Application of Machine Learning Technique to Distinguish Parkinson’s Disease Dementia and Alzheimer’s Dementia: Predictive Power of Parkinson’s Disease-Related Non-Motor Symptoms and Neuropsychological Profile


Abstract
:1. Introduction
2. Methods and Materials
2.1. Data Source
2.2. Measurement
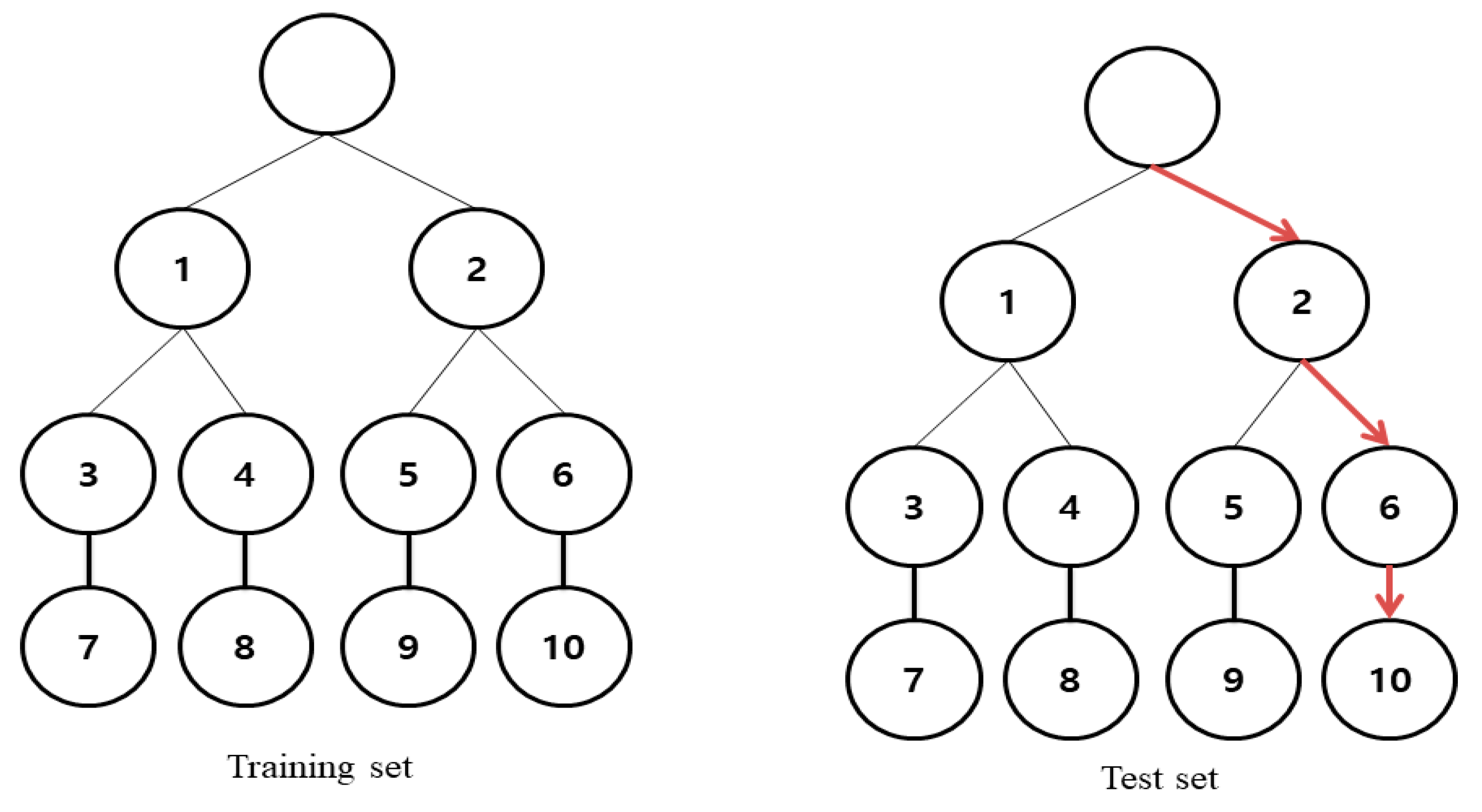
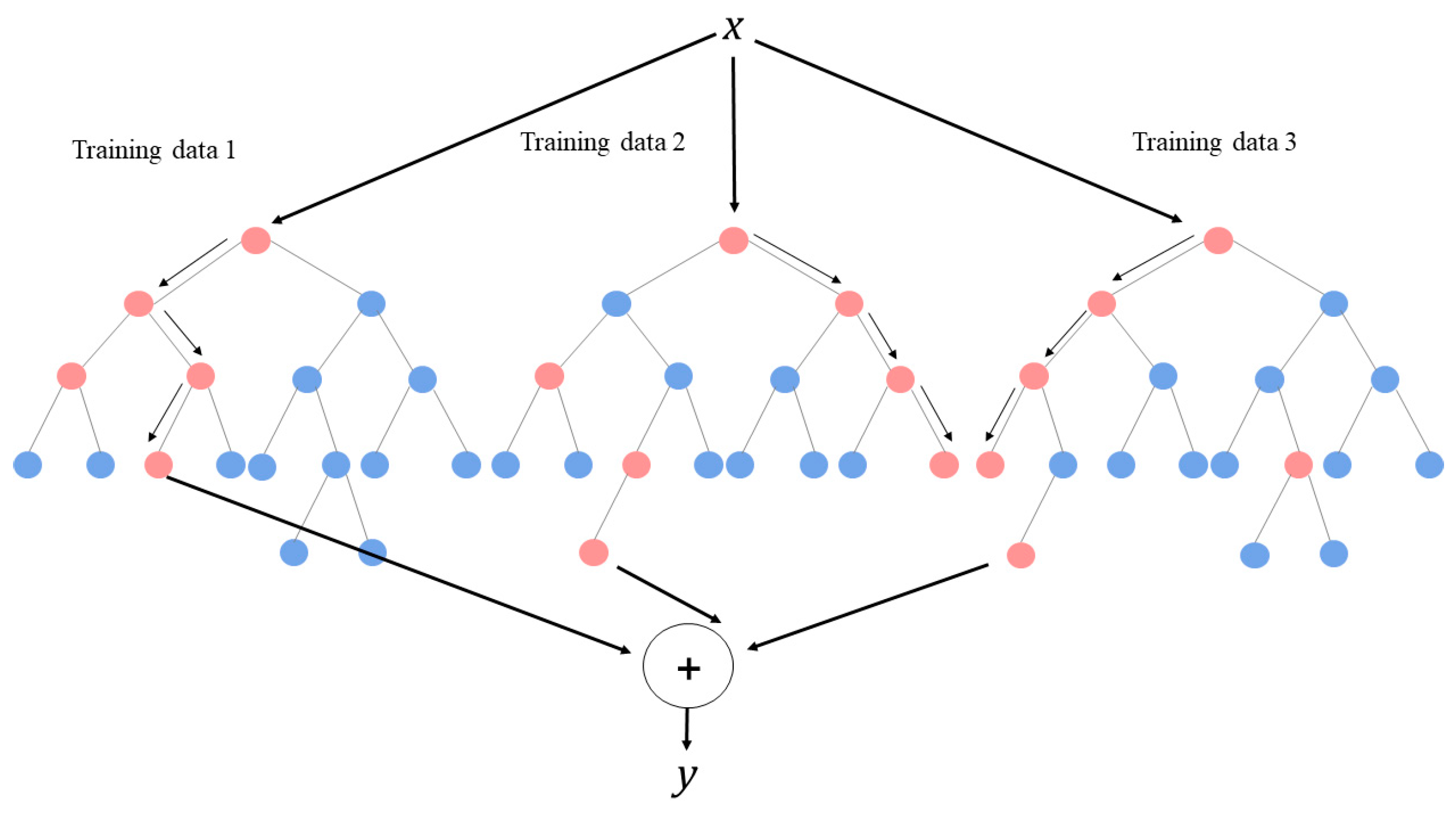
2.3. Development and Evaluation of Random Forest
3. Results
3.1. General Characteristics of Subjects
3.2. Characteristics of Subjects by Dementia Type
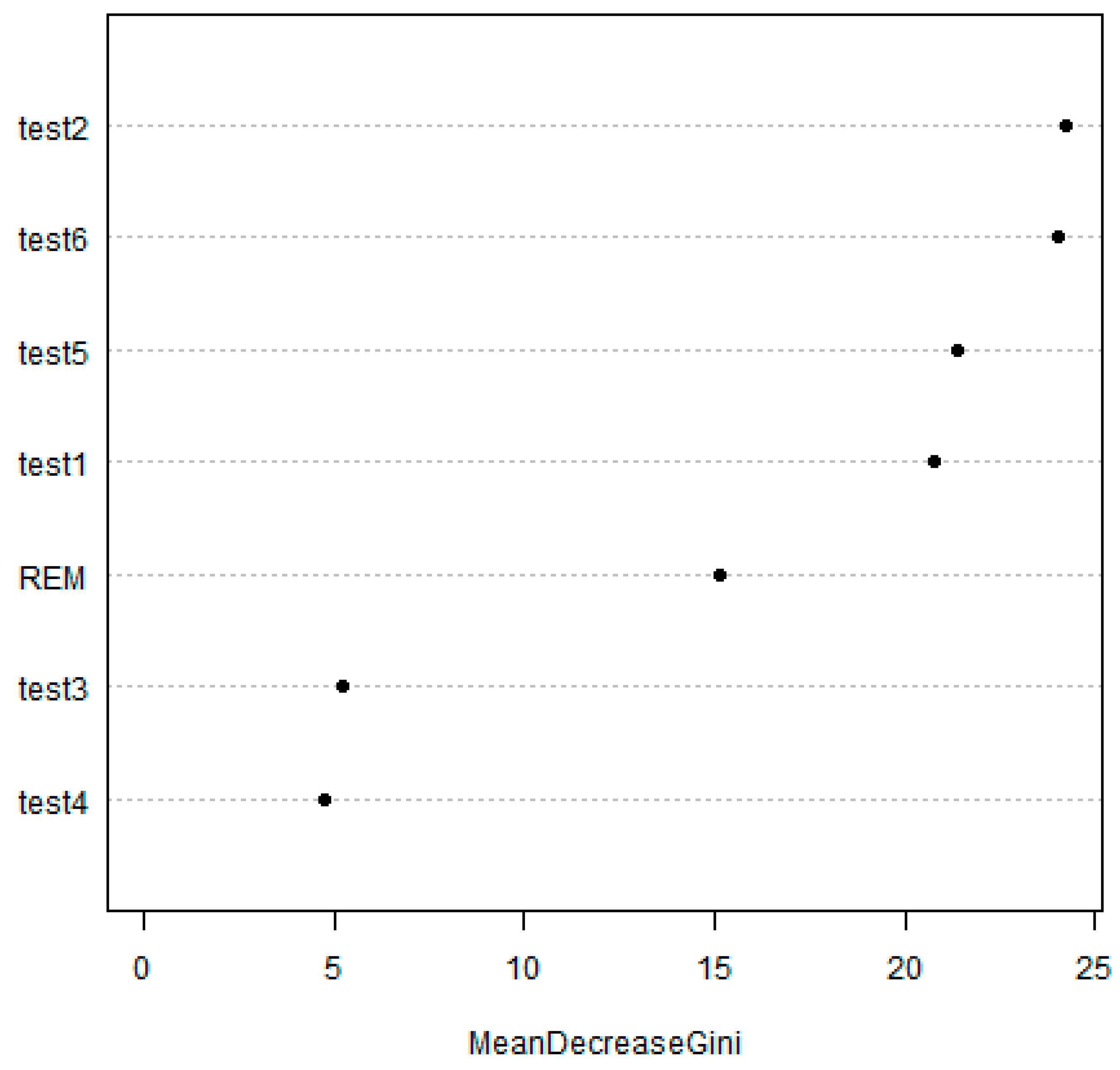
3.3. Diagnostic Predictive Capability Using Random Forest for Distinguishing between AD and PDD
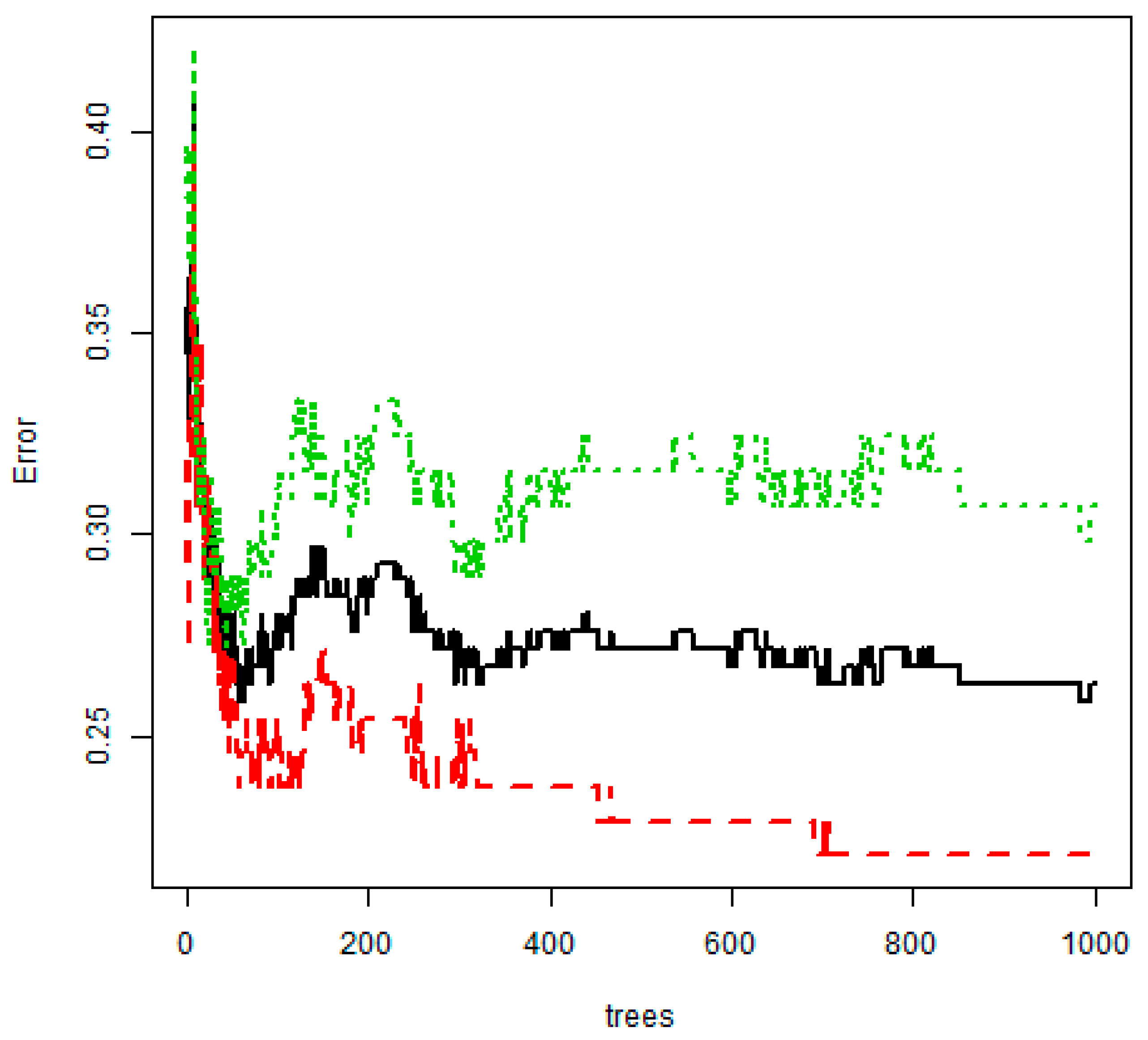
3.4. Performance of the PDD Prediction Model Based on Machine Learning
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Chen, J.H.; Hong, C.T.; Wu, D.; Chi, W.C.; Yen, C.F.; Liao, H.F.; Chan, L.; Liou, T.H. Dementia-Related Functional Disability in Moderate to Advanced Parkinson’s Disease: Assessment Using the World Health Organization Disability Assessment Schedule 2.0. Int. J. Env. Res. Public Health 2019, 16, 2230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Campenhausen, S.; Bornschein, B.; Wick, R.; Botzel, K.; Sampaio, C.; Poewe, W.; Oertel, W.; Siebert, U.; Berger, K.; Dodel, R. Prevalence and incidence of Parkinson’s disease in Europe. Eur. Neuropsychopharmacol. 2005, 15, 473–490. [Google Scholar] [CrossRef] [PubMed]
