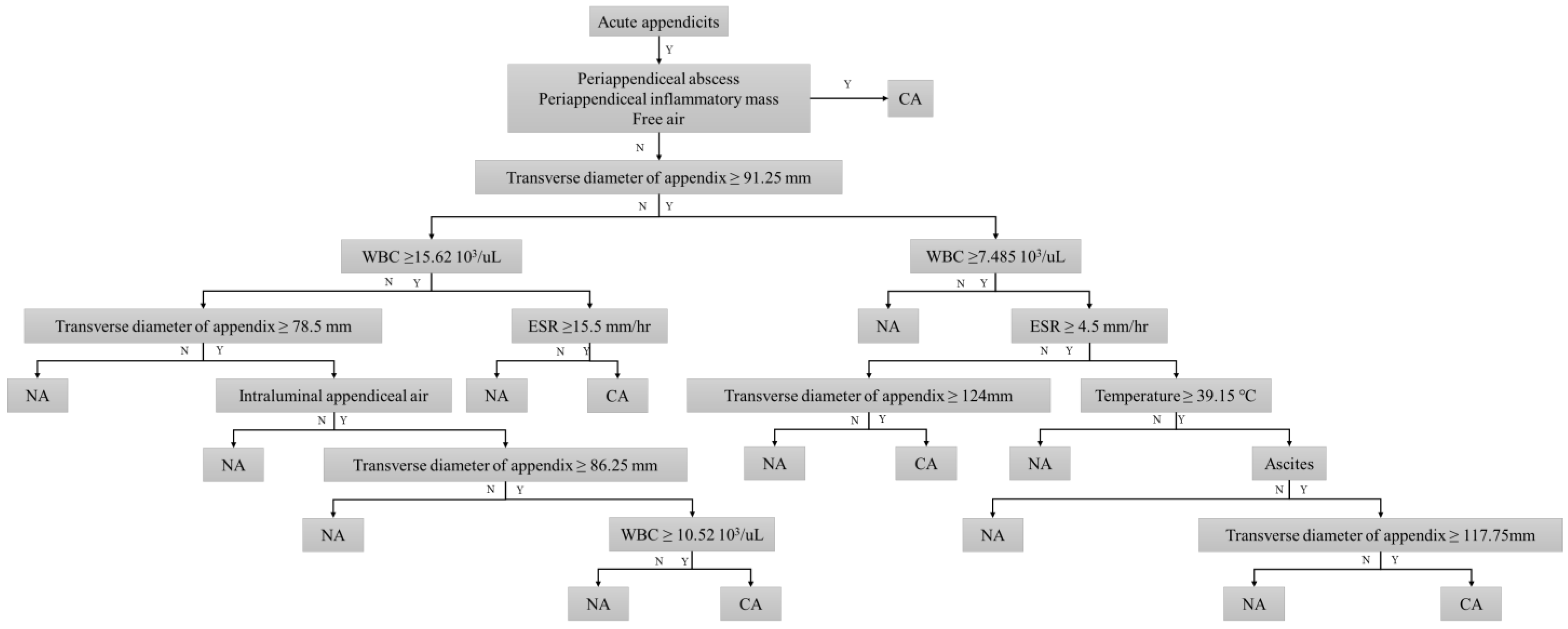
3.2. Decision Tree Model for Discriminating Complicated Appendicitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Periappendiceal Abscess | Periappendiceal Inflammatory Mass | Free Air | Intraluminal Appendiceal Air | Appendicolith | Suspicious Wall Defect | Transverse Diameter of Appendix (mm) † | Periappendiceal Fluid Collection | Ascites | Periappendiceal Infiltration | |
|---|---|---|---|---|---|---|---|---|---|---|
| Kappa | 1 | 1 | 1 | 0.98 | 0.97 | 0.88 | 0.92 | 0.87 | 0.94 | 0.87 |
| 95% CI | 1.00, 1.00 | 1.00, 1.00 | 1.00, 1.00 | 0.95, 1.00 | 0.95, 1.00 | 0.80, 0.94 | 0.90, 0.93 | 0.80, 0.94 | 0.90, 0.98 | 0.80, 0.93 |
References
- Kim, M.S.; Park, H.W.; Park, J.Y.; Park, H.J.; Lee, S.Y.; Hong, H.P.; Kwag, H.J.; Kwon, H.J. Differentiation of early perforated from nonperforated appendicitis: MDCT findings, MDCT diagnostic performance, and clinical outcome. Abdom. Imaging 2014, 39, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Fox, S.M. Pediatric Abdominal Pain: An Emergency Medicine Perspective. Emerg. Med. Clin. N. Am. 2016, 34, 341–361. [Google Scholar] [CrossRef] [PubMed]
- Rothrock, S.G.; Skeoch, G.; Rush, J.J.; Johnson, N.E. Clinical features of misdiagnosed appendicitis in children. Ann. Emerg. Med. 1991, 20, 45–50. [Google Scholar] [CrossRef]
- Dadeh, A.A.; Puitong, K. Predictive Factors to Diagnose Appendicitis in Children in the Emergency Department. Open Access Emerg. Med. 2021, 13, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Elliston, C.D.; Hall, E.J.; Berdon, W.E. Estimated risks of radiation-induced fatal cancer from pediatric CT. Am. J. Roentgenol. 2001, 176, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyzer, C.; Zalcman, M.; De Maertelaer, V.; Coppens, E.; Bali, M.A.; Gevenois, P.A.; Van Gansbeke, D. Comparison of US and unenhanced multi-detector row CT in patients suspected of having acute appendicitis. Radiology 2005, 236, 527–534. [Google Scholar] [CrossRef]
- Lane, M.J.; Katz, D.S.; Ross, B.A.; Clautice-Engle, T.L.; Mindelzun, R.E.; Jeffrey, R.B., Jr. Unenhanced helical CT for suspected acute appendicitis. AJR Am. J. Roentgenol. 1997, 168, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Lane, M.J.; Liu, D.M.; Huynh, M.D.; Jeffrey, R.B., Jr.; Mindelzun, R.E.; Katz, D.S. Suspected acute appendicitis: Nonenhanced helical CT in 300 consecutive patients. Radiology 1999, 213, 341–346. [Google Scholar] [CrossRef]
- Rao, P.M.; Rhea, J.T.; Novelline, R.A.; McCabe, C.J.; Lawrason, J.N.; Berger, D.L.; Sacknoff, R. Helical CT technique for the diagnosis of appendicitis: Prospective evaluation of a focused appendix CT examination. Radiology 1997, 202, 139–144. [Google Scholar] [CrossRef]
