
Identifying Barriers and Facilitators to Diet and Physical Activity Behaviour Change in Type 2 Diabetes Using a Design Probe Methodology

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
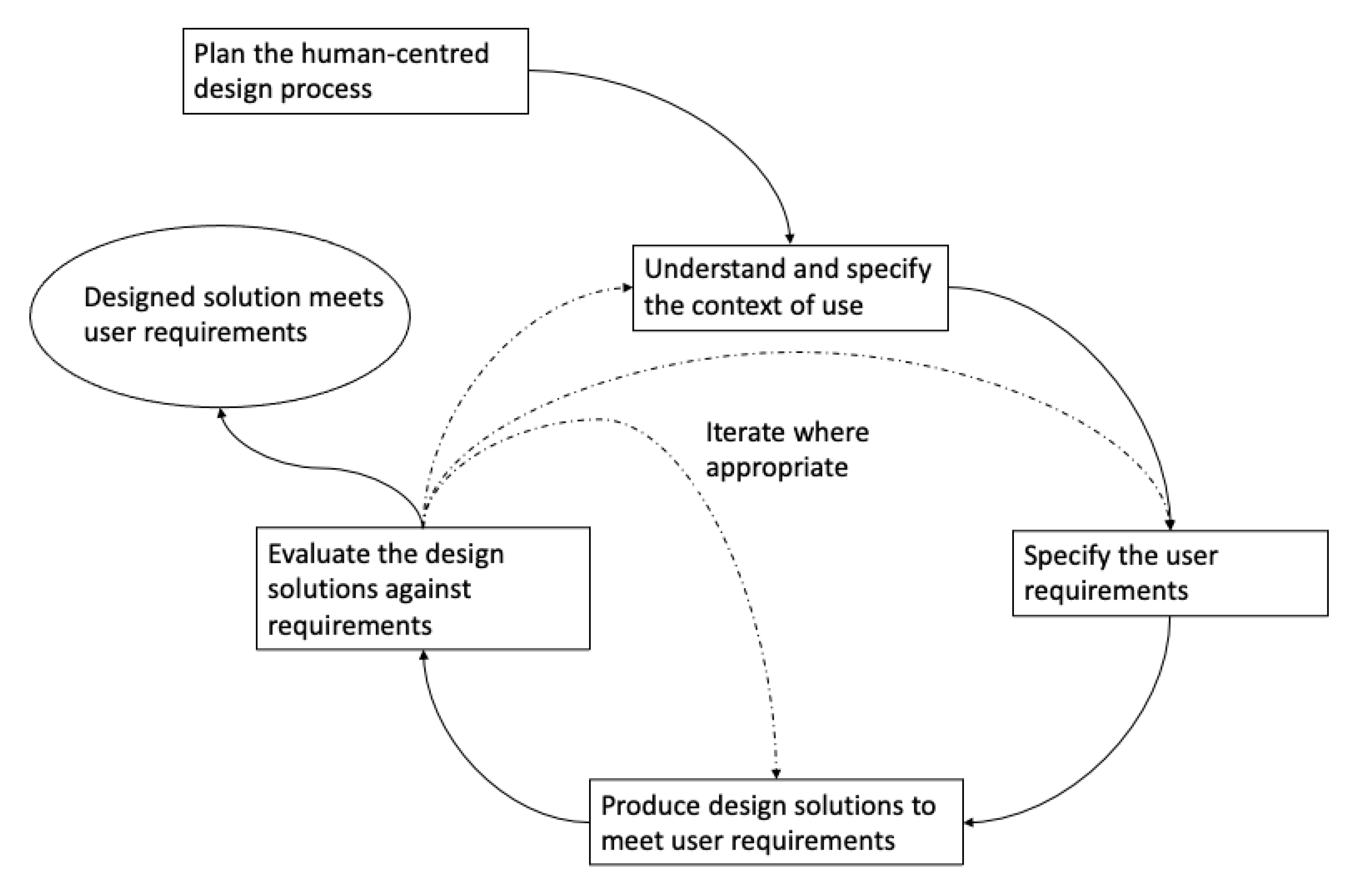
- requires an explicit understanding of users, tasks, and environments
- has users involved throughout the design and development process
- is driven and refined through user-centred evaluation
- is an iterative process
- addresses the whole user experience
- involves a design team with multidisciplinary skills and perspectives
- Design Probes allows the participant to interact with them on a daily basis in their own time and space, reflecting on their lived experience and capturing that reflection by adding content to the probe each day [16].
- A Design Probe is an exploratory method that does not conform to traditional ethnographic methods but is capable of yielding rich insights [17], perhaps unattainable by other established methods.