- Savica, R.; Grossardt, B.R.; Bower, J.H.; Ahlskog, J.E.; Rocca, W.A. Time trends in the iIncidence of Parkinson disease. JAMA Neurol. 2016, 73, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Wang, L.; Liu, S.; Zhu, L.; Loprinzi, P.D.; Fan, X. The Impact of Mind-Body Exercises on Motor Function, Depressive Symptoms, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Int. J. Env. Res. Public Health 2020, 17, e31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, X.; Wang, D.; Hellman, B.; Janssen, M.F.; Bakker, G.; Coghlan, R.; Hursey, A.; Matthews, H.; Whetstone, I. Assessment of Health-Related Quality of Life between People with Parkinson’s Disease and Non-Parkinson’s: Using Data Drawn from the ‘100 for Parkinson’s’ Smartphone-Based Prospective Study. Int. J. Env. Res. Public Health 2018, 15, e2538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarsland, D.; Andersen, K.; Larsen, J.P.; Lolk, A.; Kragh-Sørensen, P. Prevalence and characteristics of dementia in Parkinson disease: an 8-year prospective study. Arch. Neurol. 2003, 60, 387–392. [Google Scholar] [CrossRef] [Green Version]
- Hely, M.A.; Reid, W.G.; Adena, M.A.; Halliday, G.M.; Morris, J.G. The Sydney multicenter study of Parkinson’s disease: the inevitability of dementia at 20 years. Mov. Disord. 2008, 23, 837–844. [Google Scholar] [CrossRef]
- Emre, M. Dementia associated with Parkinson’s disease. Lancet Neurol. 2003, 2, 229–237. [Google Scholar] [CrossRef]
- De Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef]
- McKeith, I.; Mintzer, J.; Aarsland, D.; Burn, D.; Chiu, H.; Cohen-Mansfield, J.; Dickson, D.; Dubois, B.; Duda, J.; Feldman, H.; et al. Dementia with Lewy bodies. Lancet Neurol. 2004, 3, 19–28. [Google Scholar] [CrossRef]
- Nussbaum, M.; Treves, T.A.; Inzelberg, R.; Rabey, J.M.; Korczyn, A.D. Survival in Parkinson’s disease: the effect of dementia. Parkinsonism Relat. Disord. 1998, 4, 179–181. [Google Scholar] [CrossRef]
