Blood Biomarkers for Assessing Headaches in Healthcare Workers after Wearing Biological Personal Protective Equipment in a COVID-19 Field Hospital

 ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Study Protocol and Measures
2.4. Outcome and Data Abstraction
2.5. Missing Data
2.6. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Balachandar, V.; Mahalaxmi, I.; Kaavya, J.; Vivekanandhan, G.; Ajithkumar, S.; Arul, N.; Singaravelu, G.; Kumar, N.S.; Devi, S.M. COVID-19: Emerging protective measures. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3422–3425. [Google Scholar] [PubMed]
- Rowan, N.J.; Laffey, J.G. Challenges and solutions for addressing critical shortage of supply chain for personal and protective equipment (PPE) arising from Coronavirus disease (COVID19) pandemic—Case study from the Republic of Ireland. Sci. Total Environ. 2020, 725, 13853. [Google Scholar] [CrossRef]
- Moss, P.; Barlow, G.; Easom, N.; Lillie, P.; Samson, A. Lessons for managing high-consequence infections from first COVID-19 cases in the UK. Lancet 2020, 395, e46. [Google Scholar] [CrossRef] [Green Version]
- Huh, S. How to train the health personnel for protecting themselves from novel coronavirus (COVID-19) infection during their patient or suspected case care. J. Educ. Eval. Health Prof. 2020, 17, 10. [Google Scholar] [CrossRef]
- Sim, M.R. The COVID-19 pandemic: Major risks to healthcare and other workers on the front line. Occup. Environ. Med. 2020, 77, 281–282. [Google Scholar] [CrossRef] [Green Version]
- Ong, J.J.Y.; Bharatendu, C.; Goh, Y.; Tang, J.Z.Y.; Sooi, K.W.X.; Tan, Y.L.; Tan, B.Y.Q.; Teoh, H.-L.; Ong, S.T.; Allen, D.M.; et al. Headaches Associated with Personal Protective Equipment—A Cross-Sectional Study among Frontline Healthcare Workers during COVID-19. Headache 2020. [Google Scholar] [CrossRef] [Green Version]
- Khalid, I.; Khalid, T.J.; Qabajah, M.R.; Barnard, A.G.; Qushmaq, I.A. Healthcare Workers Emotions, Perceived Stressors and Coping Strategies during a MERS-CoV Outbreak. Clin. Med. Res. 2016, 14, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.D.; Wu, J.; Williams, T.C.; Loberger, J.M.; Hudson, M.F.; Burdine, J.R.; Wagner, P.J. The experience of headaches in health care workers: Opportunity for care improvement. Headache 2013, 53, 962–969. [Google Scholar] [CrossRef]
