Prediction of Major Depressive Disorder Following Beta-Blocker Therapy in Patients with Cardiovascular Diseases

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Design
2.2.1. Study Population and Outcome
2.2.2. Variables and Analysis
3. Results
3.1. Baseline Characteristics
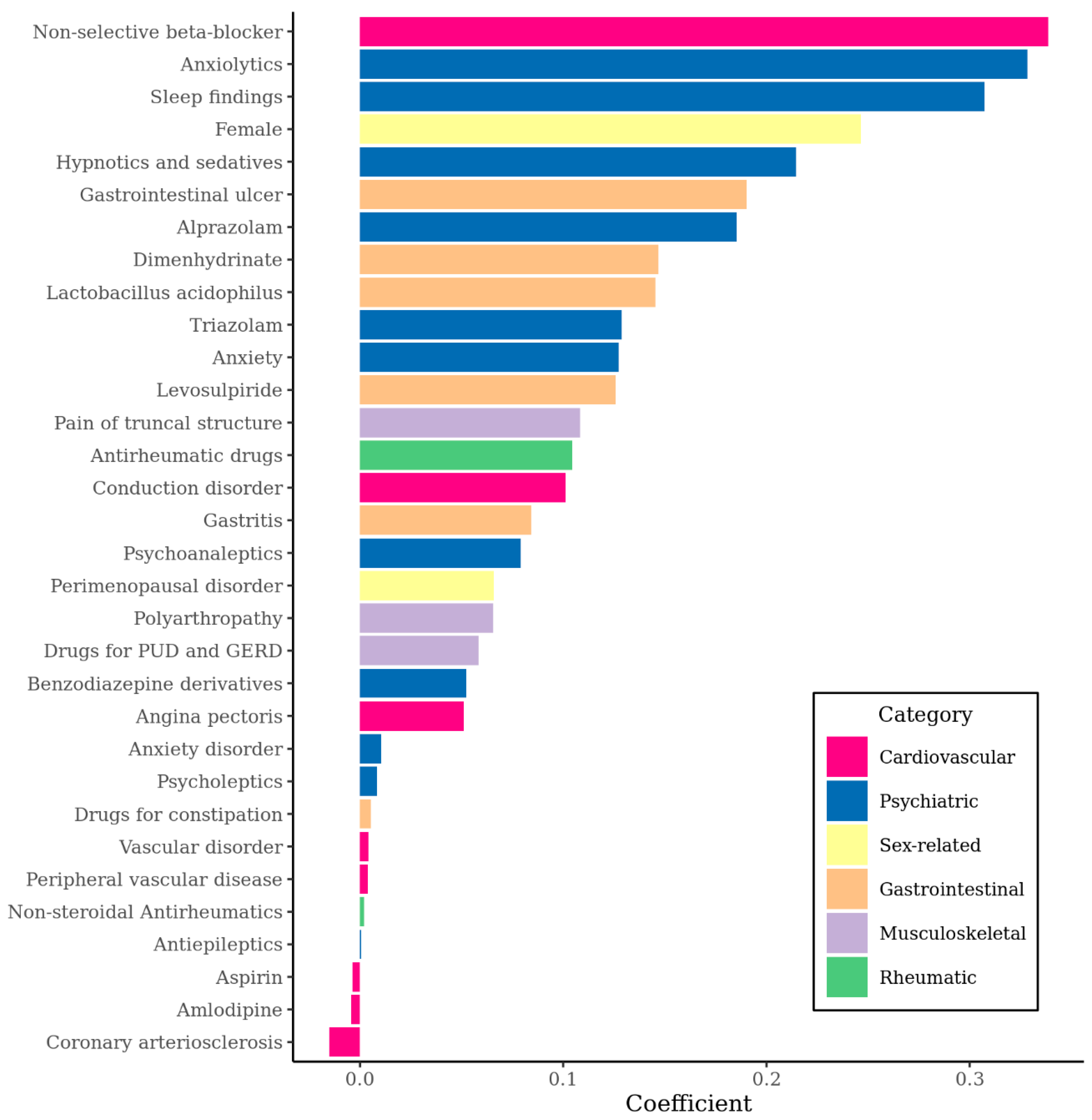
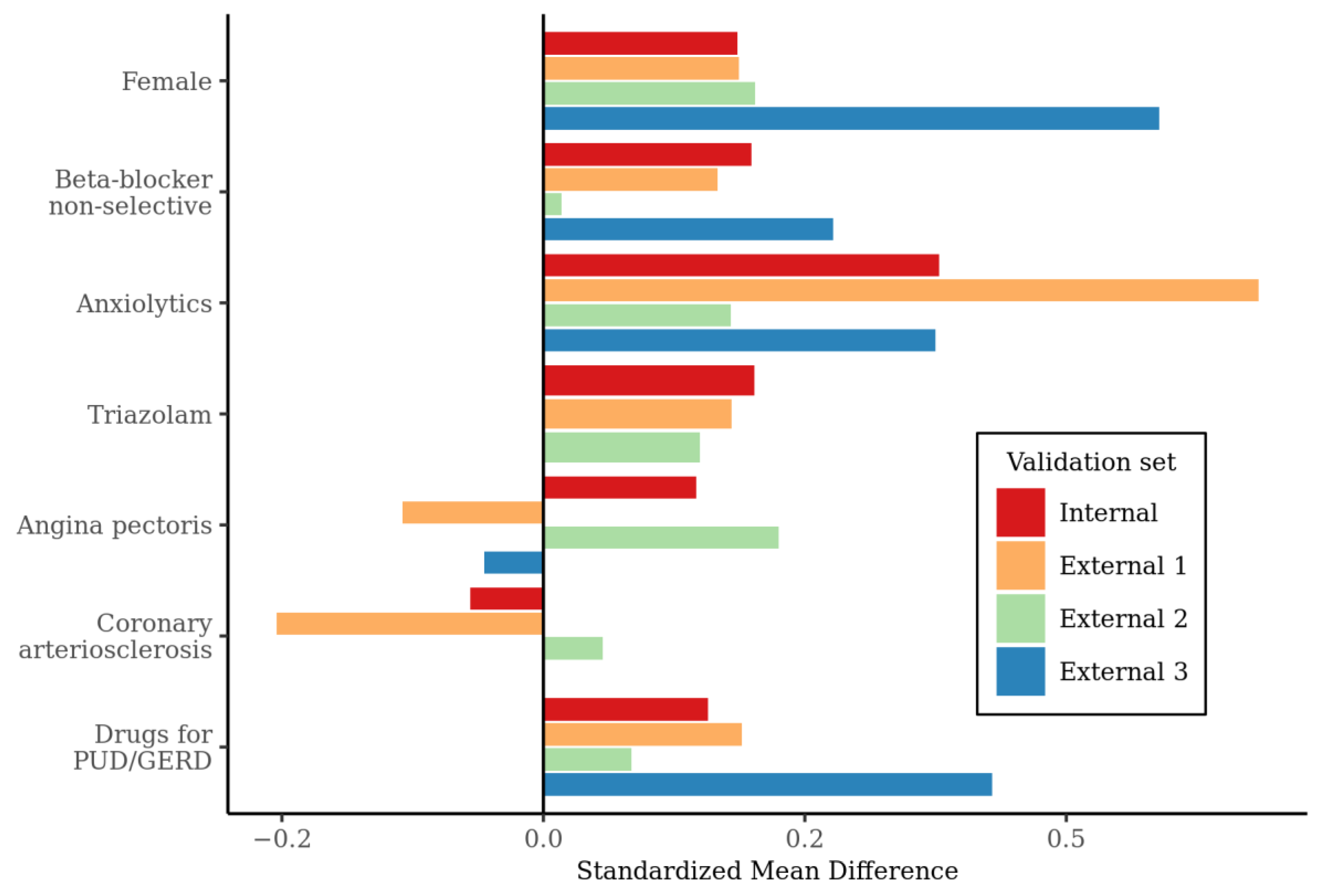
3.2. Variables
3.3. Model Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef] [Green Version]
- Strik, J.J.; Denollet, J.; Lousberg, R.; Honig, A. Comparing symptoms of depression and anxiety as predictors of cardiac events and increased health care consumption after myocardial infarction. J. Am. Coll. Cardiol. 2003, 42, 1801–1807. [Google Scholar] [CrossRef] [Green Version]
- Van Melle, J.P.; De Jonge, P.; Spijkerman, T.A.; Tijssen, J.G.; Ormel, J.; Van Veldhuisen, D.J.; Van Den Brink, R.H.; Van Den Berg, M.P. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: A meta-analysis. Psychosom. Med. 2004, 66, 814–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, R.M.; Freedland, K.E. Depression and coronary heart disease. Nat. Rev. Cardiol. 2017, 14, 145. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-M.; Stewart, R.; Lee, Y.-S.; Lee, H.-J.; Kim, M.C.; Kim, J.-W.; Kang, H.-J.; Bae, K.-Y.; Kim, S.-W.; Shin, I.-S. Effect of escitalopram vs placebo treatment for depression on long-term cardiac outcomes in patients with acute coronary syndrome: A randomized clinical trial. JAMA 2018, 320, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, R.M.; Freedland, K.E.; Steinmeyer, B.C.; Rubin, E.H.; Rich, M.W. Clinical predictors of depression treatment outcomes in patients with coronary heart disease. J. Psychosom. Res. 2016, 88, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Avorn, J.; Everitt, D.E.; Weiss, S. Increased Antidepressant Use in Patients Prescribed β-Blockers. JAMA 1986, 255, 357–360. [Google Scholar] [CrossRef]
- Thiessen, B.Q.; Wallace, S.M.; Blackburn, J.L.; Wilson, T.W.; Bergman, U. Increased Prescribing of Antidepressants Subsequent to ß-Blocker Therapy. Arch. Intern. Med. 1990, 150, 2286–2290. [Google Scholar] [CrossRef]
- Boal, A.H.; Smith, D.J.; McCallum, L.; Muir, S.; Touyz, R.M.; Dominiczak, A.F.; Padmanabhan, S. Monotherapy with major antihypertensive drug classes and risk of hospital admissions for mood disorders. Hypertension 2016, 68, 1132–1138. [Google Scholar] [CrossRef]