- Gold, D.A. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2012, 34, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Hu, M.H.; Chen, H.Y.; Li, R.H. Self-reported mobility and instrumental activities of daily living: test-retest reliability and criterion validity. J. Aging. Phys. Act. 2012, 20, 186–197. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Kehagia, A.A.; Barker, R.A.; Robbins, T.W. Neuropsychological and clinical heterogeneity of cognitive impairment and dementia in patients with Parkinson’s disease. Lancet Neurol. 2010, 9, 1200–1213. [Google Scholar] [CrossRef]
- Kudlicka, A.; Clare, L.; Hindle, J.V. Executive functions in Parkinson’s disease: Systematic review and meta-analysis. Mov. Disord. 2011, 26, 2305–2315. [Google Scholar] [CrossRef]
- Taylor, A.E.; Saint, C.; Lang, A.E. Memory and learning in early Parkinson’s disease evidence for a ’frontal lobe syndrome’. Brain Cogn. 1990, 19, 211–232. [Google Scholar] [CrossRef]
- Byeon, H.; Jin, H.; Cho, S. Development of Parkinson’s disease dementia prediction model based on verbal memory, visuospatial memory, and executive function. J. Med. Imaging. Health Inform. 2017, 7, 1517–1521. [Google Scholar]
- Péran, P.; Rascol, O.; Démonet, J.F.; Celsis, P.; Nespoulous, J.L.; Dubois, B.; Cardebat, D. Deficit of verb generation in nondemented patients with Parkinson’s disease. Mov. Disord. 2003, 18, 150–156. [Google Scholar]
- Bherer, L.; Belleville, S.; Hudon, C. Executive function deficits in normal aging, Alzheimer’s disease, and frontotemporal dementia. Psychol. Neuropsychiatr. Vieil. 2004, 2, 181–189. [Google Scholar]