- Rao, P.M.; Rhea, J.T.; Novelline, R.A.; Mostafavi, A.A.; McCabe, C.J. Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N. Engl. J. Med. 1998, 338, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Rhea, J.T.; Halpern, E.F.; Ptak, T.; Lawrason, J.N.; Sacknoff, R.; Novelline, R.A. The status of appendiceal CT in an urban medical center 5 years after its introduction: Experience with 753 patients. AJR Am. J. Roentgenol. 2005, 184, 1802–1808. [Google Scholar] [CrossRef] [PubMed]
- Horrow, M.M.; White, D.S.; Horrow, J.C. Differentiation of perforated from nonperforated appendicitis at CT. Radiology 2003, 227, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Andersson, R.E. The appendicitis inflammatory response score: A tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J. Surg. 2008, 32, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Pham, X.-B.D.; Sullins, V.F.; Kim, D.Y.; Range, B.; Kaji, A.H.; de Virgilio, C.M.; Lee, S.L. Factors predictive of complicated appendicitis in children. J. Surg. Res. 2016, 206, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Avanesov, M.; Wiese, N.J.; Karul, M.; Guerreiro, H.; Keller, S.; Busch, P.; Jacobsen, F.; Adam, G.; Yamamura, J. Diagnostic prediction of complicated appendicitis by combined clinical and radiological appendicitis severity index (APSI). Eur. Radiol. 2018, 28, 3601–3610. [Google Scholar] [CrossRef] [PubMed]
- Kabir, H.D.; Khanam, S.; Khozeimeh, F.; Khosravi, A.; Mondal, S.K.; Nahavandi, S.; Acharya, U.R. Aleatory-aware deep uncertainty quantification for transfer learning. Comput. Biol. Med. 2022, 143, 105246. [Google Scholar] [CrossRef]
- Gosain, A.; Williams, R.F.; Blakely, M.L. Distinguishing acute from ruptured appendicitis preoperatively in the pediatric patient. Adv. Surg. 2010, 44, 73–85. [Google Scholar] [CrossRef]
- Ashcraft, K.W.; Holcomb, G.; Murphy, J.P.; Ostlie, D.J. Pediatric Surgery; Saunders/Elsevier: London, UK, 2014. [Google Scholar]
- Brunicardi, F.C.; Andersen, A.; Billiar, T.R.; Dunn, D.L.; Hunter, J.G. Schwartz’s Principles of Surgery; McGraw-Hill Education: New York, NY, USA, 2014. [Google Scholar]
- Peña, B.M.; Taylor, G.A.; Lund, D.P.; Mandl, K.D. Effect of computed tomography on patient management and costs in children with suspected appendicitis. Pediatrics 1999, 104, 440–446. [Google Scholar] [CrossRef]
- Fraser, J.D.; Aguayo, P.; Sharp, S.W.; Snyder, C.L.; Rivard, D.C.; Cully, B.E.; Sharp, R.J.; Ostlie, D.J.; St Peter, S.D. Accuracy of computed tomography in predicting appendiceal perforation. J. Pediatr. Surg. 2010, 45, 231–234; discussion 234–234. [Google Scholar] [CrossRef]
- Baldisserotto, M.; Marchiori, E. Accuracy of noncompressive sonography of children with appendicitis according to the potential positions of the appendix. AJR Am. J. Roentgenol. 2000, 175, 1387–1392. [Google Scholar] [CrossRef] [Green Version]
- Benjaminov, O.; Atri, M.; Hamilton, P.; Rappaport, D. Frequency of visualization and thickness of normal appendix at nonenhanced helical CT. Radiology 2002, 225, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Espejo, O.d.J.A.; Mejía, M.E.M.; Guerrero, L.H.U. Acute appendicitis: Imaging findings and current approach to diagnostic images. Rev. Colomb. Radiol. 2014, 25, 3877–3888. [Google Scholar]