- Luc, P.; Sheldon, W.T. Contemporary Use of β-Blockers: Clinical Relevance of Subclassification. Can J. Cardiol. 2014, 30, S9–S15. [Google Scholar]
- Bavishi, C.; Chatterjee, S.; Ather, S.; Patel, D.; Messerli, F.H. Beta-blockers in heart failure with preserved ejection fraction: A meta-analysis. Heart Fail. Rev. 2015, 20, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Dondo, T.B.; Hall, M.; West, R.M.; Jernberg, T.; Lindahl, B.; Bueno, H.; Danchin, N.; Deanfield, J.E.; Hemingway, H.; Fox, K.A. β-blockers and mortality after acute myocardial infarction in patients without heart failure or ventricular dysfunction. J. Am. Coll. Cardiol. 2017, 69, 2710–2720. [Google Scholar] [CrossRef] [PubMed]
- Wiysonge, C.S.; Bradley, H.A.; Volmink, J.; Mayosi, B.M.; Opie, L.H. Beta-blockers for hypertension. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [Green Version]
- Bangalore, S.; Steg, G.; Deedwania, P.; Crowley, K.; Eagle, K.A.; Goto, S.; Ohman, E.M.; Cannon, C.P.; Smith, S.C.; Zeymer, U. β-Blocker use and clinical outcomes in stable outpatients with and without coronary artery disease. JAMA 2012, 308, 1340–1349. [Google Scholar] [CrossRef]
- Smith, C.M. Origin and uses of primum non nocere—Above all, do no harm! J. Clin. Pharmacol. 2005, 45, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.M.; Williams, J.L.; Burnham, T.G.; Prevost, A.T.; Schiff, R.; Erskine, S.D.; Davies, J.G. Predicting adverse drug reactions in older adults; a systematic review of the risk prediction models. Clin. Interv. Aging 2014, 9, 1581. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Yue, Y.; Jiang, H.; Lu, J.; Wu, A.; Geng, D.; Wang, J.; Lu, J.; Li, S.; Tang, H. A risk prediction model for post-stroke depression in Chinese stroke survivors based on clinical and socio-psychological features. Oncotarget 2017, 8, 62891. [Google Scholar] [CrossRef] [Green Version]
- Cattelani, L.; Murri, M.B.; Chesani, F.; Chiari, L.; Bandinelli, S.; Palumbo, P. Risk prediction model for late life depression: Development and validation on three large European datasets. IEEE J. Biomed. Health Inform. 2018, 23, 2196–2204. [Google Scholar] [CrossRef]