- Song, I.U.; Kim, J.S.; Yoo, J.Y.; Song, H.J.; Lee, K.S. Cognitive dysfunctions in mild Parkinson’s disease dementia: Comparison with patients having mild Alzheimer’s disease and normal controls. Eur. Neurol. 2008, 59, 49–54. [Google Scholar] [CrossRef]
- Mann, D.M.; Jones, D. Deposition ofamyloid (A4) protein within the brains of persons with dementing disorders other than Alzheimer’s disease and Down’s syndrome. Neurosci. Lett. 1990, 109, 68–75. [Google Scholar] [CrossRef]
- Inzelberg, R.; Paleacu, D.; Chapman, J.; Korezyn, A.D. ApolipoproteinE and Parkinson’s disease. Ann. Neurol. 1998, 44, 294. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Burn, D.; Goetz, C.; Aarsland, D.; Brown, R.G.; Broe, G.A.; Dickson, D.; Duyckaerts, C.; Cummings, J.; Gauthier, S.; et al. Diagnostic procedures for Parkinson’s disease dementia: recommendations from the movement disorder society task force. Mov. Disord. 2007, 22, 2314–2324. [Google Scholar] [CrossRef] [PubMed]
- Trout, J.; Christiansen, T.; Bulkley, M.B.; Tanner, J.J.; Sozda, C.N.; Bowers, D.; Kay, D.B. Cognitive Impairments and Self-Reported Sleep in Early-Stage Parkinson’s Disease with Versus without Probable REM Sleep Behavior Disorder. Brain Sci. 2020, 10, e9. [Google Scholar] [CrossRef] [Green Version]
- Aarsland, D.; Tandberg, E.; Larsen, J.P.; Cummings, J.L. Frequency of dementia in Parkinson disease. Arch. Neurol. 1996, 53, 538–542. [Google Scholar] [CrossRef]