- Xie, W.; Li, R.; He, M.; Cui, F.; Sun, T.; Xiong, J.; Zhao, D.; Na, W.; Liu, R.; Yu, S. Prevalence and risk factors associated with headache amongst medical staff in South China. J. Headache Pain 2020, 21, 5. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xie, J.; Yang, F.; Wu, S.; Wang, H.; Zhang, X.; Liu, H.; Deng, X.; Yu, S. The prevalence of primary headache disorders and their associated factors among nursing staff in North China. J. Headache Pain 2015, 16, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferroni, P.; Barbanti, P.; Spila, A.; Fratangeli, F.; Aurilia, C.; Fofi, L.; Gabriella, E.; Fiorella, G. Circulating Biomarkers in Migraine: New Opportunities for Precision Medicine. Curr. Med. Chem. 2019, 26, 6191–6205. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, K.K.; Rice, M.J. Point-of-Care Blood Testing: The Technology behind the Numbers. Anesth. Analg. 2019, 129, 92–98. [Google Scholar] [CrossRef]
- Loder, E.; Cardona, L. Evaluation for secondary causes of headache: The role of blood and urine testing. Headache 2011, 51, 338–345. [Google Scholar] [CrossRef]
- Evans, R.W. Diagnostic Testing for Migraine and Other Primary Headaches. Neurol. Clin. 2019, 37, 707–725. [Google Scholar] [CrossRef]
- Reynolds, R.M.; Padfield, P.L.; Seckl, J.R. Disorders of sodium balance. BMJ 2006, 332, 702–705. [Google Scholar] [CrossRef] [Green Version]
- Sharp, M.K.; Bertizzolo, L.; Rius, R.; Wager, E.; Gómez, G.; Hren, D. Using the STROBE statement: Survey findings emphasized the role of journals in enforcing reporting guidelines. J. Clin. Epidemiol. 2019, 116, 26–35. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Safe Use of Personal Protective Equipment in the Treatment of Infectious Diseases of High Consequence; ECDC: Stockholm, Sweden, 2014. [Google Scholar]
- Rahmani, Z.; Kochanek, A.; Astrup, J.J.; Poulsen, J.N.; Gazerani, P. Helmet-induced headache among Danish military personnel. Scand. J. Public Health 2017, 45, 818–823. [Google Scholar] [CrossRef]
- Harrison, M.; Coffey, B.; Wayne, W.; Fischer, S. Night Vision Goggle-Induced Neck Pain in Military Helicopter Aircrew: A Literature Review. Aerosp. Med. Hum. Perform. 2015, 86, 46–55. [Google Scholar] [CrossRef]
