
Factors Affecting Post-Stroke Depression in Acute Ischemic Stroke Patients after 3 Months

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
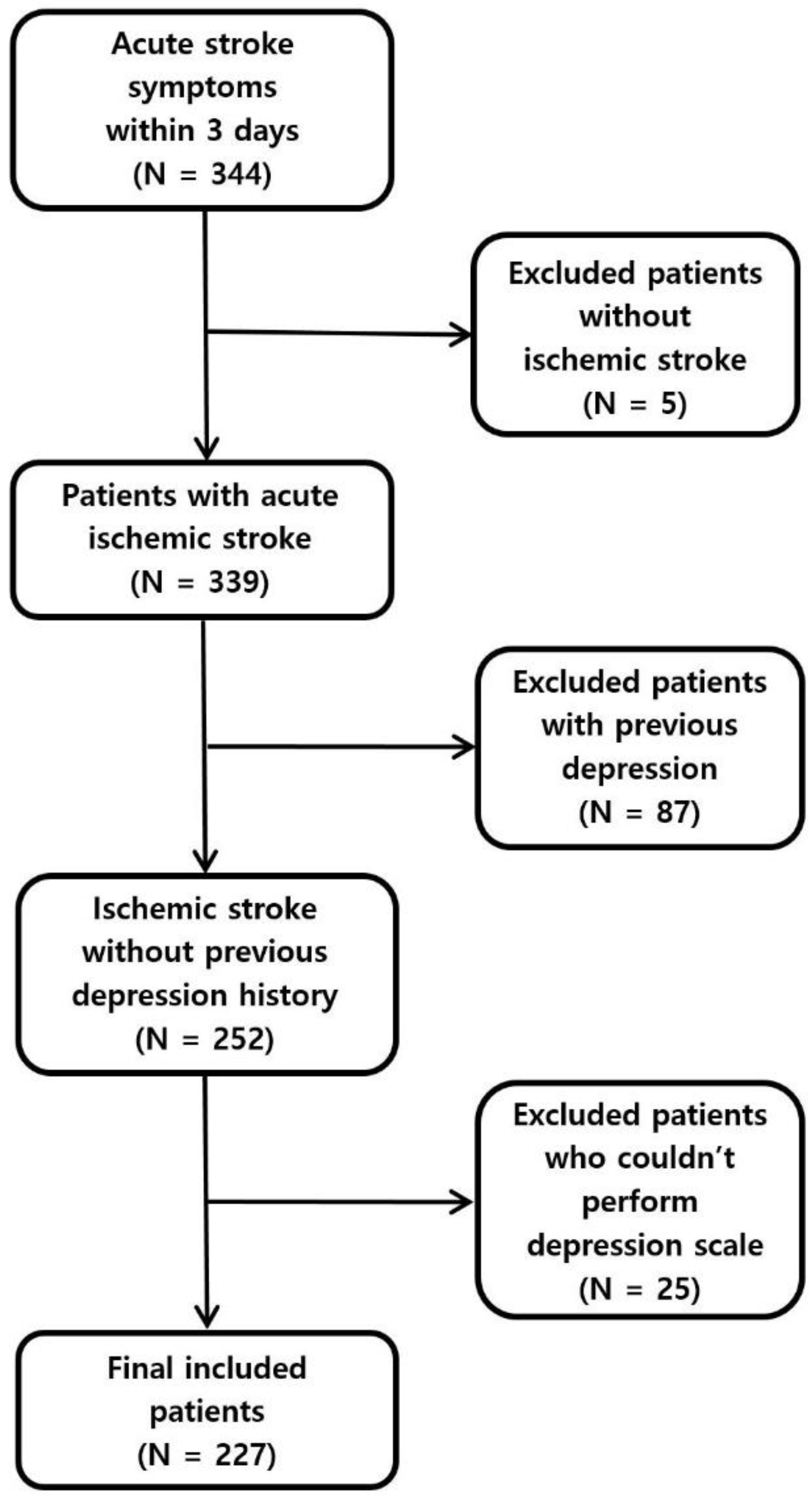
2.1. Patient Selection
2.2. Neuropsychiatric Test
2.3. Diagnosis of Acute Ischemic Stroke
2.4. Classification of Ischemic Stroke
2.5. Statistical Analysis
3. Results
3.1. Factors Affecting PSD Three Months after Ischemic Stroke Occurrence
3.2. Factors Impacting the Improvement of PSD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 9 December 2020).
- Wijeratne, T.; Sales, C. Understanding why post-stroke depression may be the norm rather than the exception: The anatomical and neuroinflammatory correlates of post-stroke depression. J. Clin. Med. 2021, 10, 1674. [Google Scholar] [CrossRef]
- Zhang, E.; Liao, P. Brain-derived neurotrophic factor and post-stroke depression. J. Neurosci. Res. 2020, 98, 537–548. [Google Scholar] [CrossRef]
- Swartz, R.H.; Bayley, M.; Lanctôt, K.L.; Murray, B.J.; Cayley, M.L.; Lien, K.; Sicard, M.N.; Thorpe, K.E.; Dowlatshahi, D.; Mandzia, J.L.; et al. Post-stroke depression, obstructive sleep apnea, and cognitive impairment: Rationale for, and barriers to, routine screening. Int. J. Stroke 2016, 11, 509–518. [Google Scholar] [CrossRef]
- Wang, Z.; Shi, Y.; Liu, F.; Jia, N.; Gao, J.; Pang, X.; Deng, F. Diversiform etiologies for post-stroke depression. Front. Psychiatry 2019, 9, 761. [Google Scholar] [CrossRef]
- Ahn, D.H.; Lee, Y.J.; Jeong, J.H.; Kim, Y.R.; Park, J.B. The effect of post-stroke depression on rehabilitation outcome and the impact of caregiver type as a factor of post-stroke depression. Ann. Rehabil. Med. 2015, 39, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Qiu, X.; Miao, J.; Lan, Y.; Sun, W.; Chen, Y.; Cao, Z.; Li, G.; Zhao, X.; Zhu, Z.; Zhu, S. Association of Cerebral Artery Stenosis With Post-stroke Depression at Discharge and 3 Months After Ischemic Stroke Onset. Front. Psychiatry 2020, 25, 585201. [Google Scholar] [CrossRef]
- Tu, X.Q.; Lai, Z.H.; Zhang, Y.; Ding, K.Q.; Ma, F.Y.; Yang, G.Y.; He, J.R.; Zeng, L.L. Periventricular White Matter Hyperintensity in Males is Associated with Post-Stroke Depression Onset at 3 Months. Neuropsychiatr. Dis. Treat. 2021, 8, 1839–1857. [Google Scholar] [CrossRef]
- Zhang, Y.; He, J.R.; Liang, H.B.; Lu, W.J.; Yang, G.Y.; Liu, J.R.; Zeng, L.L. Diabetes mellitus is associated with late-onset post-stroke depression. J. Affect. Disord. 2017, 15, 222–226. [Google Scholar] [CrossRef]