- Chua, W.; Purmah, Y.; Cardoso, V.R.; Gkoutos, G.V.; Tull, S.P.; Neculau, G.; Thomas, M.R.; Kotecha, D.; Lip, G.Y.; Kirchhof, P. Data-driven discovery and validation of circulating blood-based biomarkers associated with prevalent atrial fibrillation. Eur. Heart J. 2019, 40, 1268–1276. [Google Scholar] [CrossRef] [Green Version]
- Reps, J.M.; Schuemie, M.J.; Suchard, M.A.; Ryan, P.B.; Rijnbeek, P.R. Design and implementation of a standardized framework to generate and evaluate patient-level prediction models using observational healthcare data. J. Am. Med. Inform. Assoc. 2018, 25, 969–975. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort profile: The national health insurance service–national sample cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.; Posada, J.; Olson, G.; Li, W.; O’Reilly, C.; Balraj, D.; Mesterhazy, J.; Pallas, J.; Desai, P.; Shah, N. A new paradigm for accelerating clinical data science at Stanford Medicine. arXiv 2020, arXiv:2003.10534. [Google Scholar]
- FitzHenry, F.; Resnic, F.; Robbins, S.; Denton, J.; Nookala, L.; Meeker, D.; Ohno-Machado, L.; Matheny, M. Creating a common data model for comparative effectiveness with the observational medical outcomes partnership. Appl. Clin. Inform. 2015, 6, 536. [Google Scholar] [PubMed] [Green Version]
- Hripcsak, G.; Duke, J.D.; Shah, N.H.; Reich, C.G.; Huser, V.; Schuemie, M.J.; Suchard, M.A.; Park, R.W.; Wong, I.C.K.; Rijnbeek, P.R. Observational Health Data Sciences and Informatics (OHDSI): Opportunities for observational researchers. Stud. Health Technol. Inform. 2015, 216, 574. [Google Scholar]
- Christodoulou, E.; Ma, J.; Collins, G.S.; Steyerberg, E.W.; Verbakel, J.Y.; Van Calster, B. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J. Clin. Epidemiol. 2019, 110, 12–22. [Google Scholar] [CrossRef]
- Sanchez-Pinto, L.N.; Venable, L.R.; Fahrenbach, J.; Churpek, M.M. Comparison of variable selection methods for clinical predictive modeling. Int. J. Med. Inform. 2018, 116, 10–17. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) The TRIPOD Statement. Circulation 2015, 131, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Agustini, B.; Mohebbi, M.; Woods, R.L.; McNeil, J.J.; Nelson, M.R.; Shah, R.C.; Murray, A.M.; Ernst, M.E.; Reid, C.M.; Tonkin, A. The association of antihypertensive use and depressive symptoms in a large older population with hypertension living in Australia and the United States: A cross-sectional study. J. Hum. Hypertens. 2020, 34, 787–794. [Google Scholar] [CrossRef]