2. Materials and Methods
2.1. Recruitment/Subjects
2.2. Design Probe Design Philosophy
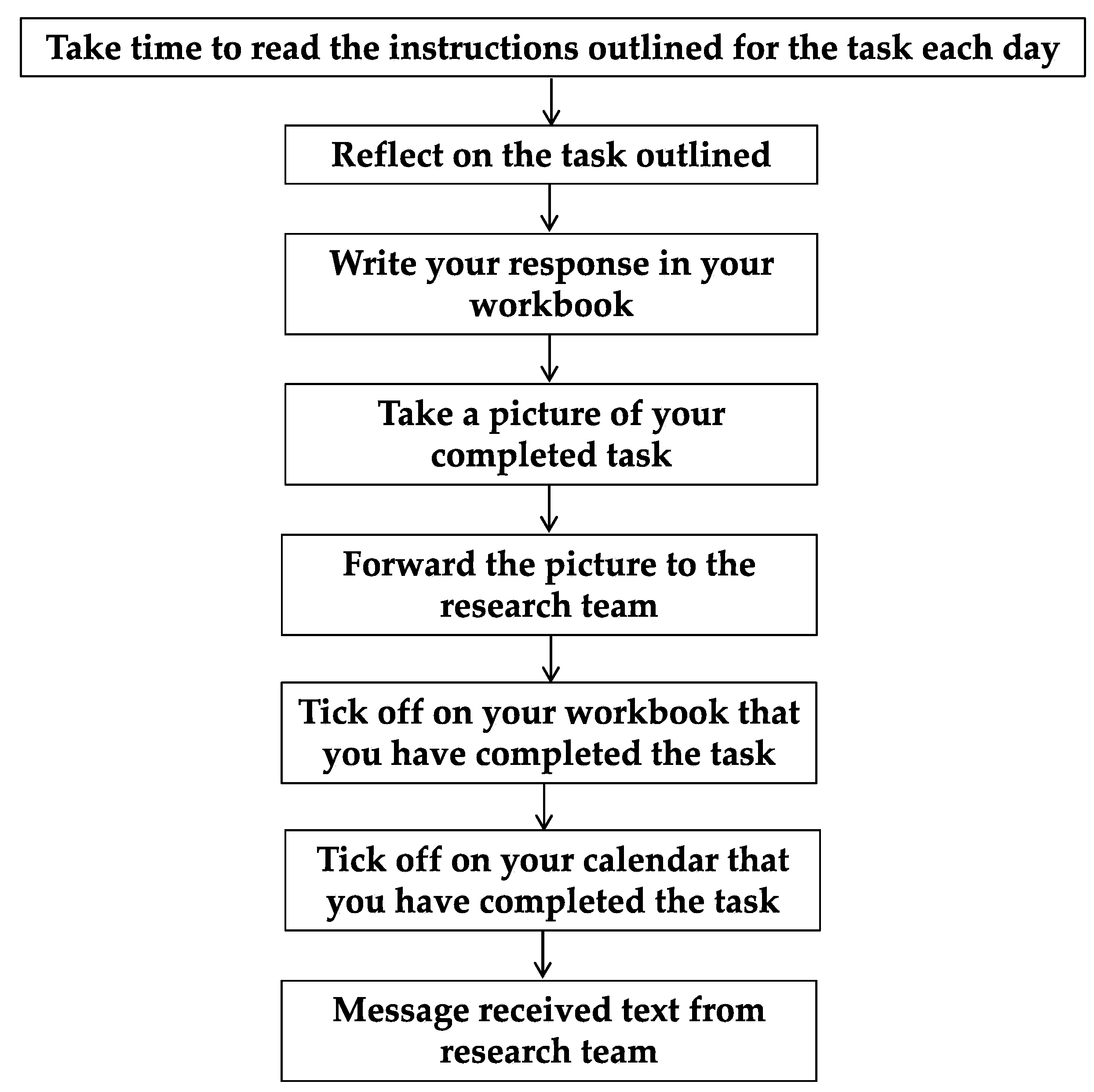
2.3. Design Probe Process
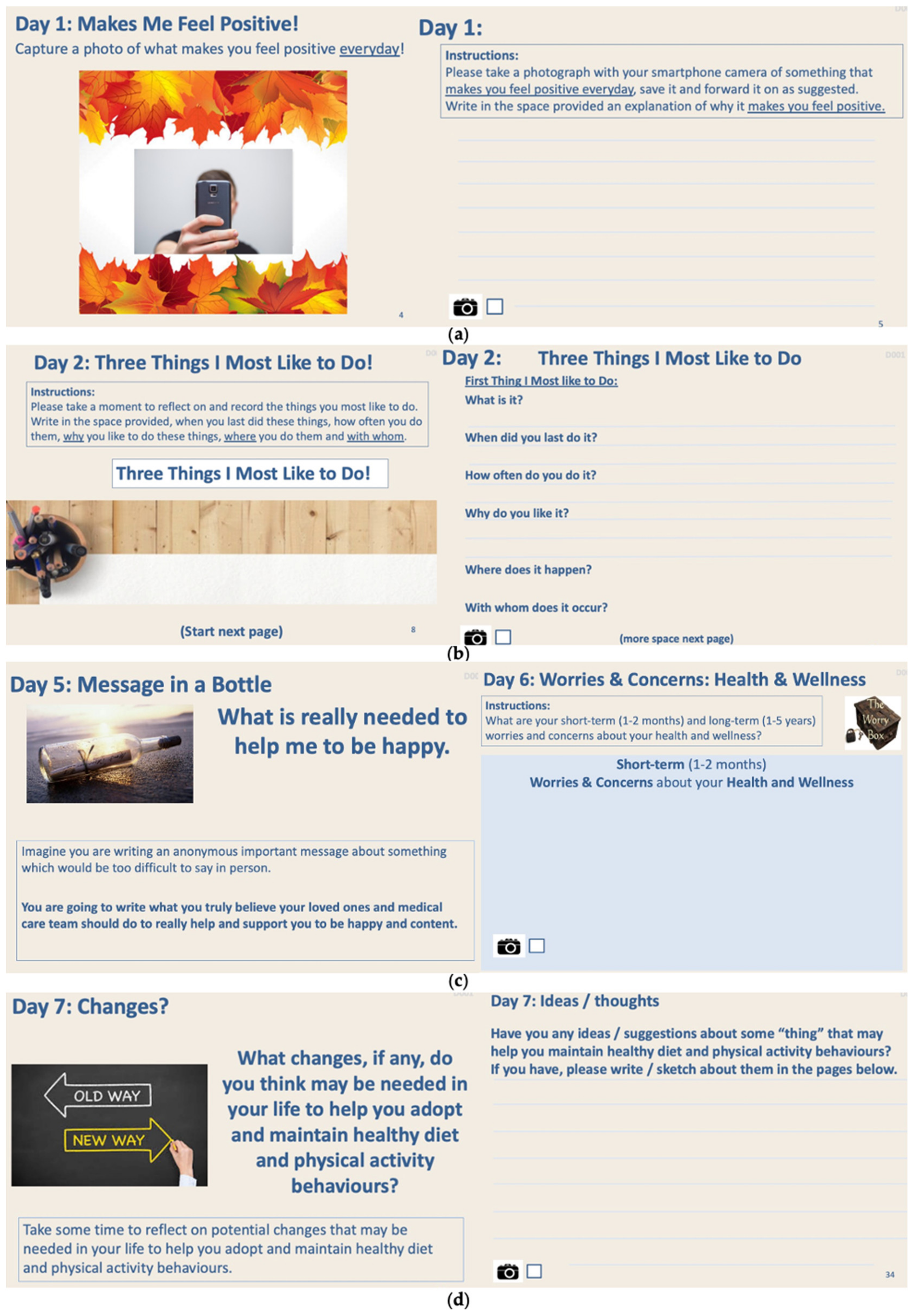
2.4. Design Probe Design
- something that “makes me feel” positive and something that “makes me feel” negative in photo-based tasks (Day 1)
- three things participants most like to do and the context in which those things occur (Day 2)
- three things participants least like to do and the context in which those things occur (Day 3)
- examples of where the participants believe that they were/are not being listened to; (Day 4)
- write an anonymous message in a bottle about what is really needed to make me happy written to both loved ones and to their medical care team (Day 5)
- short-term and long-term health and wellness hopes/dreams and worries/concerns; (Day 6)
- changes needed in my life to help adopt healthy diet and physical activity behaviours (Day 7)
- ideas to maintain healthy diet and physical activity behaviours (Days 7–28)
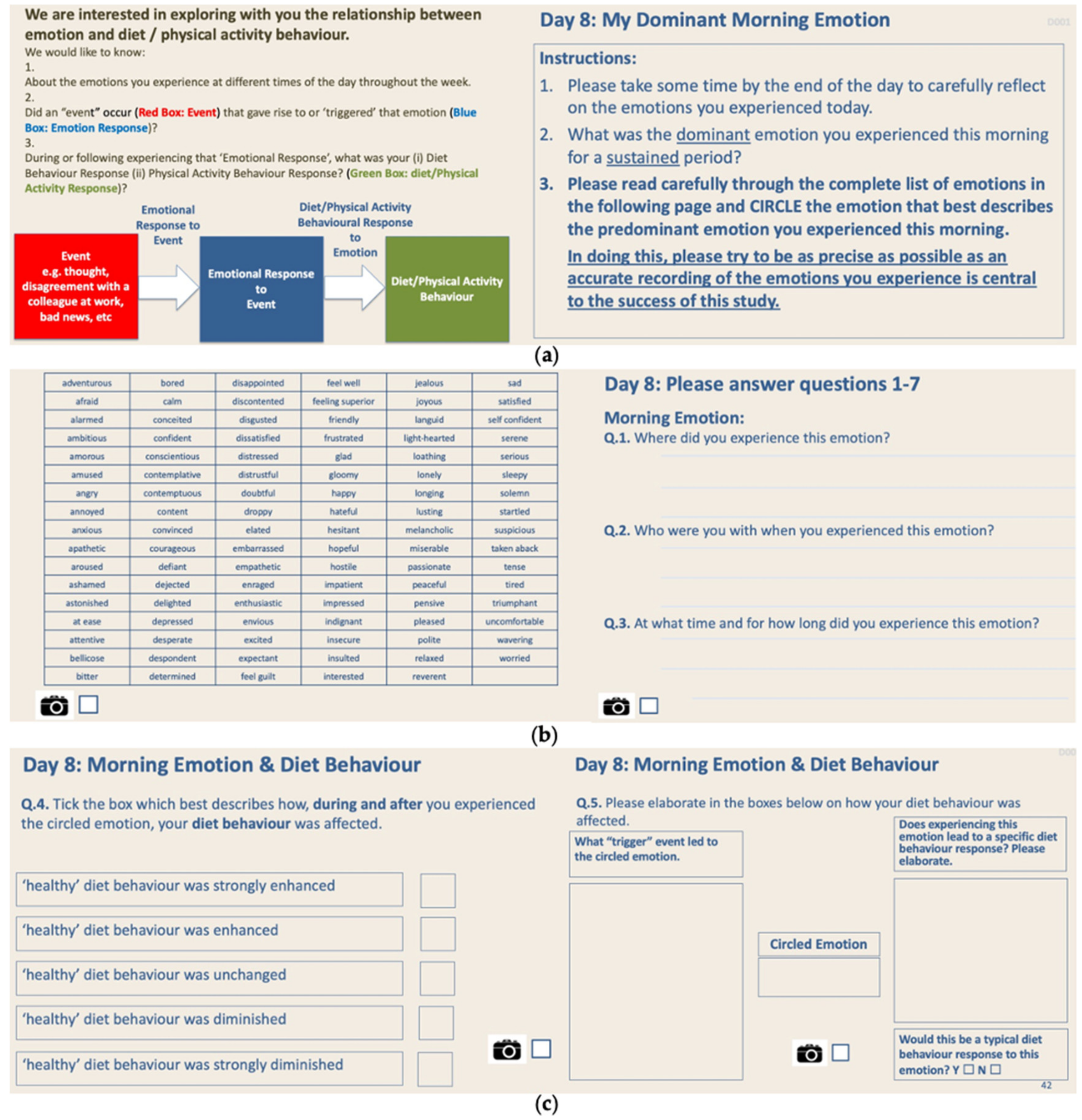
- reflection and sensitisation of the participants to the inter-connection between emotions they experienced, the context in which those emotions occurred, how those emotions might have influenced their diet behaviours and how those emotions might have influenced their physical activity behaviours and what were the trigger events that may have triggered those emotions; this process was repeated for 7 days of dominant morning emotions, 7 days of dominant afternoon emotions and 7 days of dominant evening emotions; (Days 8–14 morning, Days 15–21 afternoon, Days 22–28 evening)
- barriers to diet behaviour change—what is it, when did it occur, where did it occur, who did it occur with (Day 29)
- barriers to physical activity behaviour change—what is it, when did it occur, where did it occur, who did it occur with (Day 29)
- facilitators to diet behaviour change—what is it, when did it occur, where did it occur, who did it occur with (Day 30)
- facilitators to physical activity behaviour change—what is it, when did it occur, where did it occur, who did it occur with (Day 30)
- best ideas from those generated over Days 7–28
2.5. Data Analysis
- Familiarising yourself with the data and identifying items of potential interest
- Generating codes
- Generating initial themes
- Reviewing initial themes
- Defining and naming themes
3. Results
Barriers to Healthy Diet Behaviours
- Food environment
- Mental health
- Work schedule
- Planning
- Social support
- Cravings
- Economic circumstances
- Energy
Facilitators to Healthy Diet Behaviours
- Planning
- Food environment
- Social support
- Economic circumstances
Barriers to Healthy Physical Activity Behaviours
- Physical health *
- Mental health
- Social support
- Motivation *
- Energy
- Weather *
- Work schedule
- Physical environment *
- Economic circumstances
Facilitators to Healthy Physical Activity Behaviours
- Social support
- Planning
- Mental health
- Physical health
- Motivation
- Physical environment
- Weather
- Economic circumstances
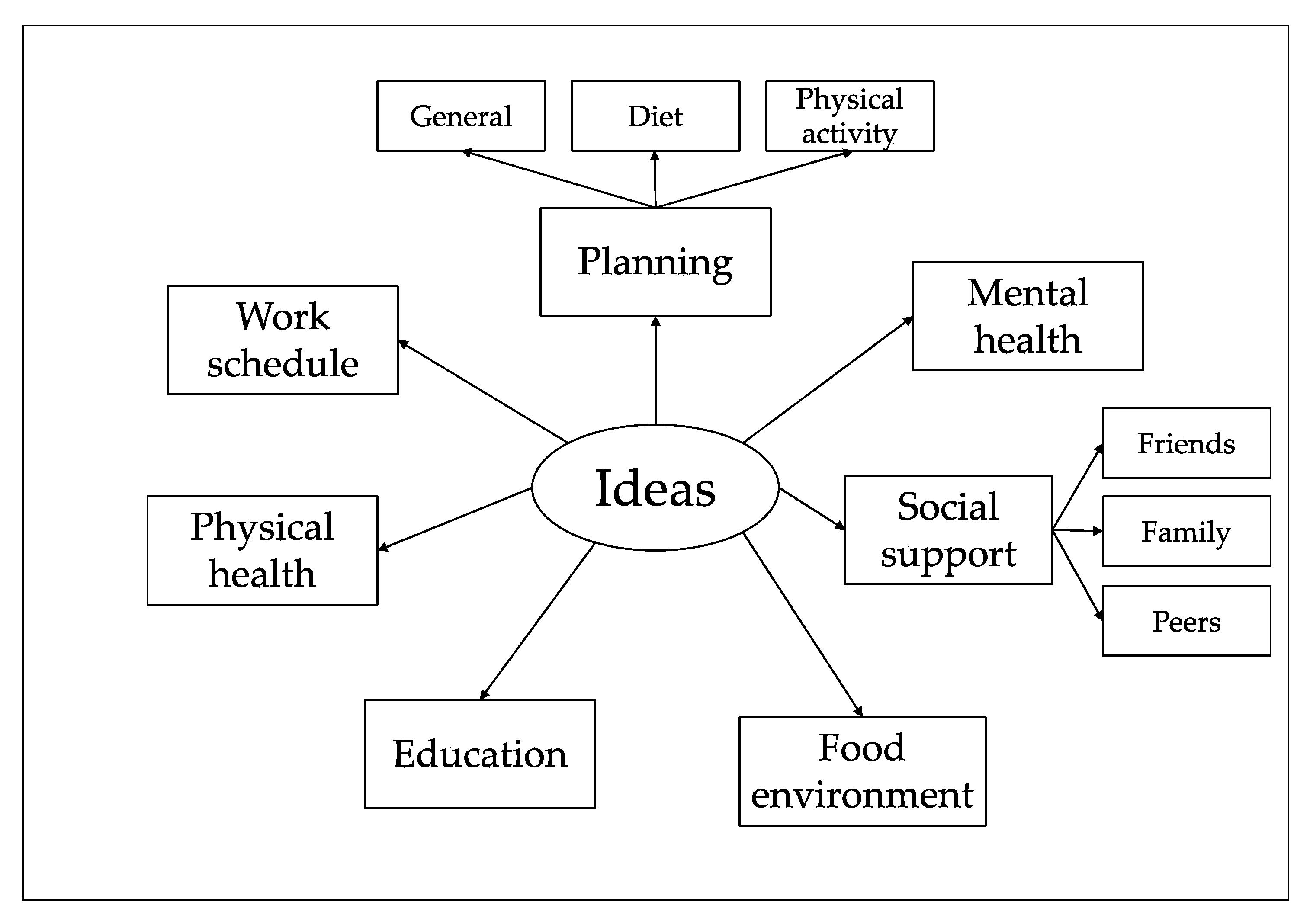
Best Ideas
- Planning
- Mental health
- Social support
- Food environment
- Education *
- Physical health
- Work schedule
Food Environment
“When I shop for groceries, the ‘non-healthy’ foods are very tempting to buy…I have to make a special effort not to buy such foods”P9 (F)
“supermarket…availability of healthy foods…easier to make better decisions”P11 (F)
“At home…I’m more likely to eat carbs in the form of bread”P4 (F)
“being organised & having healthy eating choices in my house”P9 (F)
“people around me eating sweet things…I get tempted to eat/overeat this kind of food”P9 (F)
“In our local café…availability of healthy food”P11 (F)
“I spend all summer on the road which leads to ‘grazing’ on the go”P2 (M)
“finding quick ways to bring good food to work”P4 (F)
“remove ‘unhealthy’ food from my house to reduce the ‘temptation’…having alternatives to snack on/make my meals from”P9 (F)
“When on the road, don’t rely on service stations…take packed lunches”P2 (M)
Mental Health
“Depression, leads to complete self-neglect and loss of energy”P6 (M)
“stress, or worry, when I feel stressed…I turn to food for comfort…I eat in secret”P9 (F)
