Retrospective Side Effect Profiling of the Metastatic Melanoma Combination Therapy Ipilimumab-Nivolumab Using Adverse Event Data

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Adverse Event Data Set
2.2. FAERS Data Integration
- Drugs were further categorized according to the Anatomical Therapeutic Chemical (ATC) classification system.
- Indications and reactions (coded by FAERS in terms from the MedDRA dictionary) were contextualized further by using the full hierarchical structure of the ontology.
2.3. Statistical Characterization of the Adverse Event Data
| AE cases | Event (E) | Not E | Totals |
| Drug (D) | a | B | a + b |
| Not D | c | D | c + d |
| Totals | a + c | b + d | N = a + b + c + d |
2.4. Experiments: Definition of Cohorts
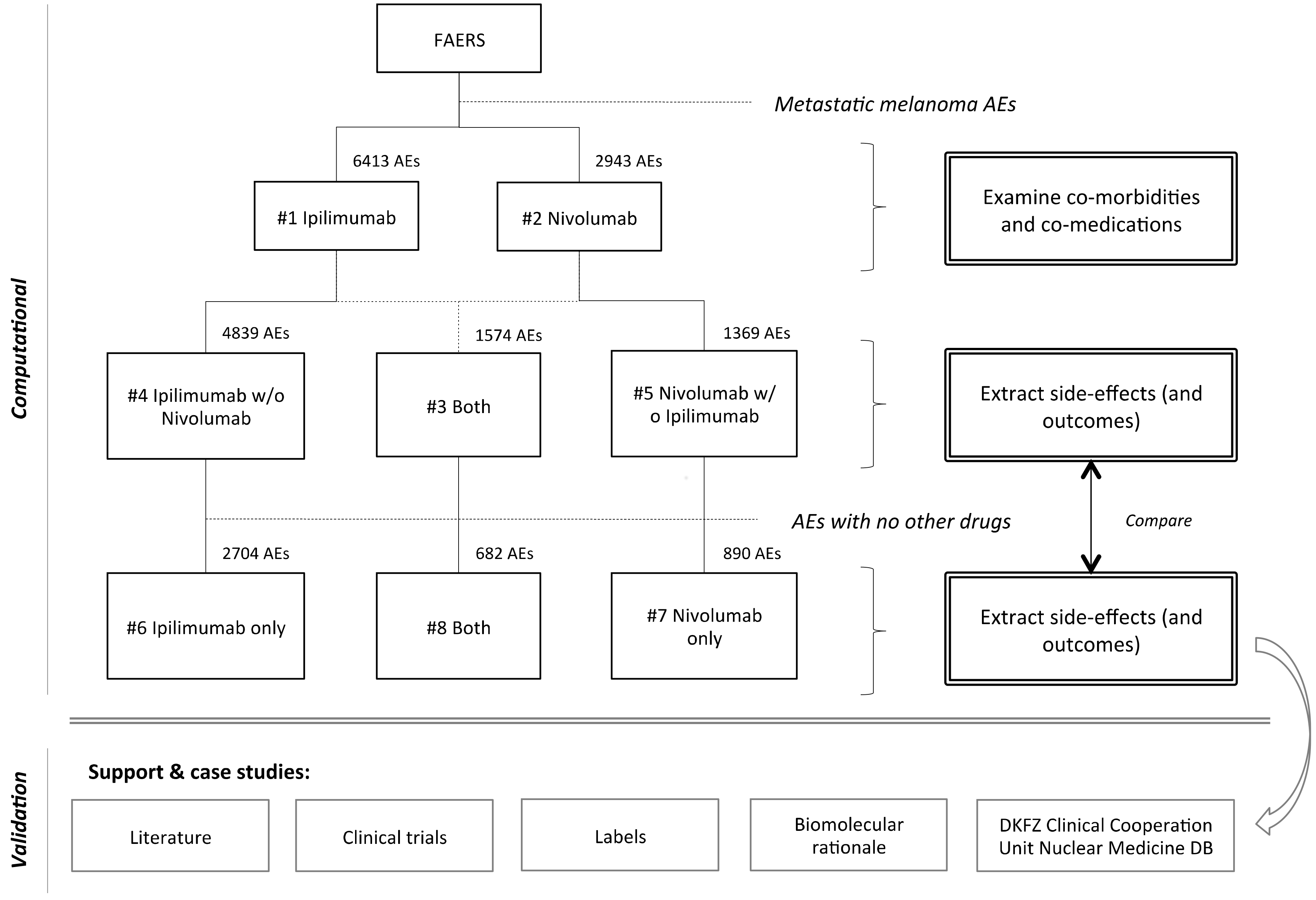
- #1) Ipilimumab: cases that had ipilimumab reported as medication. This set of 6413 AEs was used to profile co-morbidities and co-medications of ipilimumab, as reported in FAERS.