- Byeon, H. Predicting the Swallow-Related Quality of Life of the Elderly Living in a Local Community Using Support Vector Machine. Int. J. Env. Res. Public Health 2019, 16, e4269. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. The risk factors of laryngeal pathology in Korean adults using a decision tree model. J. Voice. 2015, 29, 59–64. [Google Scholar] [CrossRef]
- Dauwan, M.; van der Zande, J.J.; van Dellen, E.; Sommer, I.E.; Scheltens, P.; Lemstra, A.W.; Stam, C.J. Random forest to differentiate dementia with Lewy bodies from Alzheimer’s disease. Alzheimers. Dement (Amst). 2016, 4, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. A prediction model for mild cognitive impairment using random forests. IJACSA. 2015, 6, 8–12. [Google Scholar] [CrossRef]
- Lee, J.E.; Kim, J.H.; Hong, E.J.; Yoo, H.S.; Nam, H.Y.; Park, O. National Biobank of Korea: quality control programs of collected-human biospecimens. Osong. Public Health Res. Perspect. 2012, 3, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. Is the Random Forest Algorithm Suitable for Predicting Parkinson’s Disease with Mild Cognitive Impairment out of Parkinson’s Disease with Normal Cognition? Int. J. Env. Res. Public Health 2020, 17, e2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinicopathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry. 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Kang, Y.; Park, J.; Yu, K.H.; Lee, B.C. The validity of the Korean-Montreal Cognitive Assessment (K-MoCA) as a screening test for both MCI and VCI. Conference Abstract: The 20th Annual Rotman Research Institute Conference. Frontal Lobes 2010, 148. [Google Scholar] [CrossRef]
- Cho, M.J.; Bae, J.N.; Suh, G.H.; Hahm, B.J.; Kim, J.K.; Lee, D.W.; Kang, M.H. Validation of geriatric depression scale, Korean version (GDS) in the assessment of DSM-III-R major depression. J. Korean Neuropsychiatr. Assoc. 1999, 38, 48–63. [Google Scholar]