“my size makes me embarrassed so I don’t go swimming which I love”P4 (F)
“if house happy, I am more likely to do more exercise”P3 (F)
“behave and act much more positively”P13 (M)
“Try to keep as stress free as possible”P10 (F)
Work Schedule
“my hours are not set…hard to plan”P1 (M)
“leave home 5–6 a.m. and return 6–8 p.m.…leaves little time for any real physical activity”P2 (M)
“make work fit around my life and not the other way around”P13 (M)
Planning
“Not eating regularly, I tend to miss meals and then I overeat”P3 (F)
“being organised & having healthy eating choices in my house, helps me make healthy eating choices”P9 (F)
“Planning what to eat and shopping accordingly (in advance) rather than relying on picking something up last minute”P2 (M)
“When going out to eat, choosing a venue with healthy eating choice...I can enjoy a meal out”P9 (F)
“hours are not set…hard to plan”P1 (M)
“finding quick ways to bring good food to work”P4 (F)
“having a routine—a set time every-day to go for a walk…I don’t plan anything else for that time”P9 (F)
“Following a plan or schedule, taking the thinking out of it, something to follow and become routine.”P12 (F)
“Being organised & planning healthy meals in advance…by reducing / eliminating impulse eating of non-healthy foods/meals”P9 (F)
“Try to make time for some activity every day”P2 (M)
Social Support
“friends, industry colleagues, social life: i.e., eating away from home…usually involve rich hotel foods”P2 (M)
“Wife, she’s always willing me to better myself”P1 (M)
“having a ‘buddy’ to go for a walk with, I feel I would be much more likely to exercise”P9 (F)
“a friend helps me keep focused, keeps me motivated”P9 (F)
“re-join my Slimming World group, will help me to maintain a healthy eating & physically active lifestyle”P9 (F)
Diet Cravings
“When I have the munchies…I crave chocolate and crisps”P11 (F)
Economic Circumstances
“fresh food…especially can be expensive”P10 (F)
“If I do not have enough money, I tend to eat junk food”P5 (F)
“a job… provides money to be able to buy better food”P6 (M)
“without money I am unable to pay for the gym”P6 (M)
“A job… forces me in another rhythm and provides money for the gym”P6 (M)
Energy
“tiredness… don’t seem to have the energy after a long day at work”P1 (M)
“If I am too tired, I do not feel like exercising”P5 (F)
Physical Health
“arthritis…I am not able to walk very far without pain”P4 (F)
“With the weight off, I have more energy, doing more”P11 (F)
“Swimming causes no pain on my feet…I’m a very good swimmer…just have to stop being embarrassed about my weight but the more weight I lose the easier that will be”P4 (F)
Motivation
“Motivation/commitment: I always give up, I don’t know why”P13 (M)
“Signing up for charity walks…makes me get out and train”P1 (M)
Weather
“Weather… it’s a barrier to most of the physical activities I do”P2 (M)
“fine weather makes me more adventurous…my physical activity is weather dependent”P2 (M)
Physical Environment
“I am afraid of tripping or falling when I go for a walk”P3 (F)
“Lack of garden…gardening brings me out of the house”P6 (M)
“Garden Allotment…gardening provides healthy exercise”P6 (M)
Education
“do the 10 week course with CROI, I learnt so much from that”P1 (M)
“re-join my Slimming World group…will help me to maintain a healthy eating & physical activity lifestyle”P9 (F)
4. Discussion
4.1. Design Ideas
4.2. Empathy for Design
4.3. Strengths and Limitations
4.4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Cradock, K.A.; ÓLaighin, G.; Finucane, F.M.; Gainforth, H.L.; Quinlan, L.R.; Martin Ginis, K.A. Behaviour change techniques targeting both diet and physical activity in type 2 diabetes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young-Hyman, D.; De Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial care for people with diabetes: A position statement of the American diabetes association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; Alkandari, J.R.; Andersen, L.B.; Blair, S.N.; Brownson, R.C.; et al. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Goldney, R.D.; Phillips, P.J.; Fisher, L.J.; Wilson, D.H. Diabetes, Depression, and Quality of Life: A population study. Diabetes Care 2004, 27, 1066–1070. [Google Scholar] [CrossRef] [Green Version]