- Kim, J.H.; Wu, T.; Powell, J.B.; Roberge, R.J. Physiologic and fit factor profiles of N95 and P100 filtering facepiece respirators for use in hot, humid environments. Am. J. Infect. Control 2016, 44, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.C.H.; Seet, R.C.S.; Lee, K.H.; Wilder-Smith, E.P.V.; Chuah, B.Y.S.; Ong, B.K.C. Headaches and the N95 face-mask amongst healthcare providers. Acta Neurol. Scand. 2006, 113, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Roberge, R.J.; Coca, A.; Williams, W.J.; Palmiero, A.J.; Powell, J.B. Surgical mask placement over N95 filtering facepiece respirators: Physiological effects on healthcare workers. Respirology 2010, 15, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Offeddu, V.; Yung, C.F.; Low, M.S.F.; Tam, C.C. Effectiveness of Masks and Respirators against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2017, 65, 1934–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacIntyre, C.R.; Wang, Q.; Cauchemez, S.; Seale, H.; Dwyer, D.E.; Yang, P.; Shi, W.; Gao, Z.; Pang, X.; Zhang, Y.; et al. A cluster randomized clinical trial comparing fit-tested and non-fit-tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza Respir. Viruses 2011, 5, 170–179. [Google Scholar] [CrossRef]
- Smith, J.D.; MacDougall, C.C.; Johnstone, J.; Copes, R.A.; Schwartz, B.; Garber, G.E. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: A systematic review and meta-analysis. CMAJ 2016, 188, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Radonovich, L.J.; Simberkoff, M.S.; Bessesen, M.T.; Brown, A.C.; Cummings, D.A.T.; Gaydos, C.A.; Los, J.G.; Krosche, A.E.; Gibert, C.L.; Gorse, G.J.; et al. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA 2019, 322, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Gozubatik-Celik, G.; Uluduz, D.; Goksan, B.; Akkaya, N.; Sohtaoglu, M.; Uygunoglu, U.; Kircelli, F.; Sezen, A.; Saip, S.; Savrun, F.K.; et al. Hemodialysis-related headache and how to prevent it. Eur. J. Neurol. 2019, 26, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Poyrazoğlu, H.G.; Öztürk, A.B. Predictive value of laboratory parameters in childhood migraine. Acta Neurol. Belg. 2019. [Google Scholar] [CrossRef]
- Blau, J.; Kell, C.; Sperling, J. Water-deprivation headache: A new headache with two variants. Headache 2004, 44, 79–83. [Google Scholar] [CrossRef]
- Ooi, S.; Koh-Tai, B.; Aw, T.; Lau, T.; Chan, S. Assessment of dehydration in adults using hematologic and biochemical tests. Acad. Emerg. Med. 1997, 4, 840–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pundir, C.S.; Kumar, P.; Jaiwal, R. Biosensing methods for determination of creatinine: A review. Biosens. Bioelectron. 2019, 126, 707–724. [Google Scholar] [CrossRef] [PubMed]