- Kessing, L.V.; Rytgaard, H.C.; Ekstrøm, C.T.; Torp-Pedersen, C.; Berk, M.; Gerds, T.A. Antihypertensive drugs and risk of depression: A nationwide population-based study. Hypertension 2020, 76, 1263–1279. [Google Scholar] [CrossRef]
- Armstrong, C.; Kapolowicz, M.R. A Preliminary Investigation on the Effects of Atenolol for Treating Symptoms of Anxiety. Mil. Med. 2020, usaa170. [Google Scholar] [CrossRef]
- Luijendijk, H.J.; Koolman, X. The incentive to publish negative studies: How beta-blockers and depression got stuck in the publication cycle. J. Clin. Epidemiol. 2012, 65, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Haug, T.T.; Mykletun, A.; Dahl, A.A. The association between anxiety, depression, and somatic symptoms in a large population: The HUNT-II study. Psychosom. Med. 2004, 66, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Fuetsch, M.; Müller, N.; Höfler, M.; Lieb, R.; Wittchen, H.-U. Social anxiety disorder and the risk of depression: A prospective community study of adolescents and young adults. Arch. Gen. Psychiatry 2001, 58, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huffman, J.C.; Celano, C.M.; Januzzi, J.L. The relationship between depression, anxiety, and cardiovascular outcomes in patients with acute coronary syndromes. Neuropsychiatr. Dis. Treat. 2010, 6, 123. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Cahalan, C.; Mensing, G.; Smith, M.; Haythornthwaite, J.A. Pain, catastrophizing, and depression in the rheumatic diseases. Nat. Rev. Rheumatol. 2011, 7, 216. [Google Scholar] [CrossRef] [PubMed]
- Magni, G.; Moreschi, C.; Rigatti-Luchini, S.; Merskey, H. Prospective study on the relationship between depressive symptoms and chronic musculoskeletal pain. Pain 1994, 56, 289–297. [Google Scholar] [CrossRef]
- Kessler, R.C.; McGonagle, K.A.; Swartz, M.; Blazer, D.G.; Nelson, C.B. Sex and depression in the National Comorbidity Survey I: Lifetime prevalence, chronicity and recurrence. J. Affect. Disord. 1993, 29, 85–96. [Google Scholar] [CrossRef] [Green Version]
- Nolen-Hoeksema, S. Sex differences in unipolar depression: Evidence and theory. Psychol. Bull. 1987, 101, 259. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-J.; Park, Y.; Yoo, K.-H.; Kim, K.-T.; Kim, E.-S.; Kim, J.-W.; Kim, S.-W.; Shin, I.-S.; Yoon, J.-S.; Kim, J.H. Sex differences in the genetic architecture of depression. Sci. Rep. 2020, 10, 9927. [Google Scholar] [CrossRef]