- Katipoglu, B.; Aygun, A.; Çınar, H. The effect of appendix diameter on perforation in acute appendicitis cases. Cumhur. Med. J. 2019, 41, 392–397. [Google Scholar] [CrossRef]
- Yildirim, O.; Solak, C.; Koçer, B.; Unal, B.; Karabeyoğlu, M.; Bozkurt, B.; Aksaray, S.; Cengiz, O. The role of serum inflammatory markers in acute appendicitis and their success in preventing negative laparotomy. J. Investig. Surg. 2006, 19, 345–352. [Google Scholar] [CrossRef]
- Gökçe, A.H.; Aren, A.; Gökçe, F.S.; Dursun, N.; Barut, A.Y. Reliability of ultrasonography for diagnosing acute appendicitis. Ulus Travma Acil Cerrahi Derg 2011, 17, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Binnebösel, M.; Otto, J.; Stumpf, M.; Mahnken, A.H.; Gassler, N.; Schumpelick, V.; Truong, S. Acute appendicitis. Modern diagnostics--surgical ultrasound. Chirurg 2009, 80, 579–587. [Google Scholar] [CrossRef]
- Azok, J.T.; Kim, D.H.; Munoz Del Rio, A.; Sonavane, S.K.; Bhalla, S.; Anaya-Baez, V.; Menias, C.O. Intraluminal air within an obstructed appendix: A CT sign of perforated or necrotic appendicitis. Acad. Radiol. 2012, 19, 1175–1180. [Google Scholar] [CrossRef]
- Hong, H.S.; Cho, H.S.; Woo, J.Y.; Lee, Y.; Yang, I.; Hwang, J.Y.; Kim, H.M.; Kim, J.W. Intra-Appendiceal Air at CT: Is It a Useful or a Confusing Sign for the Diagnosis of Acute Appendicitis? Korean J. Radiol. 2016, 17, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Sano, K.; Ogasahara, K. Receiver-operating characteristic analysis of leukocyte counts and serum C-reactive protein levels in children with advanced appendicitis. Surg. Today 2006, 36, 515–518. [Google Scholar] [CrossRef]
- Grönroos, J.M.; Forsström, J.J.; Irjala, K.; Nevalainen, T.J. Phospholipase A2, C-reactive protein, and white blood cell count in the diagnosis of acute appendicitis. Clin. Chem. 1994, 40, 1757–1760. [Google Scholar] [CrossRef]
- Grönroos, J.M.; Grönroos, P. Leucocyte count and C-reactive protein in the diagnosis of acute appendicitis. Br. J. Surg. 1999, 86, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.L.; Kong, M.S.; Lin, S.L.; Lin, T.Y.; Huang, C.S.; Lou, C.C.; Lin, J.N. Diagnostic value of C-reactive protein in children with perforated appendicitis. Eur. J. Pediatr. 1996, 155, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Woo, S.H.; Lee, W.J.; Seol, S.H.; Kim, D.H.; Lee, J.Y.; Choi, S.P. High white blood cell count and erythrocyte sedimentation rate are associated with perforated appendicitis in children. Pediatr. Emerg. Med. J. 2017, 4, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Anand, S.; Krishnan, N.; Birley, J.R.; Tintor, G.; Bajpai, M.; Pogorelić, Z. Hyponatremia—A New Diagnostic Marker for Complicated Acute Appendicitis in Children: A Systematic Review and Meta-Analysis. Children 2022, 9, 1070. [Google Scholar] [CrossRef]