- Choi, S.H.; Na, D.L.; Lee, B.H.; Hahm, D.S.; Jeong, J.H.; Yoon, S.J.; Yoo, K.H.; Ha, C.K.; Han, I.W. Estimating the validity of the Korean version of expanded clinical dementia rating (CDR) scale. J. Korean Neurol. Assoc. 2001, 19, 585–591. [Google Scholar]
- Kang, S.J.; Choi, S.H.; Lee, B.H.; Kwon, J.C.; Na, D.L.; Han, S.H. The reliability and validity of the Korean Instrumental Activities of Daily Living (K-IADL). J. Korean Neurol. Assoc. 2002, 20, 8–14. [Google Scholar]
- Bosboom, J.L.W.; Stoffers, D.; Wolters, E.C. Cognitive dysfunction and dementia in Parkinson’s disease. J. Neural. Transm (Vienna). 2004, 111, 1303–1315. [Google Scholar] [CrossRef]
- Gnanalingham, K.K.; Byrne, E.J.; Thornton, A.; Sambrook, M.A.; Bannister, P. Motor and cognitive function in Lewy body dementia: Comparison with Alzheimer’s and Parkinson’s diseases. J. Neurol. Neurosurg. Psychiatry. 1997, 62, 243–252. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Sabe, L.; Petracca, G.; Chemerinski, E.; Kuzis, G.; Merello, M.; Leiguarda, R. Neuropsychological and psychiatric differences between Alzheimer’s disease and Parkinson’s disease with dementia. J. Neurol. Neurosurg. Psychiatry. 1996, 61, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Larose, D.T.; Larose, C.D. Discovering Knowledge in Data: An Introduction to Data Mining, 2nd ed; John Wiley & Sons: Hoboken, NJ, USA, 2014; pp. 1–309. [Google Scholar]
