Plasma Disappearance Rate of Indocyanine Green for Determination of Liver Function in Three Different Models of Shock

Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Surgical Procedures
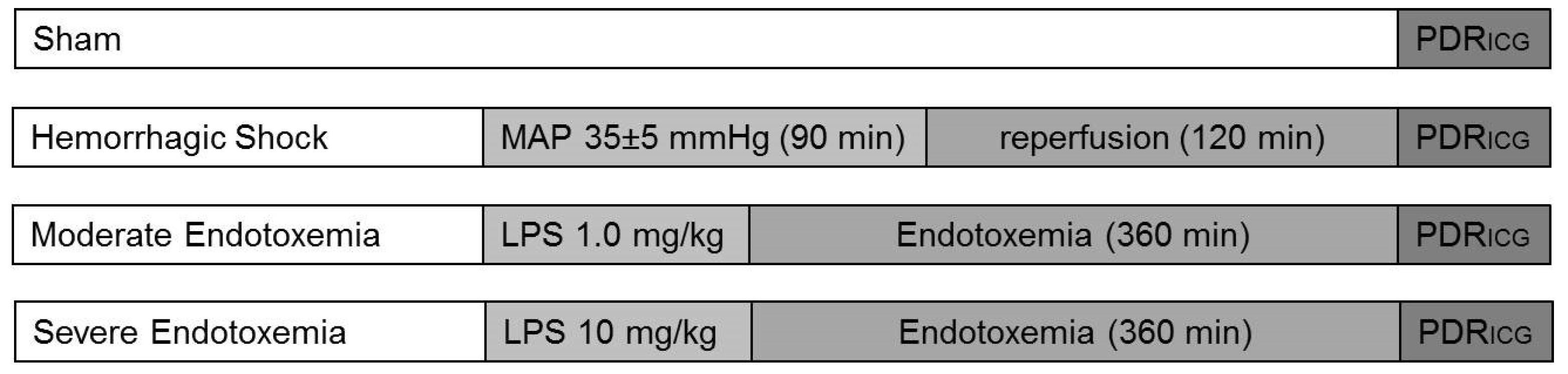
2.3. Experimental Protocol
2.4. Evaluation of PDRICG
2.5. Calculation of ICG Blood Clearance and Compartment Models
2.6. Statistical Analysis
3. Results
3.1. Hemodynamics and Blood Gas Analysis
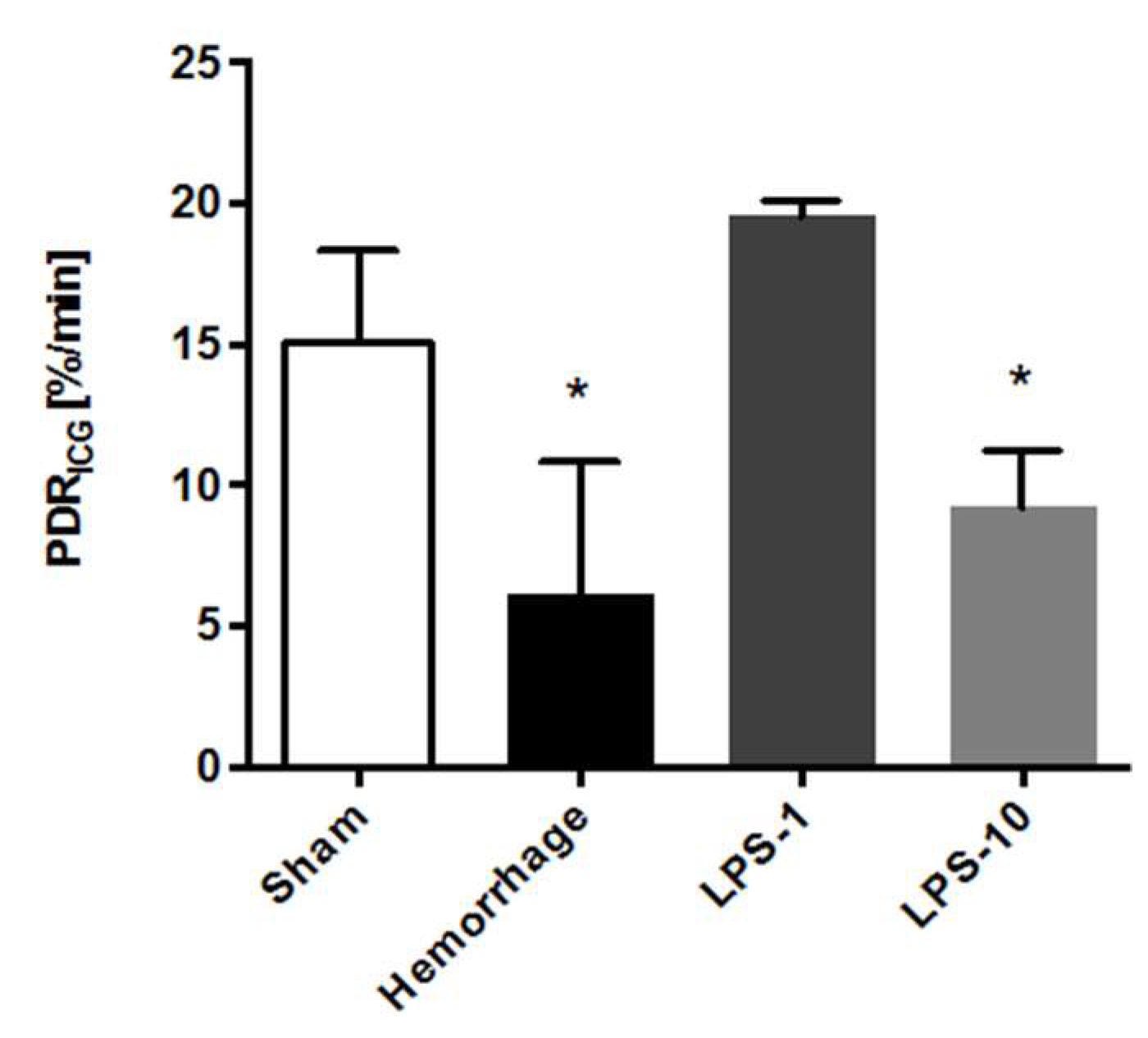
3.2. Plasma Disappearance Rate of Indocyanine Green
3.3. Calculation of 1-Compartment Models
3.4. Calculation of 2-Compartment Models
3.5. Calculation of 3-Compartment Models
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Kortgen, A.; Recknagel, P.; Bauer, M. How to assess liver function? Curr. Opin. Crit. Care 2010, 16, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Sakka, S.G. Assessing liver function. Curr. Opin. Crit. Care 2007, 13, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Sakka, S.G.; van Hout, N. Relation between indocyanine green (ICG) plasma disappearance rate and ICG blood clearance in critically ill patients. Intensive Care Med. 2006, 32, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Scheingraber, S.; Richter, S.; Igna, D.; Flesch, S.; Kopp, B.; Schilling, M.K. Indocyanine green disappearance rate is the most useful marker for liver resection. Hepato-Gastroenterol. 2008, 55, 1394–1399. [Google Scholar]
- de Liguori Carino, N.; O’Reilly, D.A.; Dajani, K.; Ghaneh, P.; Poston, G.J.; Wu, A.V. Perioperative use of the LiMON method of indocyanine green elimination measurement for the prediction and early detection of post-hepatectomy liver failure. Eur. J. Surg. Oncol. 2009, 35, 957–962. [Google Scholar] [CrossRef] [Green Version]
- Schneider, L.; Spiegel, M.; Latanowicz, S.; Weigand, M.A.; Schmidt, J.; Werner, J.; Stremmel, W.; Eisenbach, C. Noninvasive indocyanine green plasma disappearance rate predicts early complications, graft failure or death after liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2011, 10, 362–368. [Google Scholar] [CrossRef]