- Lustig, R.H. The neuroendocrinology of childhood obesity. Pediatr. Clin. N. Am. 2001, 48, 909–930. [Google Scholar] [CrossRef]
- Hankonen, N.; Sutton, S.; Prevost, A.T.; Simmons, R.K.; Griffin, S.J.; Kinmonth, A.L.; Hardeman, W. Which Behavior Change Techniques are Associated with Changes in Physical Activity, Diet and Body Mass Index in People with Recently Diagnosed Diabetes? Ann. Behav. Med. 2015, 49, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Avery, L.; Flynn, D.; Van Wersch, A.; Sniehotta, F.F.; Trenell, M.I. Changing physical activity behavior in type 2 diabetes: A systematic review and meta-analysis of behavioral interventions. Diabetes Care 2012, 35, 2681–2689. [Google Scholar] [CrossRef] [Green Version]
- Cradock, K.A.; ÓLaighin, G.; Finucane, F.M.; McKay, R.; Quinlan, L.R.; Martin Ginis, K.A.; Gainforth, H.L. Diet behavior change techniques in type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2017, 40, 1800–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DIS. 9241-210: 2010. Ergonomics of Human System Interaction-Part. 210: Human-Centred Design for Interactive Systems (Formerly Known as 13407); International Standardization Organization (ISO): Geneva, Switzerland, 2010. [Google Scholar]
- Norman, D.A.; Draper, S.W. User Centered System Design; New Perspectives on Human-Computer Interaction; L. Erlbaum Associates Inc.: Mahwah, NJ, USA, 1986. [Google Scholar]
- Kouprie, M.; Visser, F.S. A framework for empathy in design: Stepping into and out of the user’s life. J. Eng. Des. 2009, 20, 437–448. [Google Scholar] [CrossRef]
- Van Boeijen, A.; Daalhuizen, J.; Zijlstra, J.; Schoor, R.V.D. Delft Design Guide: Design Methods; BIS Publishers: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Mattelmäki, T. Design Probes; Publication Series of the University of Art and Design Helsinki A, 69/2006; Aalto University: Espoo, Finland, 2006. [Google Scholar]
- Gaver, B.; Dunne, T.; Pacenti, E. Design: Cultural probes. Interactions 1999, 6, 21–29. [Google Scholar] [CrossRef]
- Mattelmäki, T. Probing for co-exploring. CoDesign 2008, 4, 65–78. [Google Scholar] [CrossRef]
- Sanders, E.B.N.; Stappers, P.J. Probes, toolkits and prototypes: Three approaches to making in codesigning. CoDesign 2014, 10, 5–14. [Google Scholar] [CrossRef]
- Boehner, K.; Vertesi, J.; Sengers, P.; Dourish, P. How HCI interprets the probes. In Proceedings of the Conference on Human Factors in Computing Systems, San Jose, CA, USA, 28 April–3 May 2007; pp. 1077–1086. [Google Scholar] [CrossRef]
- Crabtree, A.; Hemmings, T.; Rodden, T.; Cheverst, K.; Clarke, K.; Dewsbury, G.; Hughes, J.; Rouncefield, M. Designing with care: Adapting cultural probes to inform design in sensitive settings. In Proceedings of the 2004 Australasian Conference on Computer-Human Interaction (OZCHI2004), Wollongong, Australia, 20–24 November 2004; pp. 4–13. [Google Scholar]
- Virtanen, K.; Mattelmäki, T.; Heinonen, S. Visiting eWorkers’ Homes-Three Stories for Designing eWork Homes and Furniture. In Proceedings of the 14th Annual Conference the eChallenges–e-2004, Berlin, Germany, 9–11 September 2004; pp. 27–29. [Google Scholar]
- Wherton, J.; Sugarhood, P.; Procter, R.; Rouncefield, M.; Dewsbury, G.; Hinder, S.; Greenhalgh, T. Designing assisted living technologies ‘in the wild’: Preliminary experiences with cultural probe methodology. BMC Med. Res. Methodol. 2012, 12, 188. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Crowe, C.; Gibson, I.; Cunningham, K.; Kerins, C.; Costello, C.; Windle, J.; O’Shea, P.M.; Hynes, M.; McGuire, B.; Kilkelly, K.; et al. Effects of an eight-week supervised, structured lifestyle modification programme on anthropometric, metabolic and cardiovascular risk factors in severely obese adults. BMC Endocr. Disord. 2015, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bernardini, C.; Ambrogi, V.; Fardella, G.; Perioli, L.; Grandolini, G. How to improve the readability of the patient package leaflet: A survey on the use of colour, print size and layout. Pharmacol. Res. 2001, 43, 437–443. [Google Scholar] [CrossRef]
- Scherer, K.R. What are emotions? and how can they be measured? Soc. Sci. Inf. 2005, 44, 695–729. [Google Scholar] [CrossRef]