- Maita, S.; Andersson, B.; Svensson, J.F.; Wester, T. Nonoperative treatment for nonperforated appendicitis in children: A systematic review and meta-analysis. Pediatr. Surg. Int. 2020, 36, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Roach, J.P.; Partrick, D.A.; Bruny, J.L.; Allshouse, M.J.; Karrer, F.M.; Ziegler, M.M. Complicated appendicitis in children: A clear role for drainage and delayed appendectomy. Am. J. Surg. 2007, 194, 769–773. [Google Scholar] [CrossRef]




| Characteristic | All (n = 315) | Development Cohort (n = 198) | Test Cohort (n = 117) | p-Value |
|---|---|---|---|---|
| Age(years) † | 12.1 ± 3.8 | 12.1 ± 3.8 | 12.1 ± 4.0 | 0.665 |
| Sex | ||||
| Male | 190 (60.3%) | 124 (62.6%) | 66 (56.4%) | 0.3 |
| Female | 125 (39.7%) | 74 (37.4%) | 51 (43.6%) | |
| CT findings | ||||
| Periappendiceal abscess | 6 (1.9%) | 3 (1.5%) | 3 (2.6%) | 0.67 |
| Periappendiceal inflammatory mass | 21 (6.7%) | 14 (7.1%) | 7 (6.0%) | 0.71 |
| Free air | 7 (2.2%) | 5 (2.5%) | 2 (1.7%) | 1.00 |
| Intraluminal appendiceal air | 82 (26.0%) | 55 (27.8%) | 27 (23.1%) | 0.36 |
| Appendicolith | 135 (42.9%) | 85 (42.9%) | 50 (42.7%) | 1.00 |
| Suspicious wall defect | 63 (20.0%) | 48 (24.2%) | 15 (12.8%) | 0.02 |
| Transverse diameter of appendix (mm) † | 100.6 ± 31.1 | 98.3 ± 30.4 | 102.5 ± 31.9 | 0.89 |
| Periappendiceal fluid collection | 71 (22.5%) | 49 (24.7%) | 22 (18.8%) | 0.22 |
| ascites | 185 (58.7%) | 128 (64.6%) | 57 (48.7%) | 0.01 |
| Periappendiceal infiltration | 240 (76.2%) | 158 (79.8%) | 82 (70.1%) | 0.05 |
| Laboratory results | ||||
| CRP (mg/L) † | 19.5 ± 35.8 | 20.7 ± 38.9 | 18.4 ± 32.2 | 0.07 |
| WBC (103/uL) † | 3.2 ± 4.8 | 13.3 ± 4.6 | 13.2 ± 4.7 | 0.77 |
| Neutrophil count (/uL) † | 10,591.7 ± 4682.2 | 10,612.0 ± 4543.8 | 10,804.5 ± 4412.9 | <0.01 |
| ESR (mm/hr) † | 15.10 ± 14.400 | 14.3 ± 14.6 | 16.0 ± 13.3 | 0.27 |
| Clinical Symptom and sign | ||||
| RLQ pain | 142 (45.1%) | 81 (40.9%) | 61 (52.1%) | 0.05 |
| Nausea | 130 (41.3%) | 88 (44.4%) | 42 (35.9%) | 0.14 |
| Vomiting | 146 (46.3%) | 94 (47.5%) | 52 (44.4%) | 0.60 |
| RLQ(DT) | 265 (84.1%) | 166 (83.8%) | 99 (84.6%) | 0.86 |
| RLQ(RT) | 107 (34.0%) | 73 (36.9%) | 34 (29.1%) | 0.16 |
| Duration (hr) † | 21.5 ± 23.2 | 21.9 ± 24.2 | 17.9 ± 17.9 | 0.759 |
| Temperature(°C) † | 37.1 ± 0.7 | 37.0 ± 0.7 | 37.2 ± 0.8 | 0.955 |
| Pathologic results | ||||
| Noncomplicated appendicitis | 138 (43.8%) | 98 (49.5%) | 40 (34.2%) | 0.01 |
| Complicated appendicitis | 177 (56.2%) | 100 (50.5%) | 77 (65.8%) |
| Noncomplicated Appendicitis (n = 98) | Complicated Appendicitis (n = 100) | p-Value | |
|---|---|---|---|
| Age (years) | 12.1 ± 3.6 | 12.1 ± 3.9 | 0.94 |
| Sex | |||
| Male | 68 (69.4%) | 56 (56.0%) | 0.05 |
| Female | 30 (30.6%) | 44 (44.0%) | |
| CT findings | |||