- Bromberger, J.T.; Assmann, S.F.; Avis, N.E.; Schocken, M.; Kravitz, H.M.; Cordal, A. Persistent mood symptoms in a multiethnic community cohort of pre-and perimenopausal women. Am. J. Epidemiol. 2003, 158, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.E.; Jo, M.-W.; Shin, Y.-W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Outcome (n = 774) | Non-Outcome (n = 49,623) | p-Value |
|---|---|---|---|
| Age (years, mean ± standard deviation (SD)) | 61.2 ± 12.9 | 58.7 ± 13.1 | 0.510 |
| Male 1 | 298 (38.5) | 25,527 (51.4) | <0.001 |
| Beta-blocker indication 2 | |||
| Hypertensive disorder | 726 (93.8) | 47,321 (95.4) | 0.050 |
| Myocardial infarction | 46 (5.9) | 2456 (4.9) | 0.238 |
| Angina pectoris | 205 (26.5) | 8899 (17.9) | <0.001 |
| Coronary arteriosclerosis | 13 (1.7) | 1592 (3.2) | 0.021 |
| Heart failure | 98 (12.7) | 4688 (9.4) | 0.003 |
| Chronic disease 3 | |||
| Cancer | 24 (3.1) | 1056 (2.1) | 0.084 |
| Chronic lung disease | 98 (12.7) | 4621 (9.3) | 0.002 |
| Stroke | 45 (5.8) | 1441 (2.9) | <0.001 |
| Alzheimer’s disease | 7 (0.9) | 114 (0.2) | <0.001 |
| Diabetes | 135 (17.4) | 9691 (19.5) | 0.159 |
| Chronic kidney disease | 12 (1.6) | 490 (1.0) | 0.167 |
| Mental disorder | |||
| Anxiety disorder | 150 (14.9) | 3911 (7.9) | <0.001 |
| Neurosis | 62 (8.0) | 1731 (3.5) | <0.001 |
| Organic mental disorder | 30 (3.9) | 603 (1.2) | <0.001 |
| Adjustment disorder | 6 (0.8) | 116 (0.2) | 0.012 |
| Personality disorder | 0 (0.0) | 60 (0.1) | 1.000 |
| Delusional disorder | 1 (0.1) | 14 (0.0) | 0.207 |
| Nutritional disorder | |||
| Vitamin deficiency | 9 (1.2) | 301 (0.6) | 0.08 |
| Undernutrition | 16 (2.1) | 371 (0.7) | <0.001 |
| Medication 3 | |||
| VKA | 13 (1.7) | 599 (1.2) | 0.305 |
| Aspirin | 304 (39.3) | 10,990 (22.1) | <0.001 |
| Antiplatelet agents | 66 (8.5) | 2604 (5.2) | <0.001 |
| ACEi | 165 (21.5) | 4795 (9.7) | <0.001 |
| Angiotensin II receptor blocker | 233 (30.1) | 14,926 (30.1) | 1.000 |
| Selective beta-blocker | 556 (71.8) | 37,234 (75.0) | 0.046 |
| Non-selective beta-blocker | 375 (48.4) | 17,768 (35.8) | <0.001 |
| Hydrophilic beta-blocker | 543 (71.8) | 36,302 (73.2) | 0.068 |
