
The Role of Immunohistochemical Markers for the Diagnosis and Prognosis of Adrenocortical Neoplasms

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples and Clinicopathologic Parameters
2.2. Histochemistry and Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. Clinical and Morphological Features of ACC and ACA Patients
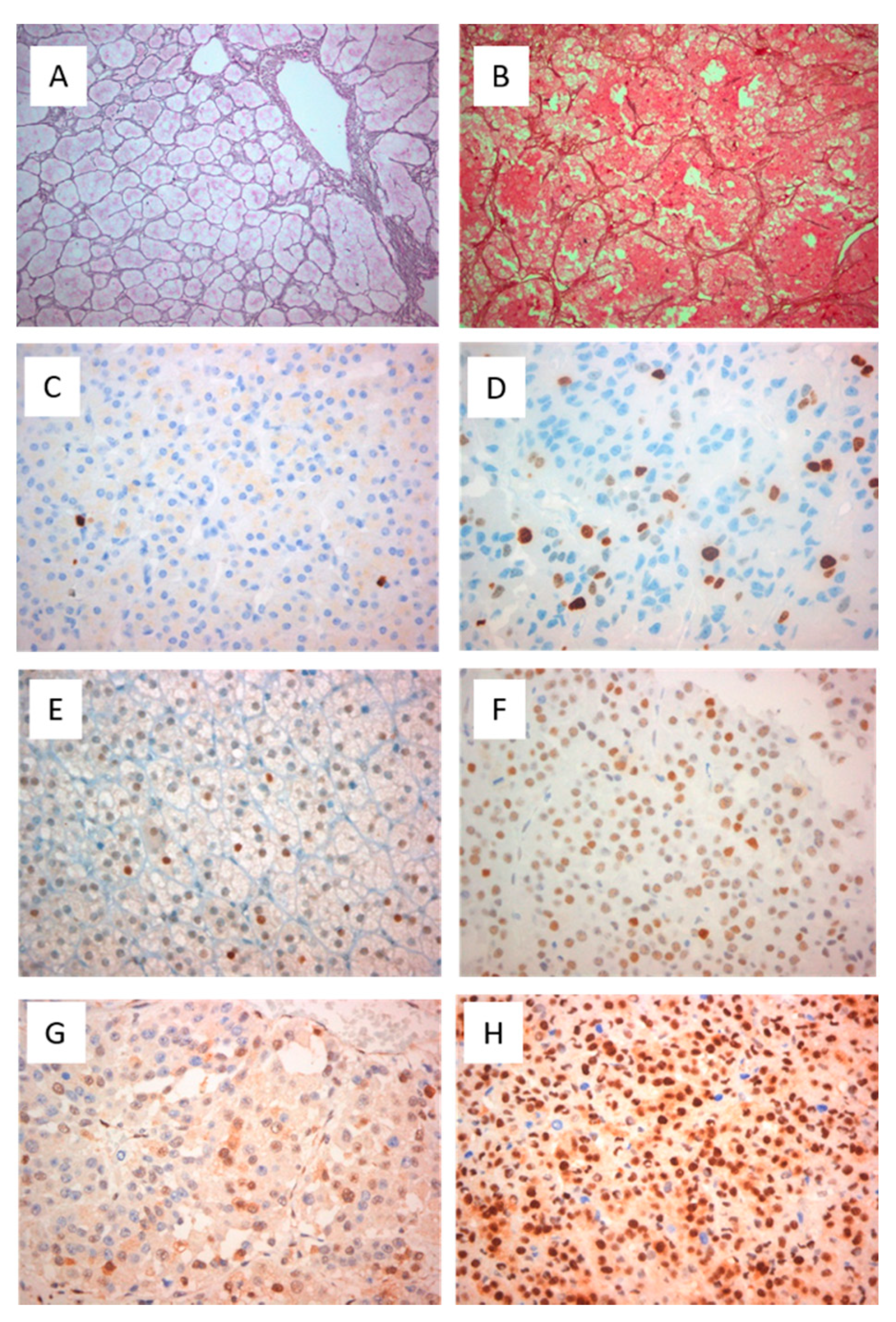
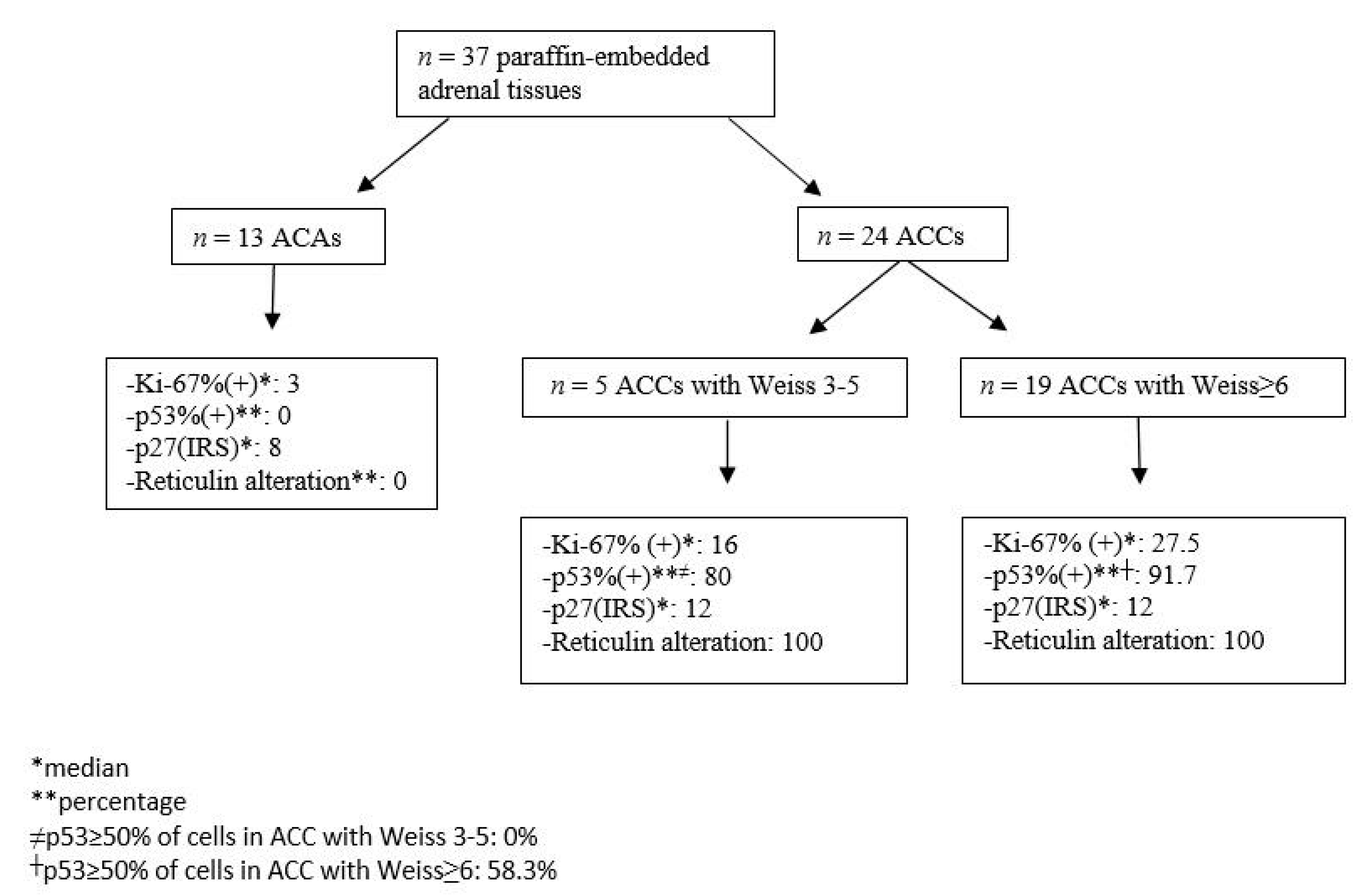
3.2. Expression of Histochemical and Immunohistochemical Markers in Adrenocortical Neoplasms
3.3. Prognostic Role of the Histopathological Markers in ACC Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allolio, B.; Fassnacht, M. Adrenocortical Carcinoma: Clinical Update. J. Clin. Endocrinol. Metab. 2006, 91, 2027–2037. [Google Scholar] [CrossRef] [Green Version]
- Ciaramella, P.D.; Vertemati, M.; Petrella, D.; Bonacina, E.; Grossrubatscher, E.; Duregon, E.; Volante, M.; Papotti, M.; Loli, P. Analysis of histological and immunohistochemical patterns of benign and malignant adrenocortical tumors by computerized morphometry. Pathol. Res. Pr. 2017, 213, 815–823. [Google Scholar] [CrossRef]
- Weiss, L.M. Comparative histologic study of 43 metastasizing and nonmetastasizing adrenocortical tumors. Am. J. Surg. Pathol. 1984, 8, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.K.; Weiss, L.M. The Weiss system for evaluating adrenocortical neoplasms: 25 years later. Hum. Pathol. 2009, 40, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Aubert, S.; Wacrenier, A.; Leroy, X.; Devos, P.; Carnaille, B.; Proye, C.; Wemeau, J.L.; Lecomte-Houcke, M.; Leteurtre, E. Weiss system revisited: A clinicopathologic and immunohistochemical study of 49 adrenocortical tumors. Am. J. Surg. Pathol. 2002, 26, 1612–1619. [Google Scholar] [CrossRef] [PubMed]
- Mete, O.; Asa, S.L.; Giordano, T.J.; Papotti, M.; Sasano, H.; Volante, M. Immunohistochemical Biomarkers of Adrenal Cortical Neoplasms. Endocr. Pathol. 2018, 29, 137–149. [Google Scholar] [CrossRef] [PubMed]
- de Reyniès, A.; Assié, G.; Rickman, D.S.; Tissier, F.; Groussin, L.; René-Corail, F.; Dousset, B.; Bertagna, X.; Clauser, E.; Bertherat, J. Gene expression profiling reveals a new classification of adrenocortical tumors and identifies molecular predictors of ma-lignancy and survival. J. Clin. Oncol. 2009, 27, 1108–1115. [Google Scholar] [CrossRef]
- Zheng, S.; Cherniack, A.D.; Dewal, N.; Moffitt, R.A.; Danilova, L.; Murray, B.A.; Lerario, A.M.; Else, T.; Knijnenburg, T.A.; Ciriello, G.; et al. Comprehensive Pan-Genomic characterization of adrenocortical carcinoma. In Proceedings of the AACR 106th Annual Meeting, Philadelphia, PA, USA, 18–22 April 2015. [Google Scholar]