- Lunetta, K.L.; Hayward, L.B.; Segal, J.; Van Eerdewegh, P. Screening large-scale association study data: Exploiting interactions using random forests. BMC Genet. 2004, 5, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | AD (n = 118) | PDD (n = 110) | p |
|---|---|---|---|
| Age | 0.006 | ||
| 60–74 years old | 46 (42.2) | 63 (57.8) | |
| ≥75 years old | 72 (60.5) | 47 (39.5) | |
| Gender | 0.055 | ||
| Male | 33 (42.9) | 44 (57.1) | |
| Female | 85 (56.3) | 66 (43.7) | |
| Education | 0.638 | ||
| Middle school graduate and below | 88 (52.7) | 79 (47.3) | |
| High school graduate and above | 30 (49.2) | 31 (50.8) | |
| Handless | 0.547 | ||
| Right hand | 114 (51.6) | 107 (48.4) | |
| Left hand | 3 (60.0) | 2 (40.0) | |
| Both hands | 0 | 1 (100) | |
| Family PD history | 0.034 | ||
| No | 74 (48.1) | 80 (51.9) | |
| Yes | 0 | 5 (100) | |
| Family dementia history | 0.081 | ||
| No | 80 (51.6) | 75 (48.4) | |
| Yes | 8 (80.0) | 2 (20.0) | |
| Pack year | 0.441 | ||
| 1−20 | 2 (28.6) | 5 (71.4) | |
| 21−40 | 1 (25.0) | 3 (75.0) | |
| 41−60 | 1 (50.0) | 1 (50.0) | |
| 61 + | 112 (52.6) | 101 (47.4) | |
| Coffee-drinking | 0.235 | ||
| No | 68 (54.8) | 56 (45.2) | |
| Yes | 1 (20.0) | 4 (80.0) | |
| Carbon monoxide poisoning | 0.623 | ||
| No | 84 (46.9) | 95 (53.1) | |
| Yes | 6 (54.5) | 5 (45.5) | |
| Traumatic brain injury | 0.381 | ||
| No | 85 (46.7) | 97 (53.3) | |
| Yes | 5 (62.5) | 3 (37.5) | |
| Diabetes | 0.921 | ||
| No | 85 (51.2) | 81 (48.8) | |
| Yes | 26 (52.0) | 24 (48.0) | |
| Hypertension | 0.660 | ||
| No | 58 (50.0) | 58 (50.0) | |
| Yes | 53 (53.0) | 47 (47.0) | |
| Hyperlipidemia | 0.902 | ||
| No | 102 (51.5) | 96 (48.5) | |
| Yes | 9 (50.0) | 9 (50.0) | |
| Atrial fibrillation | 0.522 | ||
| No | 106 (51.0) | 102 (49.0) | |