- Visser, F.S.; Stappers, P.J.; van der Lugt, R.; Sanders, E.B.N. Contextmapping: Experiences from practice. CoDesign 2005, 1, 119–149. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis:Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16. [Google Scholar] [CrossRef]
- Fereday, J.; Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- Cheng, L.; Leung, D.Y.P.; Sit, J.W.H.; Li, X.M.; Wu, Y.N.; Yang, M.Y.; Gao, C.X.; Hui, R. Factors associated with diet barriers in patients with poorly controlled type 2 diabetes. Patient Prefer. Adherence 2016, 10, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Sohal, T.; Sohal, P.; King-Shier, K.M.; Khan, N.A. Barriers and facilitators for type-2 diabetes management in south asians: A systematic review. PLoS ONE 2015, 10, e0136202. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.J.; Wu, V.X.; Dawkes, S.; Lim, S.T.; Wang, W. Factors influencing diet barriers among outpatients with poorly-controlled type 2 diabetes: A descriptive correlational study. Nurs. Health Sci. 2019, 21, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Halali, F.; Mahdavi, R.; Mobasseri, M.; Asghari Jafarabadi, M.; Karimi Avval, S. Perceived barriers to recommended dietary adherence in patients with type 2 diabetes in Iran. Eat. Behav. 2016, 21, 205–210. [Google Scholar] [CrossRef]
- Marcy, T.R.; Britton, M.L.; Harrison, D. Identification of barriers to appropriate dietary behavior in low-income patients with type 2 diabetes mellitus. Diabetes Ther. 2011, 2, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, L.K.; Parchman, M.L.; Shepherd, M.D. Family support and diet barriers among older hispanic adults with type 2 diabetes. Fam. Med. 2004, 36, 423–430. [Google Scholar] [PubMed]
- Vijan, S.; Stuart, N.S.; Fitzgerald, J.T.; Ronis, D.L.; Hayward, R.A.; Slater, S.; Hofer, T.P. Barriers to following dietary recommendations in Type 2 diabetes. Diabet. Med. 2005, 22, 32–38. [Google Scholar] [CrossRef]
- Laranjo, L.; Neves, A.L.; Costa, A.; Ribeiro, R.T.; Couto, L.; Sá, A.B. Facilitators, barriers and expectations in the self-management of type 2 diabetes-A qualitative study from Portugal. Eur. J. Gen. Pract. 2015, 21, 103–110. [Google Scholar] [CrossRef]
- Booth, A.O.; Lowis, C.; Dean, M.; Hunter, S.J.; McKinley, M.C. Diet and physical activity in the self-management of type 2 diabetes: Barriers and facilitators identified by patients and health professionals. Prim. Health Care Res. Dev. 2013, 14, 293–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, R.; Gucciardi, E.; De Melo, M.; Barata, P. Self-management experiences among men and women with type 2 diabetes mellitus: A qualitative analysis. BMC Fam. Pract. 2012, 13, 122. [Google Scholar] [CrossRef] [Green Version]
- Korkiakangas, E.E.; Alahuhta, M.A.; Laitinen, J.H. Barriers to regular exercise among adults at high risk or diagnosed with type 2 diabetes: A systematic review. Health Promot. Int. 2009, 24, 416–427. [Google Scholar] [CrossRef] [Green Version]
- Lidegaard, L.P.; Schwennesen, N.; Willaing, I.; Færch, K. Barriers to and motivators for physical activity among people with Type 2 diabetes: Patients’ perspectives. Diabet. Med. 2016, 33, 1677–1685. [Google Scholar] [CrossRef]
- Mier, N.; Medina, A.A.; Ory, M.G. Mexican Americans with type 2 diabetes: Perspectives on definitions, motivators, and programs of physical activity. Prev. Chronic Dis. 2007, 4, A24. [Google Scholar]
- Casey, D.; De Civita, M.; Dasgupta, K. Understanding physical activity facilitators and barriers during and following a supervised exercise programme in Type 2 diabetes: A qualitative study. Diabet. Med. 2010, 27, 79–84. [Google Scholar] [CrossRef]
- Dutton, G.R.; Johnson, J.; Whitehead, D.; Bodenlos, J.S.; Brantley, P.J. Barriers to physical activity among predominantly low-income African-American patients with type 2 diabetes. Diabetes Care 2005, 28, 1209–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egan, A.M.; Mahmood, W.A.W.; Fenton, R.; Redziniak, N.; Kyaw Tun, T.; Sreenan, S.; McDermott, J.H. Barriers to exercise in obese patients with type 2 diabetes. QJM 2013, 106, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Al-Kaabi, J.; Al-Maskari, F.; Saadi, H.; Afandi, B.; Parkar, H.; Nagelkerke, N. Physical activity and reported barriers to activity among type 2 diabetic patients in the United Arab Emirates. Rev. Diabet. Stud. 2009, 6, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljasem, L.I.; Peyrot, M.; Wissow, L.; Rubin, R.R. The Impact of Barriers and Self-Efficacy on Self-Care Behaviors in Type 2 Diabetes. Diabetes Educ. 2001, 27, 393–404. [Google Scholar] [CrossRef]