- Else, T.; Kim, A.C.; Sabolch, A.; Raymond, V.M.; Kandathil, A.; Caoili, E.M.; Jolly, S.; Miller, B.S.; Giordano, T.J.; Hammer, G.D. Adrenocortical Carcinoma. Endocr. Rev. 2014, 35, 282–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, K.; Giordano, T.; Mete, O. Adrenal cortical proliferations. In Endocrine Pathology; Mete, O., Asa, S.L., Eds.; Cambridge University Press: Cambridge, UK, 2016; pp. 602–627. [Google Scholar]
- Mete, O.; Asa, S.L. Precursor lesions of endocrine system neoplasms. Pathology 2013, 45, 316–330. [Google Scholar] [CrossRef]
- Heaton, J.H.; Wood, M.A.; Kim, A.C.; Lima, L.O.; Barlaskar, F.M.; Almeida, M.Q.; Fragoso, M.C.B.V.; Kuick, R.; Lerario, A.M.; Simon, D.P.; et al. Progression to Adrenocortical Tumorigenesis in Mice and Humans through Insulin-Like Growth Factor 2 and β-Catenin. Am. J. Pathol. 2012, 181, 1017–1033. [Google Scholar] [CrossRef] [PubMed]
- Assie, G.; Giordano, T.; Bertherat, J. Gene expression profiling in adrenocortical neoplasia. Mol. Cell. Endocrinol. 2012, 351, 111–117. [Google Scholar] [CrossRef]
- Assié, G.; Letouzé, E.; Fassnacht, M.; Jouinot, A.; Luscap, W.; Barreau, O.; Omeiri, H.; Rodriguez, S.; Perlemoine, K.; René-Corail, F.; et al. Integrated genomic characterization of adrenocortical carcinoma. Nat. Genet. 2014, 46, 607–612. [Google Scholar] [CrossRef]
- Espiard, S.; Bertherat, J. The Genetics of Adrenocortical Tumors. Endocrinol. Metab. Clin. N. Am. 2015, 44, 311–334. [Google Scholar] [CrossRef] [PubMed]
- Giordano, T.J. Adrenocortical tumors: An integrated clinical, pathologic, and molecular approach at the University of Michi-gan. Arch. Path. Lab. Med. 2010, 134, 1440–1443. [Google Scholar] [CrossRef] [PubMed]
- Ragazzon, B.; Libé, R.; Gaujoux, S.; Assié, G.; Fratticci, A.; Launay, P.; Clauser, E.; Bertagna, X.; Tissier, F.; De Reyniès, A.; et al. Transcriptome Analysis Reveals that p53 and β-Catenin Alterations Occur in a Group of Aggressive Adrenocortical Cancers. Cancer Res. 2010, 70, 8276–8281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papotti, M.; Volante, M.; Duregon, E.; Delsedime, L.; Terzolo, M.; Berruti, A.; Rosai, J. Adrenocortical Tumors With Myxoid Features: A Distinct Morphologic and Phenotypical Variant Exhibiting Malignant Behavior. Am. J. Surg. Pathol. 2010, 34, 973–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duregon, E.; Cappellesso, R.; Maffeis, V.; Zaggia, B.; Ventura, L.; Berruti, A.; Terzolo, M.; Fassina, A.; Volante, M.; Papotti, M. Validation of the prognostic role of the "Helsinki Score” in 225 cases of adrenocortical carcinoma. Hum. Pathol. 2017, 62, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mete, O.; Asa, S.L. Pathological definition and clinical significance of vascular invasion in thyroid carcinomas of follicular epithelial derivation. Mod. Pathol. 2011, 24, 1545–1552. [Google Scholar] [CrossRef] [Green Version]