- Levesque, E.; Saliba, F.; Benhamida, S.; Ichaï, P.; Azoulay, D.; Adam, R.; Castaing, D.; Samuel, D. Plasma disappearance rate of indocyanine green: a tool to evaluate early graft outcome after liver transplantation. Liver Transpl. 2009, 15, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Kortgen, A.; Paxian, M.; Werth, M.; Recknagel, P.; Rauchfuss, F.; Lupp, A.; Krenn, C.G.; Müller, D.; Claus, A.; Reinhart, K.; et al. Prospective assessment of hepatic function and mechanisms of dysfunction in the critically ill. Shock 2009, 32, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Inal, M.T.; Memiş, D.; Kargi, M.; Sut, N. Prognostic value of indocyanine green elimination assessed with LiMON in septic patients. J. Crit. Care 2009, 24, 329–334. [Google Scholar] [CrossRef]
- Halle, B.M.; Poulsen, T.D.; Pedersen, H.P. Indocyanine green plasma disappearance rate as dynamic liver function test in critically ill patients. Acta Anaesthesiol. Scand. 2014, 58, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Trepenaitis, D.; Pundzius, J.; Macas, A. The influence of thoracic epidural anesthesia on liver hemodynamics in patients under general anesthesia. Medicina 2010, 46, 465. [Google Scholar] [CrossRef]
- Cheng, X.P.; Zhao, J.; Chen, Y.; Meng, F.K.; Xu, B.; Yu, H.W.; Meng, Q.H.; Liu, Y.M.; Zhang, S.B.; Meng, S.; et al. Comparison of the ability of the PDD-ICG clearance test, CTP, MELD, and MELD-Na to predict short-term and medium-term mortality in patients with decompensated hepatitis B cirrhosis. Eur J. Gastroenterol. Hepatol. 2016, 28, 444–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stauber, R.E.; Wagner, D.; Stadlbauer, V.; Palma, S.; Gurakuqi, G.; Kniepeiss, D.; Iberer, F.; Smolle, K.H.; Haas, J.; Trauner, M. Evaluation of indocyanine green clearance and model for end-stage liver disease for estimation of short-term prognosis in decompensated cirrhosis. Liver Int. 2009, 29, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Stehr, A.; Ploner, F.; Traeger, K.; Theisen, M.; Zuelke, C.; Radermacher, P.; Matejovic, M. Plasma disappearance of indocyanine green: a marker for excretory liver function? Intensive. Care Med. 2005, 31, 1719–1722. [Google Scholar] [CrossRef] [PubMed]
- Wissler, E.H. Identifying a long standing error in single-bolus determination of the hepatic extraction ratio for indocyanine green. Eur J. Appl. Physiol. 