- Yeh, M.C.; Ickes, S.B.; Lowenstein, L.M.; Shuval, K.; Ammerman, A.S.; Farris, R.; Katz, D.L. Understanding barriers and facilitators of fruit and vegetable consumption among a diverse multi-ethnic population in the USA. Health Promot. Int. 2008, 23, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Lawton, J.; Ahmad, N.; Hanna, L.; Douglas, M.; Hallowell, N. ‘I can’t do any serious exercise’: Barriers to physical activity amongst people of Pakistani and Indian origin with Type 2 diabetes. Health Educ. Res. 2006, 21, 43–54. [Google Scholar] [CrossRef]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- Glanz, K.; Basil, M.; Maibach, E.; Goldberg, J.; Snyder, D. Why Americans eat what they do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J. Am. Diet. Assoc. 1998, 98, 1118–1126. [Google Scholar] [CrossRef]
- Hall, K.D. Did the Food Environment Cause the Obesity Epidemic? Obesity 2018, 26, 11–13. [Google Scholar] [CrossRef]
- Harris, J.L.; Bargh, J.A.; Brownell, K.D. Priming Effects of Television Food Advertising on Eating Behavior. Health Psychol. 2009, 28, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Döbler, A.; Belnap, B.H.; Pollmann, H.; Farin, E.; Raspe, H.; Mittag, O. Telephone-delivered lifestyle support with action planning and motivational interviewing techniques to improve rehabilitation outcomes. Rehabil. Psychol. 2018, 63, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Olander, E.K.; Fletcher, H.; Williams, S.; Atkinson, L.; Turner, A.; French, D.P. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 29. [Google Scholar] [CrossRef] [PubMed]
- West, R.; Brown, J. Theory of Addiction; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Campbell, R.; Brown, J.; Gainforth, H. ABC of Behaviour Change Theories; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Nicolucci, A.; Kovacs Burns, K.; Holt, R.I.G.; Comaschi, M.; Hermanns, N.; Ishii, H.; Kokoszka, A.; Pouwer, F.; Skovlund, S.E.; Stuckey, H.; et al. Diabetes attitudes, wishes and needs second study (DAWN2™): Cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet. Med. 2013, 30, 767–777. [Google Scholar] [CrossRef]
- Beverly, E.A.; Hultgren, B.A.; Brooks, K.M.; Ritholz, M.D.; Abrahamson, M.J.; Weinger, K. Understanding physicians’ challenges when treating type 2 diabetic patients’ social and emotional difficulties: A qualitative study. Diabetes Care 2011, 34, 1086–1088. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Mullan, J.T.; Arean, P.; Glasgow, R.E.; Hessler, D.; Masharani, U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 2010, 33, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Aikens, J.E. Prospective associations between emotional distress and poor outcomes in type 2 diabetes. Diabetes Care 2012, 35, 2472–2478. [Google Scholar] [CrossRef] [Green Version]
- Nakahara, R.; Yoshiuchi, K.; Kumano, H.; Hara, Y.; Suematsu, H.; Kuboki, T. Prospective study on influence of psychosocial factors on glycemic control in Japanese patients with type 2 diabetes. Psychosomatics 2006, 47, 240–246. [Google Scholar] [CrossRef]
- Bryden, K.S.; Peveler, R.C.; Stein, A.; Neil, A.; Mayou, R.A.; Dunger, D.B. Clinical and psychological course of diabetes from adolescence to young adulthood-A longitudinal cohort study. Diabetes Care 2001, 24, 1536–1540. [Google Scholar] [CrossRef] [Green Version]
- Kokoszka, A.; Pouwer, F.; Jodko, A.; Radzio, R.; Mućko, P.; Bieńkowska, J.; Kuligowska, E.; Smoczyńska, O.; Skłodowska, Z. Serious diabetes-specific emotional problems in patients with type 2 diabetes who have different levels of comorbid depression: A Polish study from the European Depression in Diabetes (EDID) Research Consortium. Eur. Psychiatry 2009, 24, 425–430. [Google Scholar] [CrossRef]