- Wang, Z.; Zhu, M.; Su, Z.; Guan, B.; Wang, A.; Wang, Y.; Zhang, N.; Wang, C. Post-stroke depression: Different characteristics based on follow-up stage and gender-a cohort perspective study from Mainland China. Neurol. Res. 2017, 39, 996–1005. [Google Scholar] [CrossRef]
- Hackett, M.L.; Pickles, K. Part I: Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef]
- Wang, L.; Tao, Y.; Chen, Y.; Wang, H.; Zhou, H.; Fu, X. Association of post stroke depression with social factors, insomnia, and neurological status in Chinese elderly population. Neurol. Sci. 2016, 37, 1305–1310. [Google Scholar] [CrossRef]
- Wei, N.; Yong, W.; Li, X.; Zhou, Y.; Deng, M.; Zhu, H.; Jin, H. Post-stroke depression and lesion location: A systematic review. J. Neurol. 2015, 262, 81–90. [Google Scholar] [CrossRef]
- Medeiros, G.C.; Roy, D.; Kontos, N.; Beach, S.R. Post-stroke depression: A 2020 updated review. Gen. Hosp. Psychiatry 2020, 66, 70–80. [Google Scholar] [CrossRef]
- Robinson, R.G.; Jorge, R.E. Post-stroke depression: A review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef] [Green Version]
- Shan, D.; Zheng, Y.; Froud, K. Brain-derived neurotrophic factor as a clinical biomarker in predicting the development of post-stroke depression: A review of evidence. Cureus 2021, 13, e15662. [Google Scholar] [CrossRef]
- Herrmann, M.; Bartels, C.; Schumacher, M.; Wallesch, C.W. Poststroke depression. Is there a pathoanatomic correlate for depression in the postacute stage of stroke? Stroke 1995, 26, 850–856. [Google Scholar] [CrossRef]
- Aström, M.; Adolfsson, R.; Asplund, K. Major depression in stroke patients. A 3-year longitudinal study. Stroke 1993, 24, 976–982. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Yang, D.; Zeng, Y.; Wu, W. Risk factors for post-stroke depression: A meta-analysis. Front. Aging Neurosci. 2017, 9, 218. [Google Scholar] [CrossRef]
- De Ryck, A.; Brouns, R.; Geurden, M.; Elseviers, M.; de Deyn, P.P.; Engelborghs, S.S. Risk factors for poststroke depression: Identification of inconsistencies based on a systematic review. J. Geriatr. Psychiatry Neurol. 2014, 27, 147–158. [Google Scholar] [CrossRef]
- Parganiha, A.; Taj, S.; Chandel, P.; Sultan, A.; Choudhary, V. Effect of hospitalization on rest-activity rhythm and quality of life of cancer patients. Indian J. Exp. Biol. 2014, 52, 549–558. [Google Scholar]
- Sugawara, N.; Metoki, N.; Hagii, J.; Saito, S.; Shiroto, H.; Tomita, T.; Yasujima, M.; Okumura, K.; Yasui-Furukori, N. Effect of depressive symptoms on the length of hospital stay among patients hospitalized for acute stroke in Japan. Neuropsychiatr. Dis. Treat. 2015, 11, 2551–2556. [Google Scholar] [CrossRef] [Green Version]