- Bisceglia, M.; Ludovico, O.; Di Mattia, A.; Ben-Dor, D.; Sandbank, J.; Pasquinelli, G.; Lau, S.K.; Weiss, L.M. Adrenocortical Oncocytic Tumors: Report of 10 Cases and Review of the Literature. Int. J. Surg. Pathol. 2004, 12, 231–243. [Google Scholar] [CrossRef]
- Wong, D.D.; Spagnolo, D.V.; Bisceglia, M.; Havlat, M.; McCallum, D.; Platten, M.A. Oncocytic adrenocortical neoplasms: A clinicopathologic study of 13 new cases emphasizing the importance of their recognition. Hum. Pathol. 2011, 42, 489–499. [Google Scholar] [CrossRef]
- Miller, B.S.; Gauger, P.G.; Hammer, G.D.; Giordano, T.J.; Doherty, G.M. Proposal for modification of the ENSAT staging system for adrenocortical carcinoma using tumor grade. Langenbeck’s Arch. Surg. 2010, 395, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Assié, G.; Antoni, G.; Tissier, F.; Caillou, B.; Abiven, G.; Gicquel, C.; Leboulleux, S.; Travagli, J.-P.; Dromain, C.; Bertagna, X.; et al. Prognostic Parameters of Metastatic Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2007, 92, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Wanis, K.N.; Kanthan, R. Diagnostic and prognostic features in adrenocortical carcinoma: A single institution case series and review of the literature. World J. Surg. Oncol. 2015, 13, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mete, O.; Gucer, H.; Kefeli, M.; Asa, S.L. Diagnostic and Prognostic Biomarkers of Adrenal Cortical Carcinoma. Am. J. Surg. Pathol. 2018, 42, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G.; La Rosa, S. Ki67 labeling index: Assessment and prognostic role in gastroenteropancreatic neuroendocrine neoplasms. Virchows Arch. Pathol. Anat. Histol. 2017, 472, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Lin, R.K.; Tan, Y.H.; Chen, J.T.; Chen, C.Y.; Wang, Y.C. Wild-Type p53 Overexpression and Its Correlation With MDM2 and p14ARF Alterations: An Alternative Pathway to Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2005, 23, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Köbel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas. Int. J. Gynecol. Pathol. 2019, 38, S123–S131. [Google Scholar] [CrossRef] [PubMed]