2011, 111, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Grainger, S.L.; Keeling, P.W.; Brown, I.M.; Marigold, J.H.; Thompson, R.P. Clearance and non-invasive determination of the hepatic extraction of indocyanine green in baboons and man. Clin. Sci. (Lond) 1983, 64, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Mathes, A.M.; Kubulus, D.; Pradarutti, S.; Bentley, A.; Weiler, J.; Wolf, B.; Ziegeler, S.; Bauer, I.; Rensing, H. Melatonin pretreatment improves liver function and hepatic perfusion after hemorrhagic shock. Shock 2008, 29, 112–118. [Google Scholar] [CrossRef]
- Mathes, A.M.; Kubulus, D.; Weiler, J.; Bentley, A.; Waibel, L.; Wolf, B.; Bauer, I.; Rensing, H. Melatonin receptors mediate improvements of liver function but not of hepatic perfusion and integrity after hemorrhagic shock in rats. Crit. Care Med. 2008, 36, 24–29. [Google Scholar] [CrossRef]
- Mould, D.R.; Upton, R.N. Basic Concepts in Population Modeling, Simulation, and Model-Based Drug Development—Part 2: Introduction to Pharmacokinetic Modeling Methods. CPT Pharmacometrics Syst. Pharmacol. 2013, 2, e38, Shafer, S.L. Pharmacokinetic and Pharmacodynamic Analysis with NONMEM. Palo Alto, CA, USA.; UCSF, 2008. [Google Scholar] [CrossRef]
- Scott, J.M.D.; Barcroft, J. The blood volume and the total amount of haemoglobin in anaemic rats. Biochem. J. 1924, 18, 1–8. [Google Scholar] [CrossRef]
- Mayr, U.; Fahrenkrog-Petersen, L.; Batres-Baires, G.; Herner, A.; Rasch, S.; Schmid, R.M.; Huber, W.; Lahmer, T. Large-volume paracentesis effects plasma disappearance rate of indo-cyanine green in critically ill patients with decompensated liver cirrhosis and intraabdominal hypertension. Ann. Intensive Care 2018, 8, 78. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline | 90 Min | End of Experiment | |
|---|---|---|---|
| pH | |||
| Sham | 7.37 ± 0.04 | 7.36 ± 0.05 | 7.36 ± 0.08 |
| Hemorrhage | 7.37 ± 0.04 | 7.25 ± 0.07 | 7.34 ± 0.06 |
| Moderate Endotoxemia | 7.36 ± 0.05 | 7.35 ± 0.08 | 7.25 ± 0.07 |
| Severe Endotoxemia | 7.37 ± 0.05 | 7.33 ± 0.09 | 7.19 ± 0.09 |
| Hb [g/dl] | |||
| Sham | 10.7 ± 1.1 | 11.0 ± 1.2 | 10.4 ± 1.4 |
| Hemorrhage | 11.2 ± 1.0 | 6.2 ± 1.5 | 8.8 ± 1.3 |
| Moderate Endotoxemia | 10.8 ± 0.8 | 10.0 ± 1.6 | 9.8 ± 1.5 |
| Severe Endotoxemia | 10.6 ± 1.2 | 10.1 ± 1.2 | 9.9 ± 1.5 |
| BE [mmol/L] | |||
| Sham | 0.1 ± 1.9 | −0.8 ± 3.2 | −0.6 ± 4.0 |
| Hemorrhage | −0.2 ± 2.2 | −10.2 ± 3.9 | −2.0 ± 3.5 |
| Moderate Endotoxemia | 0.3 ± 1.4 | −2.2 ± 1.9 | −9.7 ± 3.8 |
| Severe Endotoxemia | 0.4 ± 1.7 | −3.0 ± 2.1 | −14.2 ± 5.5 |