| Yes | 5 (62.5) | 3 (37.5) |
| Characteristics | AD (n = 118) | PDD (n = 110) | P |
|---|---|---|---|
| REM sleep behavior disorders | 0.003 | ||
| No | 74 (67.3) | 36 (32.7) | |
| Yes | 17 (23.9) | 54 (76.1) | |
| Depression (GDS) | 0.004 | ||
| No | 53 (62.4) | 32 (37.6) | |
| Yes | 22 (37.9) | 36 (62.1) | |
| K-MMSE, mean ± SD | 17.6 ± 5.9 | 18.5 ± 5.6 | 0.283 |
| K-MoCA, mean ± SD | 9.6 ± 5.5 | 11.7 ± 5.4 | 0.033 |
| Global CDR score, mean ± SD | 1.2 ± 0.8 | 1.0 ± 0.7 | 0.011 |
| Sum of boxes in CDR, mean ± SD | 7.2 ± 6.6 | 5.2 ± 4.9 | 0.037 |
| K-IADL, mean ± SD | 3.0 ± 5.1 | 3.1 ± 5.5 | 0.963 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, H. Application of Machine Learning Technique to Distinguish Parkinson’s Disease Dementia and Alzheimer’s Dementia: Predictive Power of Parkinson’s Disease-Related Non-Motor Symptoms and Neuropsychological Profile. J. Pers. Med. 2020, 10, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10020031
Byeon H. Application of Machine Learning Technique to Distinguish Parkinson’s Disease Dementia and Alzheimer’s Dementia: Predictive Power of Parkinson’s Disease-Related Non-Motor Symptoms and Neuropsychological Profile. Journal of Personalized Medicine. 2020; 10(2):31. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10020031
Chicago/Turabian StyleByeon, Haewon. 2020. "Application of Machine Learning Technique to Distinguish Parkinson’s Disease Dementia and Alzheimer’s Dementia: Predictive Power of Parkinson’s Disease-Related Non-Motor Symptoms and Neuropsychological Profile" Journal of Personalized Medicine 10, no. 2: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10020031