| Lipophilic beta-blocker | 388 (50.1) | 18,700 (37.7) | <0.001 |
| Diuretic | 400 (51.7) | 25,985 (52.4) | 0.732 |
| Calcium channel antagonist | 415 (53.6) | 28,057 (56.5) | 0.112 |
| Cardiac glycoside | 26 (3.4) | 1575 (3.2) | 0.851 |
| Aldosterone antagonist | 52 (6.7) | 2846 (5.7) | 0.277 |
| Verapamil/diltiazem | 80 (10.3) | 3204 (6.5) | <0.001 |
| Antiarrhythmics | 14 (1.8) | 517 (1.0) | 0.058 |
| Other immunosuppressants 4 | 1 (0.1) | 153 (0.3) | 0.735 |
| Calcineurin inhibitors | 4 (0.5) | 132 (0.3) | 0.157 |
| Selective immunosuppressants | 1 (0.1) | 78 (0.2) | 1.000 |
| Tumor necrosis factor alpha -inhibitor | 0 (0.0) | 2 (0.0) | 1.000 |
| Validation Set | Name | n | Outcome | Incidence (%) | AUC | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| Internal | NHIS | 10,078 | 154 | 1.53 | 0.74 | 83.1% | 49.5% |
| External 1 | Ajou | 8511 | 19 | 0.22 | 0.71 | 78.9% | 49.0% |
| External 2 | Hanyang | 5112 | 15 | 0.29 | 0.66 | 86.7% | 49.4% |
| External 3 | Kandong | 5097 | 26 | 0.51 | 0.70 | 80.8% | 49.9% |
| External 4 | STARR | 26,258 | 439 | 1.67 | 0.62 | 77.2% | 40.4% |
| External 5 | OpenClaims | 4,295,013 | 59,045 | 1.38 | 0.62 | 75.1% | 40.2% |
| External 6 | AmbEMR | 883,198 | 3342 | 0.38 | 0.62 | 75.4% | 40.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, S.; Kostka, K.; Posada, J.D.; Kim, Y.; Seo, S.I.; Lee, D.Y.; Shah, N.H.; Roh, S.; Lim, Y.-H.; Chae, S.G.; et al. Prediction of Major Depressive Disorder Following Beta-Blocker Therapy in Patients with Cardiovascular Diseases. J. Pers. Med. 2020, 10, 288. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040288
Jin S, Kostka K, Posada JD, Kim Y, Seo SI, Lee DY, Shah NH, Roh S, Lim Y-H, Chae SG, et al. Prediction of Major Depressive Disorder Following Beta-Blocker Therapy in Patients with Cardiovascular Diseases. Journal of Personalized Medicine. 2020; 10(4):288. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040288
Chicago/Turabian StyleJin, Suho, Kristin Kostka, Jose D. Posada, Yeesuk Kim, Seung In Seo, Dong Yun Lee, Nigam H. Shah, Sungwon Roh, Young-Hyo Lim, Sun Geu Chae, and et al. 2020. "Prediction of Major Depressive Disorder Following Beta-Blocker Therapy in Patients with Cardiovascular Diseases" Journal of Personalized Medicine 10, no. 4: 288. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm10040288