- Van Der Heijden, M.M.P.; Van Dooren, F.E.P.; Pop, V.J.M.; Pouwer, F. Effects of exercise training on quality of life, symptoms of depression, symptoms of anxiety and emotional well-being in type 2 diabetes mellitus: A systematic review. Diabetologia 2013, 56, 1210–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, L.; Chesla, C.A.; Skaff, M.M.; Mullan, J.T.; Chun, K.M.; Kanter, R.A.; Gardiner, P.S. Patient-appraised couple emotion management and disease management among Chinese American patients with type 2 diabetes. J. Fam. Psychol. 2004, 18, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B.; Browne, J.L.; Lambert, G.W.; Jones, K.M.; Reddy, P.; Pouwer, F.; Speight, J. Severely obese people with diabetes experience impaired emotional well-being associated with socioeconomic disadvantage: Results from diabetes MILES-Australia. Diabetes Res. Clin. Pract. 2013, 101, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Stellar, J.E.; John-Henderson, N.; Anderson, C.L.; Gordon, A.M.; McNeil, G.D.; Keltner, D. Positive affect and markers of inflammation: Discrete positive emotions predict lower levels of inflammatory cytokines. Emotion 2015, 15, 129–133. [Google Scholar] [CrossRef]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Ryan, R.M. The Benefits of Being Present: Mindfulness and Its Role in Psychological Well-Being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Chapleau, M.A.; Paquin, K.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A Meta-Analytic Review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Teasdale, J.D.; Segal, Z.V.; Williams, J.M.G.; Ridgewaya, V.A.; Soulsby, J.M.; Lau, M.A. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J. Consult. Clin. Psychol. 2000, 68, 615–623. [Google Scholar] [CrossRef]
- Alberts, H.J.E.M.; Thewissen, R.; Raes, L. Dealing with problematic eating behaviour. The effects of a mindfulness-based intervention on eating behaviour, food cravings, dichotomous thinking and body image concern. Appetite 2012, 58, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Saxe, G.A.; Hébert, J.R.; Carmody, J.F.; Kabat-Zinn, J.; Rosenzweig, P.H.; Jarzobski, D.; Reed, G.W.; Blute, R.D. Can diet in conjunction with stress reduction affect the rate of increase in prostate specific antigen after biochemical recurrence of prostate cancer? J. Urol. 2001, 166, 2202–2207. [Google Scholar] [CrossRef]
- Tapper, K.; Shaw, C.; Ilsley, J.; Hill, A.J.; Bond, F.W.; Moore, L. Exploratory randomised controlled trial of a mindfulness-based weight loss intervention for women. Appetite 2009, 52, 396–404. [Google Scholar] [CrossRef]
- Morone, N.E.; Greco, C.M.; Weiner, D.K. Mindfulness meditation for the treatment of chronic low back pain in older adults: A randomized controlled pilot study. Pain 2008, 134, 310–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregg, J.A.; Callaghan, G.M.; Hayes, S.C.; Glenn-Lawson, J.L. Improving Diabetes Self-Management Through Acceptance, Mindfulness, and Values: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2007, 75, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Van Rhoon, L.; Byrne, M.; Morrissey, E.; Murphy, J.; McSharry, J. A systematic review of the behaviour change techniques and digital features in technology-driven type 2 diabetes prevention interventions. Digit. Health 2020, 6. [Google Scholar] [CrossRef]
- Bennich, B.B.; Røder, M.E.; Overgaard, D.; Egerod, I.; Munch, L.; Knop, F.K.; Vilsbøll, T.; Konradsen, H. Supportive and non-supportive interactions in families with a type 2 diabetes patient: An integrative review. Diabetol. Metab. Syndr. 2017, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wanko, N.S.; Brazier, C.W.; Young-Rogers, D.; Dunbar, V.G.; Boyd, B.; George, C.D.; Rhee, M.K.; El-Kebbi, I.M.; Cook, C.B. Exercise preferences and barriers in urban African Americans with type 2 diabetes. Diabetes Educ. 2004, 30, 502–513. [Google Scholar] [CrossRef]
- Loewenstein, G. Out of control: Visceral influences on behavior. Organ. Behav. Hum. Decis. Process. 1996, 65, 272–292. [Google Scholar] [CrossRef] [Green Version]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef]
- Hagger, M.S.; Wood, C.; Stiff, C.; Chatzisarantis, N.L. Ego depletion and the strength model of self-control: A meta-analysis. Psychol. Bull. 2010, 136, 495–525. [Google Scholar] [CrossRef]