- #2) Nivolumab: cases that had nivolumab reported as medication. This set of 2943 AEs was used to profile co-morbidities and co-medications of Nivolumab, as reported in FAERS.
- #3) Ipilimumab and Nivolumab (together): cases that had both ipilimumab and nivolumab reported as medications. This set of 1574 AEs was used to cross-validate the combination’s side-effect profile when used together with other drugs.
- #4) Ipilimumab without Nivolumab: cases that had ipilimumab reported as medication but not nivolumab. This set of 4839 AEs was used to cross-validate the ipilimumab side-effect profile when used together with other drugs, but not with Nivolumab.
- #5) Nivolumab without Ipilimumab: cases that had nivolumab reported as medication but not ipilimumab. This set of 1369 AEs was used to cross-validate the nivolumab side-effect profile when used together with other drugs, but not with ipilimumab.
- #6) Ipilimumab (only): cases that had only ipilimumab reported as medication, and no other drugs. This set of 2704 AEs was used to identify the ipilimumab side-effects.
- #7) Nivolumab (only): cases that had only nivolumab reported as medication, and no other drugs. This set of 890 AEs was used to identify the nivolumab side-effects.
- #8) Ipilimumab and Nivolumab (only): cases that had both ipilimumab and nivolumab reported as medications, and no other drugs. This set of 682 AEs was used to identify the combination’s side-effect profile.
2.5. Analysis of Outcomes
| Cohort’s AEs | Outcome (O) | Not O | Totals |
| Reaction (R) | A | b | a + b |