- Xiong, D.D.; He, R.Q.; Lan, A.H.; Chen, W.J.; Luo, Y.H.; Ye, Z.H.; Ma, J.; Chen, G.; Dang, Y.W. Clinical significances of p27 in digestive tract cancers: A comprehensive analysis on immunohistochemistry staining, published literatures, microarray and RNA-seq data. Oncotarget 2018, 9, 12284–12303. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Upadhye, S.; Worster, A. Understanding receiver operating characteristic (ROC) curves. CJEM 2006, 8, 19–20. [Google Scholar] [CrossRef]
- Fonseca, D.; Murthy, S.S.; Tagore, K.R.; Rao, B.V.; Thamminedi, S.R.; Raju, K.; Sharma, R.; Challa, S. Diagnosis of adrenocortical tumors by reticulin algorithm. Indian J. Endocrinol. Metab. 2017, 21, 734. [Google Scholar] [CrossRef]
- Volante, M.; Bollito, E.; Sperone, P.; Tavaglione, V.; Daffara, F.; Porpiglia, F.; Terzolo, M.; Berruti, A.; Papotti, M. Clinico-pathological study of a series of 92 adrenocortical carcinomas: From a proposal of simplified diagnostic algorithm to prognostic stratification. Histopathology 2009, 55, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duregon, E.; Fassina, A.; Volante, M.; Nesi, G.; Santi, R.; Gatti, G.; Cappellesso, R.; Ciaramella, P.D.; Ventura, L.; Gambacorta, M. The reticulin algorithm for adrenocortical tumor diagnosis: A multicentric validation study on 245 unpublished cases. Am. J. Surg. Pathol. 2013, 37, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Sung, T.Y.; Choi, Y.M.; Kim, W.B.; Lee, Y.M.; Kim, T.Y.; Shong, Y.K.; Song, D.E. Myxoid and Sarcomatoid Variants of Adrenocortical Carcinoma: Analysis of Rare Variants in Single Tertiary Care Center. J. Korean Med Sci. 2017, 32, 764–771. [Google Scholar] [CrossRef]
- Morimoto, R.; Satoh, F.; Murakami, O.; Suzuki, T.; Abe, T.; Tanemoto, M.; Abe, M.; Uruno, A.; Ishidoya, S.; Arai, Y. Immunohistochemistry of a proliferation marker Ki67/MIB1 in adrenocortical carcinomas: Ki67/MIB1 labeling index is a predictor for recurrence of adrenocortical carcinomas. Endocr. J. 2008, 55, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Babińska, A.; Pęksa, R.; Wiśniewski, P.; Świątkowska-Stodulska, R.; Sworczak, K. Diagnostic and prognostic role of SF1, IGF2, Ki67, p53, adiponectin, and leptin receptors in human adrenal cortical tumors. J. Surg. Oncol. 2017, 116, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Jouinot, A.; Assie, G.; Libe, R.; Fassnacht, M.; Papathomas, T.; Barreau, O.; De La Villeon, B.; Faillot, S.; Hamzaoui, N.; Neou, M.; et al. DNA methylation is an independent prognostic marker of survival in adrenocortical cancer. J. Clin. Endocrinol. Metab. 2016, 102, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Papathomas, T.G.; Pucci, E.; Giordano, T.J.; Lu, H.; Duregon, E.; Volante, M.; Papotti, M.; Lloyd, R.V.; Tischler, A.S.; Van Nederveen, F.H.; et al. An International Ki67 Reproducibility Study in Adrenal Cortical Carcinoma. Am. J. Surg. Pathol. 2016, 40, 569–576. [Google Scholar] [CrossRef]