- Cánovas, R.; Cuartero, M.; Crespo, G.A. Modern creatinine (Bio)sensing: Challenges of point-of-care platforms. Biosens. Bioelectron. 2019, 130, 110–124. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mask Type | ||
|---|---|---|
| N95 | FFP2 | |
| FDA-cleared | No | No |
| Exhalation valve | No | Yes |
| Model number (3M) | 3M™ Particulate Respirator 8210, N95 | 3M™ Aura™ Particulate Respirator 9211+/37193(AAD) |
| Protects against airborne particles | Yes | Yes |
| 95% filtration efficiency of aerosol particles | Yes | Yes |
| Latex | No | No |
| Price (Box of 10) | $12.99 | $22.49 |
| Headache | |||||
|---|---|---|---|---|---|
| Characteristic 1 | Total n = 36 | No n = 21 | Yes n = 17 | Odds Ratio (95%CI) | p-Value |
| Age (years) | 29 (26–44) | 29 (26–42) | 30 (27–45) | 1.01 (0.95–1.07) | 0.674 2 |
| Gender (female) | 28 (73.7) | 18 (64.3) | 10 (35.7) | 4.20 (0.88–19.94) | 0.071 3 |
| Employment | |||||
| Physician | 12 (31.6) | 6 (28.6) | 6 (35.3) | ||
| Nurse | 15 (39.5) | 8 (38.1) | 7 (41.2) | 1.75 (0.32–9.29) | 0.511 3 |
| M. assistant | 11 (28.9) | 7 (33.3) | 4 (23.5) | 1.53 (0.31–7.53) | 0.600 3 |
| Mask type | |||||
| N95 | 19 (50.0) | 7 (33.3) | 12 (70.6) | ||
| FFP2 | 19 (50.0) | 14 (66.7) | 5 (29.4) | 4.80 (1.20–19.12) | 0.026 3 |
| PPE time (hours) | 4:10 (4:01–4:25) | 4:10 (4:03–4:25) | 4:05 (3:58–4:21) | 1.00 (0.99–1.00) | 0.640 2 |
| Blood test | |||||
| Na+ (mEq/L) | 141 (140–143) | 141 (140–142) | 142 (140–143) | 1.12 (0.77–1.62) | 0.530 2 |
| K+ (mEq/L) | 3.9 (3.6–4.0) | 4.0 (3.8–4.0) | 3.8 (3.5–4.0) | 0.26 (0.02–2.63) | 0.257 2 |
| Ca++ (mEq/L) | 1.27 (1.23–1.29) | 1.27 (1.25–1.29) | 1.25 (1.23–1.29) | NA | 0.495 2 |
| Cl− (mEq/L) | 104 (103–105) | 104 (103–105) | 104 (103–105) | 1.08 (0.71–1.66) | 0.701 2 |
| Urea (mg/dL) | 5.1 (4.4–5.7) | 5.1 (4.5–5.5) | 5.0 (4.2–6.5) | 1.38 (0.79–2.41) | 0.252 2 |
| Crea (mg/dL) | 0.91 (0.76–1.03) | 0.83 (0.72–0.96) | 0.99 (0.87–1.11) | 241.36 (2.50–23,295.43) | 0.019 2 |
| BUN (mg/dL) | 12 (10–13) | 12 (10–13) | 13 (10–15) | 1.11 (0.91–1.36) | 0.287 2 |
| Glu (mg/dL) | 96 (90–103) | 96 (88–103) | 96 (91–106) | 1.00 (0.96–1.04) | 0.936 2 |
| Lac (mmol/L) | 1.13 (0.81–1.53) | 1.13 (0.83–1.47) | 1.14 (0.79–1.53) | 1.07 (0.27–4.20) | 0.914 2 |
| Characteristic | Degrees of Freedom | Sum Squares | Mean Squares | F Value | p-Value |
|---|---|---|---|---|---|
| Mask type | 1 | 0.0950 | 0.09500 | 2.903 | 0.097 |
| Headache | 1 | 0.1606 | 0.16064 | 4.909 | 0.033 |
| Mask*Headache | 1 | 0.0013 | 0.00131 | 0.040 | 0.842 |