| Not R | C | d | c + d |
| Totals | a + c | b + d | N = a + b + c + d |
2.6. Patient Case Examples
3. Results
3.1. Side Effect Profiling
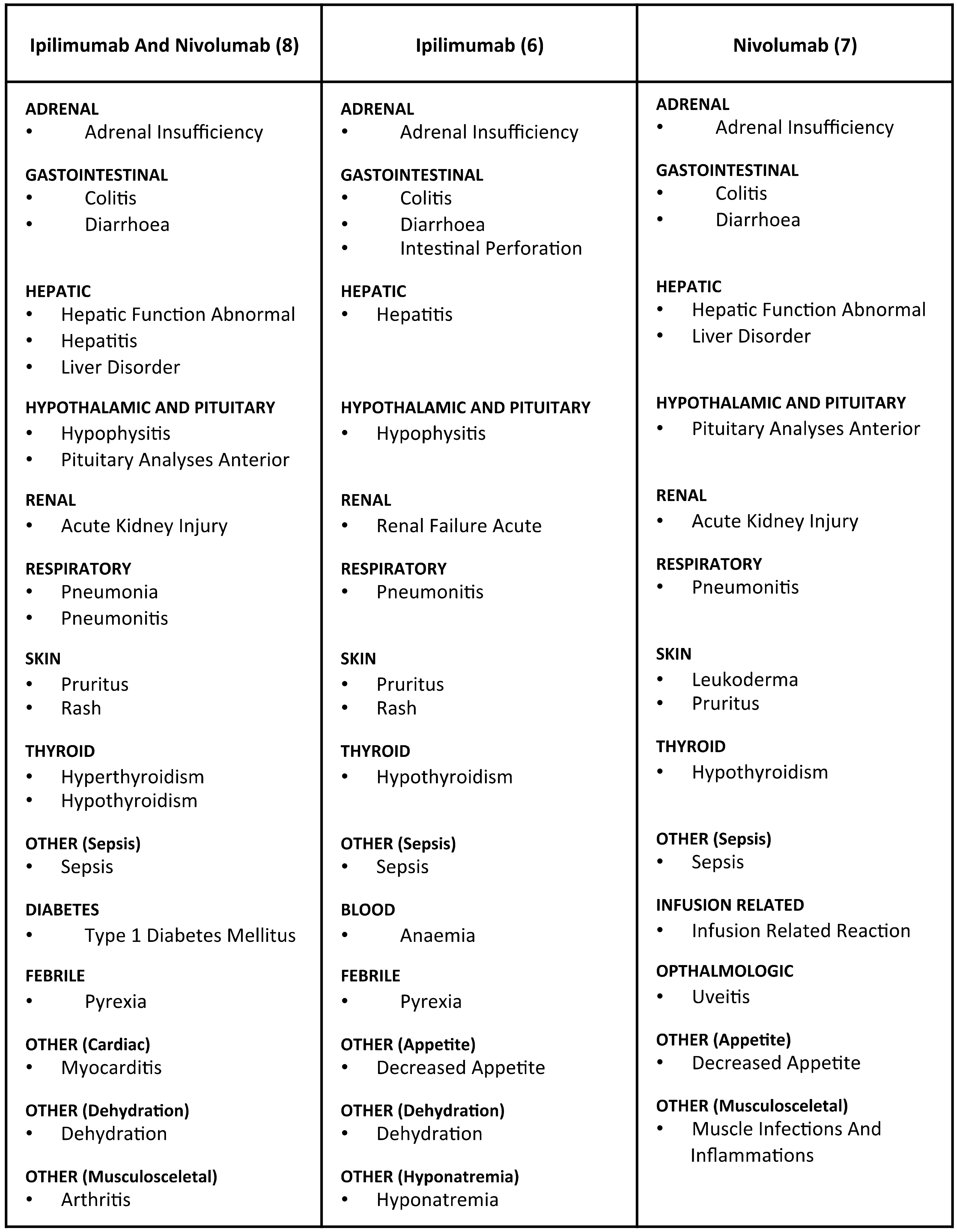
- #6: Ipilimumab (only): diarrhoea (14.35%); colitis (11.06%); rash (6.51%); hypophysitis (4.62%); pyrexia (3.96%); pruritus (2.92%); dehydration (2.89%); decreased appetite (2.74%); anaemia (1.70%); adrenal insufficiency (1.55%); sepsis (1.41%); hepatitis (1.33%); intestinal perforation (1.29%); hyponatraemia (1.29%); hypothyroidism (1.26%); pneumonitis (1.22%); renal failure acute (1.11%).
- #7: Nivolumab (only): hypothyroidism (4.72%); diarrhoea (4.27%); pruritus (3.26%); decreased appetite (2.36%); colitis (2.02%); pneumonitis (1.79%); hepatic function abnormal (1.69%); leukoderma (1.69%); pituitary analyses anterior (1.35%); muscle infections and inflammations (1.35%); sepsis (1.24%); acute kidney injury (1.24%); infusion related reaction (1.12%); uveitis (1.12%); adrenal insufficiency (1.01%); liver disorder (1.01%).
- #8: Ipilimumab and Nivolumab (only): diarrhoea (9.82%); colitis (9.53%); pyrexia (7.04%); rash (5.57%); hypophysitis (3.52%); pneumonitis (3.08%); hyperthyroidism (2.93%); hypothyroidism (2.93%); pruritus (2.79%); hepatitis (2.64%); pneumonia (2.64%); dehydration (2.05%) type 1 diabetes mellitus (1.61%); liver disorder (1.61%); myocarditis (1.61%); sepsis (1.61%); adrenal insufficiency (1.47%); acute kidney injury (1.47%); pituitary analyses anterior (1.32%); arthritis (1.32%); hepatic function abnormal (1.17%).