- Manfredi, J.J. The Mdm2-p53 relationship evolves: Mdm2 swings both ways as an oncogene and a tumor suppressor. Genes Dev. 2010, 24, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Moll, U.M.; Petrenko, O. The MDM2-p53 interaction. Mol. Cancer Res. 2003, 1, 1001–1008. [Google Scholar]
- Stojadinovic, A.; Ghossein, R.A.; Hoos, A.; Nissan, A.; Marshall, D.; Dudas, M.; Cordon-Cardo, C.; Jaques, D.P.; Brennan, M.F. Adrenocortical Carcinoma: Clinical, Morphologic, and Molecular Characterization. J. Clin. Oncol. 2002, 20, 941–950. [Google Scholar] [CrossRef]
- Reincke, M.; Karl, M.; Travis, W.H.; Mastorakos, G.; Allolio, B.; Linehan, H.M.; Chrousos, G.P. p53 mutations in human adrenocortical neoplasms: Immunohistochemical and molecular studies. J. Clin. Endocrinol. Metab. 1994, 78, 790–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barzon, L.; Chilosi, M.; Fallo, F.; Martignoni, G.; Montagna, L.; Palù, G.; Boscaro, M. Molecular analysis of CDKN1C and TP53 in sporadic adrenal tumors. Eur. J. Endocrinol. 2001, 145, 207–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libè, R.; Fratticci, A.; Bertherat, J. Adrenocortical cancer: Pathophysiology and clinical management. Endocr. Relat. Cancer 2007, 14, 13–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gicquel, C.; Bertagna, X.; Gaston, V.; Coste, J.; Louvel, A.; Baudin, E.; Bertherat, J.; Chapuis, Y.; Duclos, J.M.; Schlumberger, M.; et al. Molecular markers and long-term recurrences in a large cohort of patients with sporadic adrenocortical tumors. Cancer Res. 2001, 61, 6762–6767. [Google Scholar] [PubMed]
- Pereira, S.S.; Morais, T.; Costa, M.M.; Monteiro, M.P.; Pignatelli, D. The emerging role of the molecular marker p27 in the differential diagnosis of adrenocortical tumors. Endocr. Connect. 2013, 2, 137–145. [Google Scholar] [CrossRef]
- Wasserman, J.D.; Zambetti, G.P.; Malkin, D. Towards an understanding of the role of p53 in adrenocortical carcinogenesis. Mol. Cell. Endocrinol. 2012, 351, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Edgren, M.; Eriksson, B.; Wilander, E.; Westlin, J.E.; Nilsson, S.; Oberg, K. Biological characteristics of adrenocortical carcinoma: A study of p53, IGF, EGF-r, Ki-67 and PCNA in 17 adrenocortical carcinomas. Anticancer. Res. 1997, 17, 1303–1309. [Google Scholar]