- Hosaka, T.; Aoki, T.; Watanabe, T.; Okuyama, T.; Kurosawa, H. Comorbidity of depression among physically ill patients and its effect on the length of hospital stay. Psychiatry Clin. Neurosci. 1999, 53, 491–495. [Google Scholar] [CrossRef]
- Mumford, E.; Schlesinger, H.J.; Glass, G.V.; Patrick, C.; Cuerdon, T. A new look at evidence about reduced cost of medical utilization following mental health treatment. Am. J. Psychiatry 1984, 141, 1145–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strain, J.J.; Lyons, J.S.; Hammer, J.S.; Fahs, M.; Lebovits, A.; Paddison, P.L.; Snyder, S.; Strauss, E.; Burton, R.; Nuber, G.; et al. Cost offset from a psychiatric consultation-liaison intervention with elderly hip fracture patients. Am. J. Psychiatry 1991, 148, 1044–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Lee, E.J.; Chang, D.I.; Park, J.H.; Ahn, S.H.; Cha, J.K.; Heo, J.H.; Sohn, S.I.; Lee, B.C.; Kim, D.E.; et al. Efficacy of early administration of escitalopram on depressive and emotional symptoms and neurological dysfunction after stroke: A multicentre, double-blind, randomised, placebo-controlled study. Lancet Psychiatry 2017, 4, 33–41. [Google Scholar] [CrossRef]
- Ilut, S.; Stan, A.; Blesneag, A.; Vacaras, V.; Vesa, S.; Fodoreanu, L. Factors that influence the severity of post-stroke depression. J. Med. Life 2017, 10, 167–171. [Google Scholar]
- Mu, Y.; Wang, Z.; Zhou, J.; Tan, C.; Wang, H. Correlations of post-stroke depression with inflammatory response factors. Iran J. Public Health 2018, 47, 988–993. [Google Scholar]
- Li, G.; Miao, J.; Sun, W.; Song, X.; Lan, Y.; Zhao, X.; Qiu, X.; Zhang, C.; Zhu, Z.; Zhu, S. Lower serum uric acid is associated with post-stroke depression at discharge. Front. Psychiatry 2020, 18, 52. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | All (n = 227) | Post-Stroke Depression | p-Value | |
|---|---|---|---|---|
| Negative (n = 163) | Positive (n = 64) | |||
| Demographics | ||||
| Age (years) | 67.1 ± 12.4 | 68.2 ± 13.7 | 0.548 | |
| Sex, male (%) | 97 (59.5) | 30 (46.9) | 0.084 | |
| Body mass index (kg/m2) | 22.8 ± 4.8 | 23.9 ± 3.2 | 0.077 | |
| Cardiovascular risk | ||||
| Hypertension | 90 (55.2) | 35 (54.7) | 0.943 | |
| Diabetes mellitus | 66 (40.5) | 23 (35.9) | 0.527 | |
| Atrial fibrillation | 31 (19.0) | 9 (14.1) | 0.378 | |
| Dyslipidemia | 36 (22.1) | 16 (25.0) | 0.638 | |
| Previous stroke | 25 (15.3) | 8 (12.5) | 0.585 | |
| Previous ischemic heart disease | 13 (8.0) | 7 (10.9) | 0.479 | |
| Smoking | 38 (23.3) | 11 (17.2) | 0.313 | |
| Alcohol consumption | 43 (26.4) | 12 (18.8) | 0.227 | |
| TOAST classification | ||||
| Large-artery atherosclerosis | 39 (23.9) | 17 (26.6) | 0.587 | |