| Lactate [mmol/L] | |||
| Sham | 1.5 ± 0.5 | 1.5 ± 0.4 | 1.6 ± 0.6 |
| Hemorrhage | 1.7 ± 0.7 | 7.9 ± 1.5 | 1.8 ± 0.6 |
| Moderate Endotoxemia | 1.6 ± 0.6 | 2.4 ± 1.2 | 8.3 ± 0.7 |
| Severe Endotoxemia | 1.7 ± 0.7 | 2.2 ± 1.3 | 9.7 ± 0.6 |
| Sham | Hemorrhage | Moderate Endotoxemia | Severe Endotoxemia | |
|---|---|---|---|---|
| 1-compartment model | ||||
| ICG Distribution Volume (mL) | 60.3 | 41.6 | 32.6 | 42.8 |
| Calculated ICG Clearance (mL/min/m2) | 564.0 | 174.0 | 387.0 | 202.0 |
| 2-compartment model | ||||
| ICG Distribution Volume 1 (mL) | 16.2 | 20.2 | 13.3 | 14.1 |
| Calculated ICG Clearance 1 (mL/min/m2) | 246.0 | 84.0 | 305.0 | 181.0 |
| ICG Distribution Volume 2 (mL) | 289.9 | 85.6 | 93.3 | 25.5 |
| Calculated ICG Clearance 2 (mL/min/m2) | 211.0 | 170.0 | 90.0 | 467.0 |
| Micro-rate constant k10 | 0.15 | 0.04 | 0.22 | 0.12 |
| Micro-rate constant k12 | 0.13 | 0.08 | 0.06 | 0.33 |
| Micro-rate constant k21 | 0.007 | 0.01 | 0.009 | 0.18 |
| 3-compartment model | ||||
| ICG Distribution Volume 1 [mL] | 11.7 | 0.01 | 12.8 | 14.1 |
| Calculated ICG Clearance 1 [mL/min/m2] | 137.0 | 134.0 | 300.0 | 181.0 |
| ICG Distribution Volume 2 [mL] | 4.37 | 3.85 | 7.89 | 10.00 |
| Calculated ICG Clearance 2 [mL/min/m2] | 1132.0 | 94.0 | 421.0 | 182.0 |
| ICG Distribution Volume 2 [mL] | 736.9 | 21.4 | 3.4 | 15.5 |
| Calculated ICG Clearance 2 [mL/min/m2] | 313.0 | 222.0 | 677.0 | 284.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathes, A.; Plata, C.; Rensing, H.; Kreuer, S.; Fink, T.; Raddatz, A. Plasma Disappearance Rate of Indocyanine Green for Determination of Liver Function in Three Different Models of Shock. Diagnostics 2019, 9, 108. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030108
Mathes A, Plata C, Rensing H, Kreuer S, Fink T, Raddatz A. Plasma Disappearance Rate of Indocyanine Green for Determination of Liver Function in Three Different Models of Shock. Diagnostics. 2019; 9(3):108. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030108
Chicago/Turabian StyleMathes, Alexander, Christopher Plata, Hauke Rensing, Sascha Kreuer, Tobias Fink, and Alexander Raddatz. 2019. "Plasma Disappearance Rate of Indocyanine Green for Determination of Liver Function in Three Different Models of Shock" Diagnostics 9, no. 3: 108. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030108