- Stojadinovic, A.; Brennan, M.F.; Hoos, A.; Omeroglu, A.; Leung, D.H.Y.; Dudas, M.E.; Nissan, A.; Cordon-Cardo, C.; Ghossein, R.A. Adrenocortical Adenoma and Carcinoma: Histopathological and Molecular Comparative Analysis. Mod. Pathol. 2003, 16, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Waldmann, J.; Patsalis, N.; Fendrich, V.; Langer, P.; Saeger, W.; Chaloupka, B.; Ramaswamy, A.; Fassnacht, M.; Bartsch, D.K.; Slater, E.P. Clinical impact of TP53 alterations in adrenocortical carcinomas. Langenbeck’s Arch. Surg. 2011, 397, 209–216. [Google Scholar] [CrossRef]
- Lee, J.; Kim, S.S. The function of p27KIP1during tumor development. Exp. Mol. Med. 2009, 41, 765–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakazumi, H.; Sasano, H.; Iino, K.; Ohashi, Y.; Orikasa, S. Expression of cell cycle inhibitor p27 and Ki-67 in human adre-nocortical neoplasms. Mod. Pathol. 1998, 11, 1165–1170. [Google Scholar] [PubMed]
- Nickeleit, I.; Zender, S.; Kossatz, U.; Malek, N.P. p27kip1: A target for tumor therapies? Cell Div. 2007, 2, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | ACCs (n = 24) | ACAs (n = 13) | p-Value |
|---|---|---|---|
| Clinical characteristics | |||
| Age (median(min−max)), ys | 54.5(21–76) | 63.5(38–71) | 0.119 |
| Sex (Female, n(%)) | 14(58.3) | 9(69.2) | 0.724 |
| Size (median(min-max)), mm | 10(1–24) | 5(1.3–9) | 0.002 |
| Functionality (n(%)) | 11(45.8) | 8(61.5) | 0.495 |
| Histopathological characteristics (median(min-max)) | |||
| Weiss | 6(4–9) | 0(0–1) | 0.001 |
| Helsinki | 28(10–56) | 3(1–5) | <0.001 |
| Reticulin score | 4(3–4) | 0(0–1) | <0.001 |
| Immunohistochemical characteristics | |||
| Ki-67% (median (min-max)) | 23.5(15–45) | 3(1–5) | <0.001 |
| p27 (IRS) (median(min-max)) | 12(4–12) | 8(8–12) | 0.121 |
| p53 (pathological, n(%)) | 15(88.2) | 0(0) | <0.001 |
| p53 (WT vs. overexpression 20–49% vs. overexpression ≥50%, n(%)) | 2(11.)/8(47.1)/7(41.2) | All wild | <0.001 |
| Clinical Characteristics | |
| Stage (median (min-max)) | 3 (1–4) |
| 1 or 2 (n(%)) | 9 (37.5) |
| 3 or 4 (n (%)) | 15 (62.5) |
| Metastatic at presentation (n (%)) | 5 (20.8) |
| Duration of mitotane treatment (median (min-max)), months | 9.8 (4.6–36.9) |
| PFS (median (min-max)), months | 6.57 (1.93–19.7) |
| Rate of PD (n (%)) | 13 (54.2) |
| Mortality (median (min-max)), months | 11.4 (5.63–27.5) |
| Mortality rate (n (%)) | 8 (33.3) |
| Follow-up (median (min-max)), months | 18.4 (2.13–101.9) |
| Histopathological Characteristics | |
| Capsular invasion (n (%)) | 19 (79.2) |