| Cardioembolism | 40 (24.5) | 19 (29.7) | ||
| Small-vessel occlusion | 28 (17.2) | 9 (14.1) | ||
| Stroke of undetermined etiology | 42 (25.8) | 17 (26.6) | ||
| Stroke of other determined etiology | 14 (8.6) | 2 (3.1) | ||
| Psychological test | ||||
| Onset to test (days) | 2.7 ± 1.7 | 2.6 ± 1.8 | 0.731 | |
| HDRS score at admission | 5.8 ± 4.3 | 13.6 ± 9.7 | <0.001 | |
| Hospitalization factors | ||||
| Onset to admission (h) | 13.7 ± 18.4 | 15.7 ± 20.3 | 0.468 | |
| Hospitalization period (days) | 7.8 ± 4.5 | 9.6 ± 4.9 | 0.010 | |
| Neurological severity | ||||
| Initial NIHSS score | 4.0 ± 4.4 | 5.4 ± 5.2 | 0.034 | |
| NIHSS score at discharge | 2.1 ± 2.2 | 5.5 ± 5.0 | <0.001 | |
| NIHSS score after 3 months | 1.2 ± 1.6 | 4.7 ± 5.1 | <0.001 | |
| Initial mRS | 2.0 ± 1.4 | 2.7 ± 1.6 | 0.004 | |
| mRS at discharge | 1.4 ± 1.2 | 2.7 ± 1.6 | <0.001 | |
| mRS after 3 months | 0.9 ± 1.1 | 2.3 ± 1.7 | <0.001 | |
| Laboratory findings | ||||
| White blood cells (103/µL) | 7.9 ± 3.5 | 8.2 ± 2.8 | 0.501 | |
| Hemoglobin (g/dL) | 14.0 ± 5.1 | 13.2 ± 2.0 | 0.222 | |
| Platelets (103/µL) | 244.4 ± 67.3 | 245.5 ± 60.6 | 0.905 | |
| Protein (g/dL) | 6.4 ± 0.5 | 6.5 ± 0.6 | 0.149 | |
| Albumin (g/dL) | 3.8 ± 0.4 | 3.8 ± 0.4 | 0.297 | |
| Aspartate transaminase (U/L) | 24.5 ± 13.9 | 25.3 ± 25.7 | 0.771 | |
| Alanine transaminase (U/L) | 21.1 ± 16.7 | 18.5 ± 11.3 | 0.262 | |
| Alkaline phosphatase (U/L) | 54.1 ± 14.9 | 58.7 ± 20.1 | 0.111 | |
| Glucose (mg/dL) | 103.1 ± 48.2 | 113.4 ± 51.0 | 0.157 | |
| Blood urea nitrogen (mg/dL) | 15.4 ± 8.7 | 16.6 ± 7.9 | 0.311 | |
| Creatinine (mg/dL) | 1.0 ± 0.8 | 1.0 ± 0.3 | 0.592 | |
| Total cholesterol (mg/dL) | 186.8 ± 159.6 | 180.0 ± 42.1 | 0.744 | |
| Triglycerides (mg/dL) | 118.3 ± 78.6 | 114.0 ± 88.2 | 0.722 | |
| Uric acid (mg/dL) | 6.1 ± 13.7 | 5.0 ± 2.3 | 0.526 | |
| High-density lipoprotein (mg/dL) | 43.2 ± 10.5 | 44.4 ± 11.5 | 0.435 | |
| Low-density lipoprotein (mg/dL) | 106.4 ± 37.0 | 113.8 ± 38.5 | 0.179 | |
| Calcium (mg/dL) | 8.7 ± 0.5 | 8.8 ± 0.4 | 0.376 | |
| Sodium (mEq/L) | 149.7 ± 125.4 | 140.8 ± 3.8 | 0.571 | |
| Potassium (mEq/L) | 4.0 ± 0.4 | 4.0 ± 0.4 | 0.534 | |
| Erythrocyte sedimentation rate (mm/h) | 13.9 ± 13.6 | 13.0 ± 13.7 | 0.664 | |
| High-sensitivity C-reactive protein (mg/dL) | 0.8 ± 1.4 | 1.4 ± 2.8 | 0.094 | |
| Thyroid stimulating hormone (μIU/mL) | 1.6 ± 1.4 | 1.6 ± 1.9 | 0.774 | |
| Free thyroxine (ng/dL) | 1.2 ± 0.3 | 1.2 ± 0.4 | 0.348 | |
| Glomerular filtration rate (mL/min) | 89.4 ± 27.1 | 91.3 ± 29.8 | 0.645 | |
| Variables | Univariate Analysis | Multivariate Analysis * | ||
|---|---|---|---|---|
| Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Sex | 0.60 (0.34–1.08) | 0.086 | ||
| BMI | 1.08 (0.99–1.17) | 0.079 | ||
| HDRS score at admission | 1.21 (1.14–1.29) | <0.001 | 1.22 (1.14–1.31) | <0.001 |
| Hospitalization period (days) | 1.08 (1.01–1.15) | 0.016 | 1.11 (1.02–1.20) | 0.013 |
| Initial NIHSS score | 1.07 (1.00–1.13) | 0.037 | ||
| hs-CRP | 1.16 (1.01–1.34) | 0.039 | ||
| Variables | All (n = 109) | Improvement of PSD | p-Value | |
|---|---|---|---|---|
| PSD-Relieved Group (n = 64) | PSD-Unrelieved Group (n = 45) | |||
| Demographics | ||||
| Age (years) | 69.1 ± 12.2 | 68.8 ± 12.1 | 0.899 | |
| Sex, male (%) | 36 (56.3) | 20 (44.4) | 0.225 | |
| Body mass index (kg/m2) | 23.1 ± 3.0 | 23.5 ± 3.2 | 0.488 | |
| Cardiovascular risk | ||||
| Hypertension | 32 (50.0) | 25 (55.6) | 0.567 | |
| Diabetes mellitus | 24 (37.5) | 20 (44.4) | 0.467 | |
| Atrial fibrillation | 9 (14.1) | 8 (17.8) | 0.599 | |
| Dyslipidemia | 16 (25.0) | 12 (26.7) | 0.845 | |
| Previous stroke | 11 (17.2) | 3 (6.7) | 0.148 | |
| Previous ischemic heart disease | 4 (6.3) | 5 (11.1) | 0.484 | |
| Smoking | 15 (23.4) | 7 (15.6) | 0.313 | |
| Alcohol consumption | 15 (23.4) | 7 (15.6) | 0.313 | |
| TOAST classification | ||||
| Large-artery atherosclerosis | 16 (25.0) | 10 (22.2) | 0.941 | |
| Cardioembolism | 15 (23.4) | 11 (24.4) | ||
| Small-vessel occlusion | 8 (12.5) | 8 (17.8) | ||
| Stroke of undetermined etiology | 21 (32.8) | 14 (31.1) | ||
| Stroke of other determined etiology | 4 (6.3) | 2 (4.4) | ||
| Psychological test | ||||
| Onset to test (days) | 2.8 ± 1.9 | 2.5 ± 1.9 | 0.515 | |
| HDRS score at admission | 10.2 ± 3.4 | 17.6 ± 8.9 | <0.001 | |
| Hospitalization factors | ||||
| Onset to admission (h) | 13.4 ± 15.4 | 15.1 ± 17.3 | 0.593 | |
| Hospitalization period (days) | 7.9 ± 4.3 | 9.4 ± 4.2 | 0.070 | |
| Neurological severity | ||||
| Initial NIHSS score | 4.3 ± 4.2 | 6.2 ± 5.8 | 0.072 | |
| NIHSS score at discharge | 2.2 ± 2.3 | 5.8 ± 5.1 | <0.001 | |
| NIHSS score after 3 months | 1.4 ± 1.8 | 4.8 ± 5.3 | <0.001 | |
| Initial mRS | 2.3 ± 1.5 | 2.7 ± 1.7 | 0.124 | |
| mRS at discharge | 1.6 ± 1.2 | 2.7 ± 1.6 | <0.001 | |
| mRS after 3 months | 1.0 ± 1.1 | 2.2 ± 1.8 | <0.001 | |
| Laboratory findings | ||||
| White blood cells (103/µL) | 8.5 ± 4.6 | 8.3 ± 2.8 | 0.885 | |
| Hemoglobin (g/dL) | 13.1 ± 1.9 | 13.2 ± 2.0 | 0.784 | |
| Platelets (103/µL) | 249.8 ± 71.0 | 254.2 ± 59.4 | 0.727 | |
| Protein (g/dL) | 6.4 ± 0.5 | 6.5 ± 0.6 | 0.371 | |
| Albumin (g/dL) | 3.8 ± 0.5 | 3.8 ± 0.4 | 0.547 | |
| Aspartate transaminase (U/L) | 24.6 ± 13.0 | 26.2 ± 30.0 | 0.694 | |