- Oaten, M.; Cheng, K. Longitudinal gains in self-regulation from regular physical exercise. Br. J. Health Psychol. 2006, 11, 717–733. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Freeman, W.; Lightsey, R. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1999. [Google Scholar]
- McGee, S.L.; Hargreaves, M. Exercise adaptations: Molecular mechanisms and potential targets for therapeutic benefit. Nat. Rev. Endocrinol. 2020, 16, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Hofstetter, C.R.; Sallis, J.F.; Hovell, M.F. Some health dimensions of self-efficacy: Analysis of theoretical specificity. Soc. Sci. Med. 1990, 31, 1051–1056. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the intention-behaviour gap: Planning, self-efficacy, and action control in the adoption and maintenance of physical exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef]
- Geidl, W.; Schlesinger, S.; Mino, E.; Miranda, L.; Pfeifer, K. Dose–response relationship between physical activity and mortality in adults with noncommunicable diseases: A systematic review and meta-analysis of prospective observational studies. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 109. [Google Scholar] [CrossRef]
- Harkness, E.; Macdonald, W.; Valderas, J.; Coventry, P.; Gask, L.; Bower, P. Identifying psychosocial interventions that improve both physical and mental health in patients with diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 926–930. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Sex | Age (Range/Years) | T2D Duration (Years) | Probe Status | Reasons for Incomplete Probe | Education Highest Level | Race/Ethnicity |
|---|---|---|---|---|---|---|---|
| 1 | M | 35–44 | 1 to 2 | Fully Completed | NA | 2nd Level | White/Irish |
| 2 | M | 55–64 | 6 to 10 | Fully Completed | NA | 3rd Level (L6) | White/British |
| 3 | F | 55–64 | >10 | Fully Completed | NA | 3rd Level (L5) | White/English |
| 4 | F | 55–64 | 6 to 10 | Fully Completed | NA | 3rd Level (L8) | White/Irish |
| 5 | F | 35–44 | 1 to 2 | Fully Completed | NA | 3rd Level (L5) | White/Irish |
| 6 | M | 45–54 | >10 | Fully Completed | NA | 2nd Level | White/Dutch |
| 7 | M | 35–44 | 6 to 10 | Fully Completed | NA | 2nd Level | White/Irish |
| 8 | F | 55–64 | 4 to 6 | Fully Completed | NA | 3rd Level (L8) | White/Irish |
| 9 | F | 55–64 | >10 | Fully Completed | NA | 3rd Level (L6) | White/Irish |
| 10 | F | 55–64 | 2 to 4 | Fully Completed | NA | 3rd Level (L6) | White/Irish |
| 11 | F | 55–64 | 4 to 6 | Fully Completed | NA | 3rd Level (L7) | White/Irish |
| 12 | F | 55–64 | >10 | Fully Completed | NA | 2nd Level | White/Irish |
| 13 | M | 25–34 | 1 to 2 | Fully Completed | NA | 3rd Level (L8) | White/Irish |
| 14 | M | >65 | >10 | (11 days) | No reason provided | 2nd Level | White/Irish |
| 15 | F | NR | NR | (8 days) | In hospital | NR | White/Irish |
| 16 | F | 55–64 | 2 to 4 | (12 days) | No reason provided | Primary level | White/Irish |
| 17 | M | NR | NR | (15 days) | Family member in hospital | NR | White/Irish |
| 18 | F | NR | NR | (9 days) | No reason provided | NR | White/Irish |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cradock, K.A.; Quinlan, L.R.; Finucane, F.M.; Gainforth, H.L.; Martin Ginis, K.A.; Barros, A.C.d.; Sanders, E.B.N.; ÓLaighin, G. Identifying Barriers and Facilitators to Diet and Physical Activity Behaviour Change in Type 2 Diabetes Using a Design Probe Methodology. J. Pers. Med. 2021, 11, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020072
Cradock KA, Quinlan LR, Finucane FM, Gainforth HL, Martin Ginis KA, Barros ACd, Sanders EBN, ÓLaighin G. Identifying Barriers and Facilitators to Diet and Physical Activity Behaviour Change in Type 2 Diabetes Using a Design Probe Methodology. Journal of Personalized Medicine. 2021; 11(2):72. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020072
Chicago/Turabian StyleCradock, Kevin A., Leo R. Quinlan, Francis M. Finucane, Heather L. Gainforth, Kathleen A. Martin Ginis, Ana Correia de Barros, Elizabeth B. N. Sanders, and Gearóid ÓLaighin. 2021. "Identifying Barriers and Facilitators to Diet and Physical Activity Behaviour Change in Type 2 Diabetes Using a Design Probe Methodology" Journal of Personalized Medicine 11, no. 2: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11020072