| Vascular invasion (n (%)) | 11 (45.8) |
| Necrosis (n (%)) | 23 (95.8) |
| Mitoses >20 per 50 HPF (n (%)) | 11 (45.8) |
| Atypical mitoses (n (%)) | 21 (87.5) |
| Characteristics | No Relapse | Relapse | p-Value | No Death | Death | p-Value |
|---|---|---|---|---|---|---|
| Clinical | ||||||
| Size | 9(3.5–15.2) | 10(1–24) | 0.417 | 9.5(3.5–24) | 11(1–16) | 0.759 |
| Functionality (n (%)) | 1(9.09) | 10(76.9) | 0.001 | 5(31.3) | 6(75) | 0.043 |
| Histopathological | ||||||
| Weiss (median (min-max)) | 6(4–8) | 6(4–9) | 0.434 | 6(4–8) | 6.5(6–9) | 0.481 |
| Helsinki (median (min-max)) | 30(10–56) | 28(20–53) | 0.619 | 28(10–56) | 33(23–53) | 0.426 |
| Capsular invasion (n (%)) | 7(63.6) | 12(92.3) | 0.142 | 12(75) | 7(87.5) | 0.631 |
| Vascular invasion (n (%)) | 4(36.4) | 7(53.9) | 0.444 | 6(37.5) | 5(62.5) | 0.390 |
| Nuclear atypia (n (%)) | 10(90.9) | 13(100) | 0.458 | 15(93.8) | 8(100) | 0.999 |
| Mitoses >20 per 50HPF (n (%)) | 3(27.3) | 8(61.5) | 0.123 | 7(43.8) | 4(50) | 0.999 |
| Reticulin (score 4, n (%)) | 5(55.6) | 4(44.4) | 0.999 | 6(50) | 3(50) | 0.999 |
| Immunohistopathological (median(min-max)) | ||||||
| Ki-67% | 23.5(15–40) | 25(15–45) | 0.668 | 23.5(15–40) | 25(15–45) | 0.785 |
| p27([IRS) | 12(8–12) | 9(4–12) | 0.175 | 12(6–12) | 9(4–12) | 0.302 |
| p53 (pathological, n (%)) | 7(87.5) | 8(88.9) | 0.999 | 9(81.8) | 6(100) | 0.515 |
| p53 (WT/overexpression 21–50%/≥ 50%, n (%)) | 1(12.5)/6(75)/1(12.5) | 1(11.1)/2(22.2)/6(66.7) | 0.057 | 2(18.2)/8(72.7)/1(9.1) | 0(0)/0(0)/6(100) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelousi, A.; Kyriakopoulos, G.; Athanasouli, F.; Dimitriadi, A.; Kassi, E.; Aggeli, C.; Zografos, G.; Kaltsas, G. The Role of Immunohistochemical Markers for the Diagnosis and Prognosis of Adrenocortical Neoplasms. J. Pers. Med. 2021, 11, 208. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11030208
Angelousi A, Kyriakopoulos G, Athanasouli F, Dimitriadi A, Kassi E, Aggeli C, Zografos G, Kaltsas G. The Role of Immunohistochemical Markers for the Diagnosis and Prognosis of Adrenocortical Neoplasms. Journal of Personalized Medicine. 2021; 11(3):208. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11030208
Chicago/Turabian StyleAngelousi, Anna, Georgios Kyriakopoulos, Fani Athanasouli, Anastasia Dimitriadi, Eva Kassi, Chrysanthi Aggeli, George Zografos, and Gregory Kaltsas. 2021. "The Role of Immunohistochemical Markers for the Diagnosis and Prognosis of Adrenocortical Neoplasms" Journal of Personalized Medicine 11, no. 3: 208. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11030208