| Periappendiceal abscess | 0 (0.0%) | 3 (3.0%) | 0.25 |
| Periappendiceal inflammatory mass | 0 (0.0%) | 14 (14.0%) | <0.001 |
| Free air | 0 (0.0%) | 5 (5.0%) | 0.06 |
| Intraluminal appendiceal air | 38 (38.8%) | 17 (17.0%) | <0.001 |
| Appendicolith | 24 (24.5%) | 61 (61.0%) | <0.001 |
| Suspicious wall defect | 5 (5.1%) | 43 (43.0%) | <0.001 |
| Transverse diameter of appendix (mm) | 83.0 ± 22.8 | 117.1 ± 28.5 | <0.001 |
| Periappendiceal fluid collection | 8 (8.2%) | 41(41.0%) | <0.001 |
| Ascites | 46 (46.9%) | 82 (82.0%) | <0.001 |
| Periappendiceal infiltration | 62 (63.3%) | 96 (96.0%) | <0.001 |
| Laboratory results | |||
| CRP (mg/L) † | 11.7 ± 15.0 | 29.7 ± 51.3 | 0.12 |
| WBC (103/uL) † | 11.2 ± 4.4 | 15.4 ± 4.4 | <0.001 |
| Neutrophil count † (/uL) | 8516.7 ± 4223.4 | 12,757.4 ± 4397.9 | <0.001 |
| ESR (mm/hr) † | 12.51 ± 13.799 | 16.74 ± 15.952 | 0.06 |
| Clinical Symptom and sign | |||
| RLQ pain | 40 (40.8%) | 41 (41.0%) | 0.98 |
| Nausea | 47 (48.0%) | 41 (41.0%) | 0.32 |
| Vomiting | 48 (49.0%) | 46 (46.0%) | 0.67 |
| RLQ(DT) | 84 (85.7%) | 82 (82.0%) | 0.48 |
| RLQ(RT) | 34 (34.7%) | 39 (39.0%) | 0.53 |
| Duration (hr) † | 23.7 ± 26.7 | 22.8 ± 24.8 | 0.79 |
| Temperature (°C) † | 37.0 ± 0.7 | 37.0 ± 0.7 | 0.97 |
| Development Group | Test Group | |||||
|---|---|---|---|---|---|---|
| Pathology Results | Complicated Appendicitis | Noncomplicated Appendicitis | Complicated Appendicitis | Noncomplicated Appendicitis | ||
| Model prediction | Complicated appendicitis | 90 | 10 | 55 | 22 | |
| Noncomplicated appendicitis | 8 | 90 | 9 | 31 | ||
| AUC | 0.91 (0.86, 0.95) | 0.74 (0.63, 0.84) | ||||
| Sensitivity (%) | 91.8 (84.5, 96.4) | 85.9 (75.0, 93.4) | ||||
| Specificity (%) | 90.0 (82.4, 95.1) | 58.5 (44.1, 71.9) | ||||
| Accuracy (%) | 90.9 (86.0, 94.5) | 73.5 (64.2, 81.2) | ||||
| PPV (%) | 90 (83.3, 94.2) | 71.4 (64.2, 77.8) | ||||
| NPV (%) | 91.8 (85.2, 95.6) | 77.5 (64.3, 86.8) | ||||
| PLR | 9.2 (5.1, 16.6) | 2.1 (1.5, 2.9) | ||||
| NLR | 0.1 (0.1, 0.2) | 0.2 (0.1, 0.5) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, J.; Park, S.; Hwang, S.M. Diagnostic Algorithm Based on Machine Learning to Predict Complicated Appendicitis in Children Using CT, Laboratory, and Clinical Features. Diagnostics 2023, 13, 923. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13050923
Byun J, Park S, Hwang SM. Diagnostic Algorithm Based on Machine Learning to Predict Complicated Appendicitis in Children Using CT, Laboratory, and Clinical Features. Diagnostics. 2023; 13(5):923. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13050923
Chicago/Turabian StyleByun, Jieun, Seongkeun Park, and Sook Min Hwang. 2023. "Diagnostic Algorithm Based on Machine Learning to Predict Complicated Appendicitis in Children Using CT, Laboratory, and Clinical Features" Diagnostics 13, no. 5: 923. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13050923