3.2. Outcome Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hodi, F.S.; O’day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.S.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.T.; Berman, D.M.; Wolchok, J.D. Pooled Analysis of Long-Term Survival Data from Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller, W.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients with Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet 2017, 390, 1853–1862. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-N.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Warner, A.B.; Postow, M.A. Combination Controversies: Checkpoint Inhibition Alone or in Combination for the Treatment of Melanoma? Oncology 2018, 32, 228–234. [Google Scholar] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S.; Feunang, Y.D.; Guo, A.C.; Lo, E.J.; Marcu, A.; Grant, J.R.; Sajed, T.; Johnson, D.; Li, C.; Sayeeda, Z.; et al. DrugBank 5.0: A major update to the DrugBank database for 2018. Nucleic Acids Res. 2018, 46, D1074–D1082. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Thiessen, P.A.; Bolton, E.E.; Chen, J.; Fu, G.; Gindulyte, A.; Han, L.; He, J.; He, S.; Shoemaker, B.A.; et al. PubChem Substance and Compound databases. Nucleic Acids Res. 2016, 44, D1202–D1213. [Google Scholar] [CrossRef] [PubMed]
- Van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, T.G.; O’Donoghue, S.I.; Satagopam, V.P.; Jensen, L.J.; Brown, N.P.; Barbosa-Silva, A.; Schneider, R. Martini: Using literature keywords to compare gene sets. Nucleic Acids Res. 2010, 38, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, T.G.; Perdigão, N.; Brown, N.P.; Sabir, K.S.; O’Donoghue, S.I. How to learn about gene function: Text-mining or ontologies? Methods 2015, 74, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; López-Martin, J.A.; Bendell, J.; Ott, P.A.; Taylor, M.; Eder, J.P.; Jäger, D.; Pietanza, C.; Le, D.T.; Braud, F.; et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): A multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016, 17, 883–895. [Google Scholar] [CrossRef]
- Attia, P.; Phan, G.Q.; Maker, A.V.; Robinson, M.R.; Quezado, M.M.; Yang, J.C.; Sherry, R.M.; Topalian, S.L.; Kammula, U.S.; Royal, R.E.; et al. Autoimmunity correlates with tumor regression in patients with metastatic melanoma treated with anti-cytotoxic T-lymphocyte antigen-4. J. Clin. Oncol. 2005, 23, 6043–6053. [Google Scholar] [CrossRef] [PubMed]
- Downey, S.G.; Klapper, J.A.; Smith, F.O.; Yang, J.C.; Sherry, R.M.; Royal, R.E.; Kammula, U.S.; Hughes, M.S.; Allen, T.E.; Levy, C.L.; et al. Prognostic factors related to clinical response in patients with metastatic melanoma treated by CTL-associated antigen-4 blockade. Clin. Cancer Res. 2007, 13, 6681–6688. [Google Scholar] [CrossRef] [PubMed]
- Assi, H.; Wilson, K.S. Immune toxicities and long remission duration after ipilimumab therapy for metastatic melanoma: Two illustrative cases. Curr. Oncol. 2013, 20, e165–e169. [Google Scholar] [CrossRef] [PubMed]
- Horvat, T.Z.; Adel, N.G.; Dang, T.O.; Momtaz, P.; Postow, M.A.; Callahan, M.K.; Carvajal, R.D.; Dickson, M.A.; D’Angelo, S.P.; Woo, K.M.; et al. Immune-Related Adverse Events, Need for Systemic Immunosuppression, and Effects on Survival and Time to Treatment Failure in Patients with Melanoma Treated with Ipilimumab at Memorial Sloan Kettering Cancer Center. J. Clin. Oncol. 2015, 33, 3193–3198. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; Di Dalmazi, G.; Lombardi, M.; Grosso, F.; Larman, H.B.; Larman, T.; Taverna, G.; Cosottini, M.; Lupi, I. Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series. Am. J. Pathol. 2016, 186, 3225–3235. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, E.H.; Fisher, D.E. Immune and molecular correlates in melanoma treated with immune checkpoint blockade. Cancer 2017, 123, 2143–2153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassel, J.C.; Heinzerling, L.; Aberle, J.; Bähr, O.; Eigentler, T.K.; Grimm, M.O.; Grünwald, V.; Leipe, J.; Reinmuth, N.; Tietze, J.K.; et al. Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): Evaluation and management of adverse drug reactions. Cancer Treat. Rev. 2017, 57, 36–49. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | Ipilimumab and Nivolumab (#8) | Ipilimumab (#6) | Nivolumab (#7) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Order | Name | AEs | % | Name | AEs | % | Name | AEs | % |
| 1 | Diarrhoea | 67 | 9.9 | Diarrhoea | 388 | 14.3 | Hypothyroidism | 42 | 4.7 |
| 2 | Colitis | 65 | 9.5 | Colitis | 299 | 11.1 | Diarrhoea | 38 | 4.3 |
| 3 | Pyrexia | 48 | 7.0 | Rash | 176 | 6.5 | Pruritus | 29 | 3.3 |
| 4 | Rash | 38 | 5.6 | Fatigue | 139 | 5.1 | Alanine aminotransferase increased | 21 | 2.4 |
| 5 | Hypophysitis | 24 | 3.5 | Hypophysitis | 125 | 4.6 | Decreased appetite | 21 | 2.4 |
| 6 | Pneumonitis | 21 | 3.1 | Pyrexia | 107 | 3.9 | Aspartate aminotransferase increased | 20 | 2.2 |
| 7 | Hyperthyroidism | 20 | 2.9 | Vomiting | 99 | 3.7 | Colitis | 18 | 2.0 |
| 8 | Hypothyroidism | 20 | 2.9 | Pruritus | 79 | 2.9 | Gamma-glutamyltransferase increased | 17 | 1.9 |
| 9 | Pruritus | 19 | 2.8 | Dehydration | 78 | 2.9 | Pneumonitis | 16 | 1.8 |
| 10 | Hepatitis | 18 | 2.6 | Decreased appetite | 74 | 2.7 | Hepatic function abnormal | 15 | 1.7 |
| 11 | Pneumonia | 18 | 2.6 | Abdominal pain | 67 | 2.5 | Interstitial lung disease | 15 | 1.7 |
| 12 | General physical health deterioration | 17 | 2.5 | Enterocolitis | 56 | 2.1 | Leukoderma | 15 | 1.7 |
| 13 | Abdominal pain | 16 | 2.3 | Weight decreased | 53 | 2.0 | Blood alkaline phosphatase increased | 14 | 1.6 |
| 14 | Alanine aminotransferase increased | 14 | 2.1 | Anaemia | 46 | 1.7 | Acute kidney injury | 11 | 1.2 |
| 15 | Dehydration | 14 | 2.1 | Adrenal insufficiency | 42 | 1.6 | Lung disorder | 11 | 1.2 |
| 16 | Aspartate aminotransferase increased | 11 | 1.6 | Sepsis | 38 | 1.4 | Sepsis | 11 | 1.2 |
| 17 | Liver disorder (not further clarified) | 11 | 1.6 | Hepatitis | 36 | 1.3 | Infusion related reaction | 10 | 1.1 |
| 18 | Myocarditis | 11 | 1.6 | Hyponatraemia | 35 | 1.3 | Renal impairment | 10 | 1.1 |
| 19 | Sepsis | 11 | 1.6 | Intestinal perforation | 35 | 1.3 | Uveitis | 10 | 1.1 |
| 20 | Type 1 diabetes mellitus | 11 | 1.6 | Hypothyroidism | 34 | 1.3 | Adrenal insufficiency|liver disorder|diabetic ketoacidosis | 9 | 1.0 |
| Total | 591 reactions | 682 | - | 1130 reactions | 2704 | - | 675 reactions | 890 | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soldatos, T.G.; Dimitrakopoulou-Strauss, A.; Larribere, L.; Hassel, J.C.; Sachpekidis, C. Retrospective Side Effect Profiling of the Metastatic Melanoma Combination Therapy Ipilimumab-Nivolumab Using Adverse Event Data. Diagnostics 2018, 8, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics8040076
Soldatos TG, Dimitrakopoulou-Strauss A, Larribere L, Hassel JC, Sachpekidis C. Retrospective Side Effect Profiling of the Metastatic Melanoma Combination Therapy Ipilimumab-Nivolumab Using Adverse Event Data. Diagnostics. 2018; 8(4):76. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics8040076
Chicago/Turabian StyleSoldatos, Theodoros G., Antonia Dimitrakopoulou-Strauss, Lionel Larribere, Jessica C. Hassel, and Christos Sachpekidis. 2018. "Retrospective Side Effect Profiling of the Metastatic Melanoma Combination Therapy Ipilimumab-Nivolumab Using Adverse Event Data" Diagnostics 8, no. 4: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics8040076