| Alanine transaminase (U/L) | 20.4 ± 16.1 | 18.7 ± 11.1 | 0.538 | |
| Alkaline phosphatase (U/L) | 54.8 ± 15.4 | 58.4 ± 19.6 | 0.297 | |
| Glucose (mg/dL) | 96.1 ± 32.0 | 117.4 ± 51.8 | 0.009 | |
| Blood urea nitrogen (mg/dL) | 14.2 ± 4.3 | 16.9 ± 8.8 | 0.037 | |
| Creatinine (mg/dL) | 0.9 ± 0.3 | 1.0 ± 0.4 | 0.713 | |
| Total cholesterol (mg/dL) | 172.8 ± 45.4 | 182.2 ± 41.0 | 0.275 | |
| Triglycerides (mg/dL) | 123.5 ± 98.1 | 116.6 ± 93.7 | 0.717 | |
| Uric acid (mg/dL) | 5.1 ± 1.6 | 4.9 ± 2.5 | 0.696 | |
| High-density lipoprotein (mg/dL) | 43.9 ± 11.3 | 44.3 ± 11.4 | 0.859 | |
| Low-density lipoprotein (mg/dL) | 105.6 ± 41.8 | 113.0 ± 36.9 | 0.342 | |
| Calcium (mg/dL) | 8.7 ± 0.5 | 8.8 ± 0.5 | 0.189 | |
| Sodium (mEq/L) | 164.9 ± 200.0 | 140.7 ± 3.7 | 0.419 | |
| Potassium (mEq/L) | 3.9 ± 0.3 | 4.0 ± 0.5 | 0.198 | |
| Erythrocyte sedimentation rate (mm/h) | 16.9 ± 17.1 | 12.8 ± 12.6 | 0.190 | |
| High-sensitivity C-reactive protein (mg/dL) | 0.9 ± 1.6 | 1.8 ± 3.2 | 0.096 | |
| Thyroid stimulating hormone (μIU/mL) | 1.4 ± 1.1 | 1.4 ± 1.2 | 0.992 | |
| Free thyroxine (ng/dL) | 1.2 ± 0.4 | 1.3 ± 0.5 | 0.362 | |
| Glomerular filtration rate (mL/min) | 91.9 ± 30.0 | 91.1 ± 30.0 | 0.894 | |
| Variables | Univariate Analysis | Multivariate Analysis * | ||
|---|---|---|---|---|
| Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| NIHSS score at discharge | 0.77 (0.67–0.88) | <0.001 | 0.80 (0.68–0.94) | 0.006 |
| Hospitalization period (days) | 1.09 (0.99–1.20) | 0.080 | ||
| HDRS score at admission | 0.77 (0.68–0.86) | <0.001 | 0.80 (0.71–0.89) | <0.001 |
| Glucose | 1.01 (1.00–1.02) | 0.017 | ||
| BUN | 1.08 (1.00–1.16) | 0.060 | ||
| hs-CRP | 1.17 (0.98–1.39) | 0.078 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-H.; Jeon, S.H.; Kim, M.J.; Ra, G.D.; Lee, Y.-H.; Hong, S.H.; Shin, B.-S.; Kang, H.G. Factors Affecting Post-Stroke Depression in Acute Ischemic Stroke Patients after 3 Months. J. Pers. Med. 2021, 11, 1178. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111178
Lee C-H, Jeon SH, Kim MJ, Ra GD, Lee Y-H, Hong SH, Shin B-S, Kang HG. Factors Affecting Post-Stroke Depression in Acute Ischemic Stroke Patients after 3 Months. Journal of Personalized Medicine. 2021; 11(11):1178. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111178
Chicago/Turabian StyleLee, Chan-Hyuk, Su Hong Jeon, Min Ju Kim, Gyu Dam Ra, Yong-Hyun Lee, Seung Hyeon Hong, Byoung-Soo Shin, and Hyun Goo Kang. 2021. "Factors Affecting Post-Stroke Depression in Acute Ischemic Stroke Patients after 3 Months" Journal of Personalized Medicine 11, no. 11: 1178. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11111178