| Residuals | 34 | 1.1126 | 0.03272 |
| Mask Type | |||
|---|---|---|---|
| Global | N95 | FFP2 | |
| Headache prevalence | 44.7 | 63.2 | 26.3 |
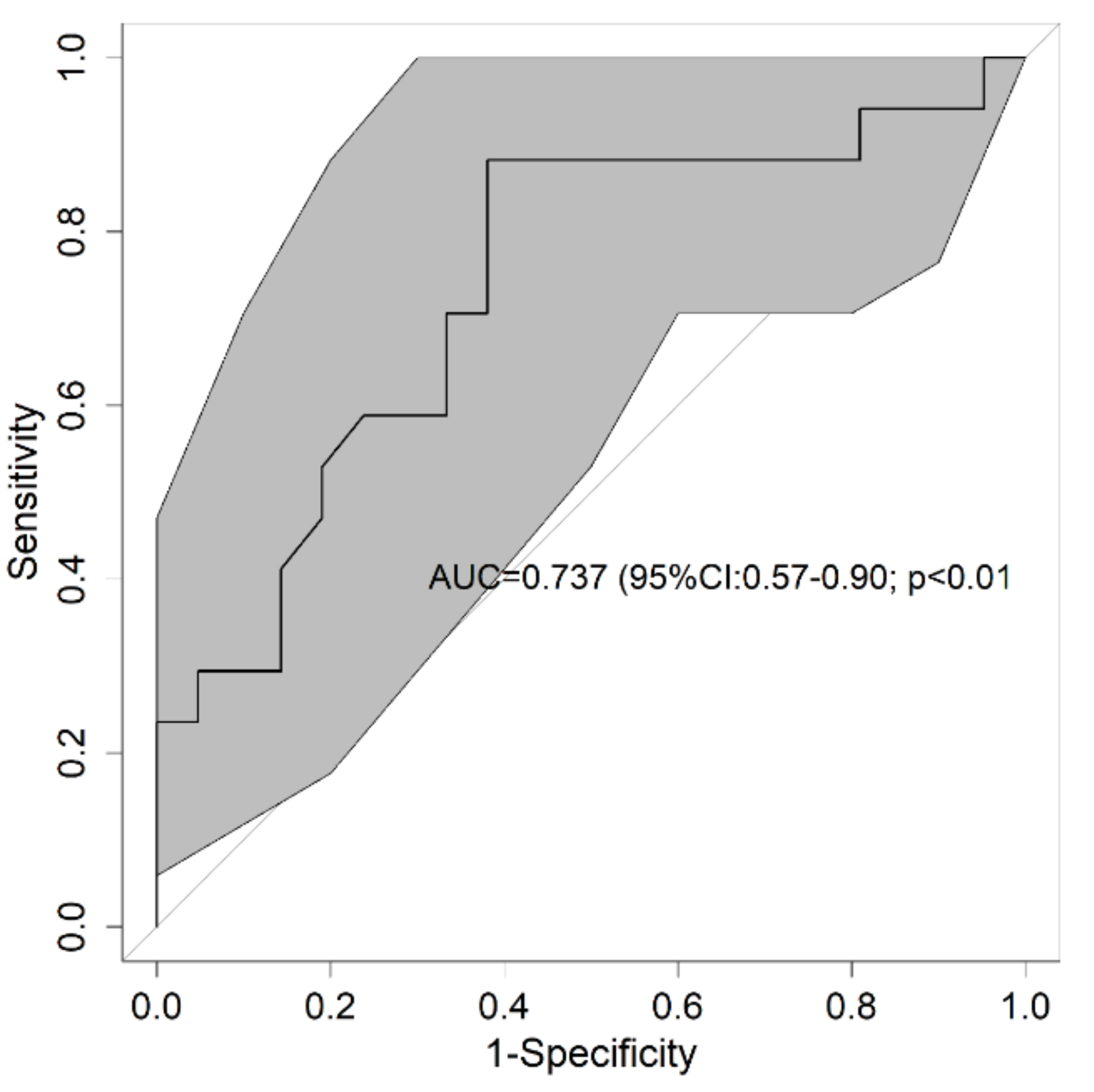
| Creatinine cut-off point (mg/dL) | 0.87 | 1.10 | 0.87 |
| Area under the curve 1 | 0.737 (0.57–0.90) | 0.702 (0.46–0.94) | 0.764 (0.49–1.00) |
| p-value 1 | <0.01 | 0.098 | 0.055 |
| Sensitivity 1 | 88.2 (65.7–96.7) | 41.7 (19.3–68.0) | 100 (56.6–100) |
| Specificity 1 | 61.9 (40.9–79.2) | 100 (64.6–100) | 64.3 (38.8–83.7) |
| Positive predictive value 1 | 65.2 (44.9–81.2) | 100 (56.6–100) | 50.0 (23.7–76.3) |
| Negative predictive value 1 | 86.7 (62.1–96.3) | 50.0 (26.8–73.2) | 100 (70.1–100) |
| Likelihood ratio (+) 1 | 2.32 (1.31–4.10) | 0 | 2.80 (1.39–5.65) |
| Likelihood ratio (-) 1 | 0.19 (0.05–0.73) | 0.58 (0.36–0.94) | 0 |
| Diagnostic accuracy 1 | 73.7 (58.0–86.0) | 63.2 (41.0–80.9) | 73.7 (51.2–88.2) |
| Pretest probability | 44.7 | 63.2 | 26.3 |
| Youden’s test | 0.5 | 0.4 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Rodríguez, F.; López-Izquierdo, R.; Portillo Rubiales, R.M.; Fadrique Millán, L.N.; Carbajosa Rodríguez, V.; Sanz-García, A.; Ortega Rabbione, G.; Polonio-López, B.; Castro Villamor, M.Á.; Martín-Conty, J.L. Blood Biomarkers for Assessing Headaches in Healthcare Workers after Wearing Biological Personal Protective Equipment in a COVID-19 Field Hospital. J. Pers. Med. 2021, 11, 27. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010027
Martín-Rodríguez F, López-Izquierdo R, Portillo Rubiales RM, Fadrique Millán LN, Carbajosa Rodríguez V, Sanz-García A, Ortega Rabbione G, Polonio-López B, Castro Villamor MÁ, Martín-Conty JL. Blood Biomarkers for Assessing Headaches in Healthcare Workers after Wearing Biological Personal Protective Equipment in a COVID-19 Field Hospital. Journal of Personalized Medicine. 2021; 11(1):27. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010027
Chicago/Turabian StyleMartín-Rodríguez, Francisco, Raúl López-Izquierdo, Raquel M. Portillo Rubiales, Laura N. Fadrique Millán, Virginia Carbajosa Rodríguez, Ancor Sanz-García, Guillermo Ortega Rabbione, Begoña Polonio-López, Miguel Ángel Castro Villamor, and José L. Martín-Conty. 2021. "Blood Biomarkers for Assessing Headaches in Healthcare Workers after Wearing Biological Personal Protective Equipment in a COVID-19 Field Hospital" Journal of Personalized Medicine 11, no. 1: 27. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11010027