
Ratings of the Effectiveness of Nutraceuticals for Autism Spectrum Disorders: Results of a National Survey

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics and Medical History
3.2. Nutraceuticals
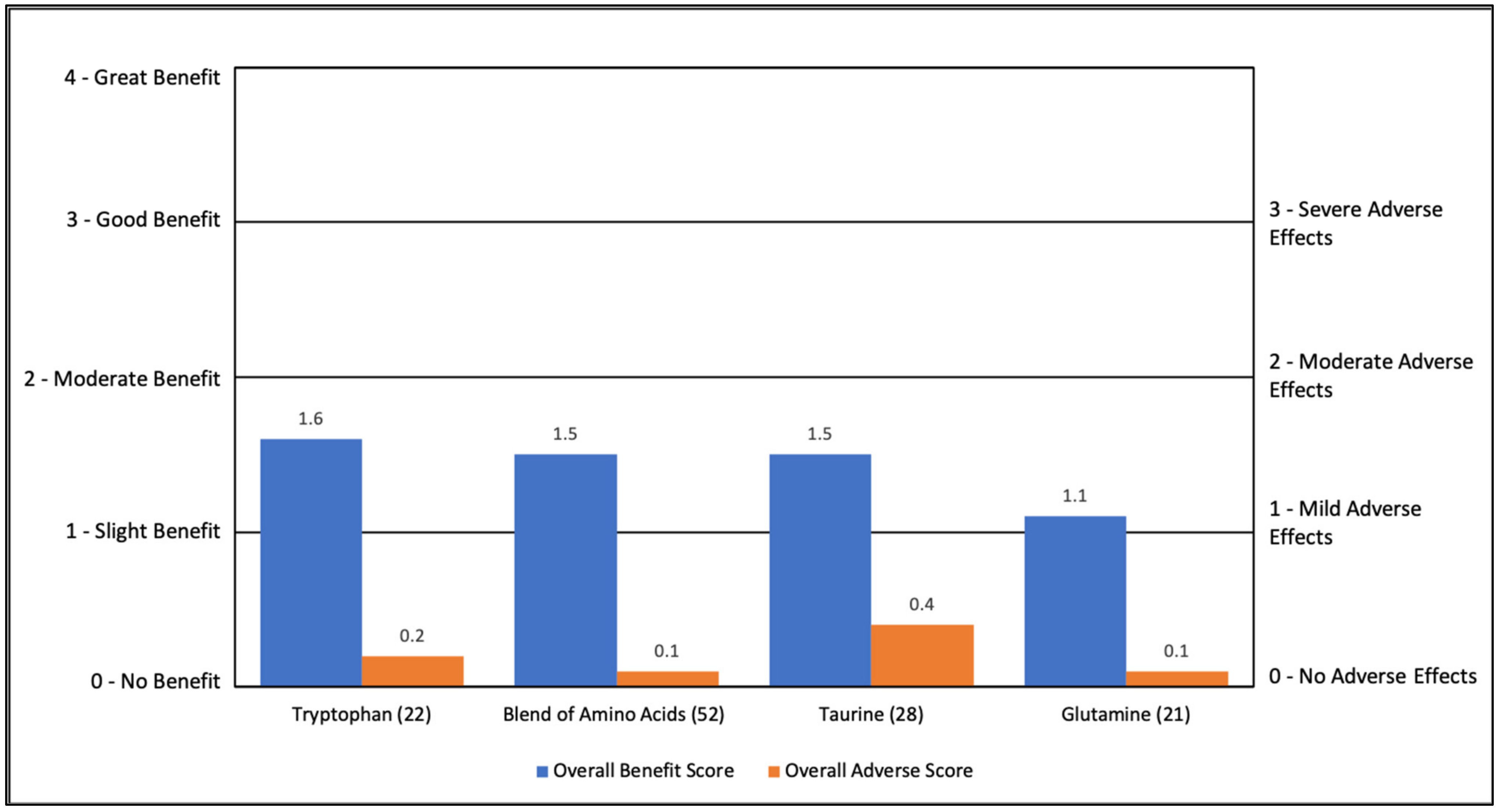
3.2.1. Amino Acids
3.2.2. Fatty Acids
3.2.3. Glutathione-Related Nutraceuticals
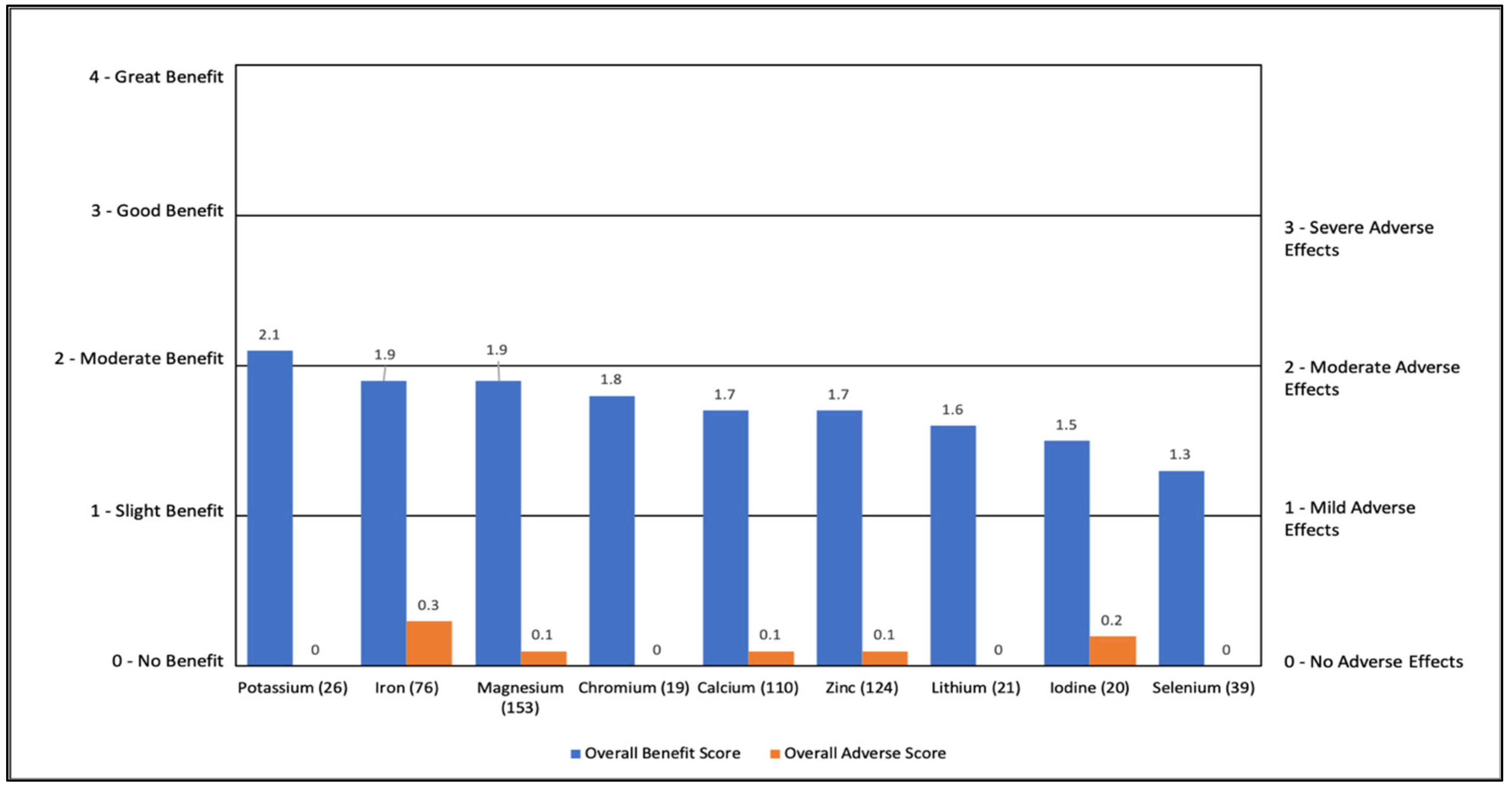
3.2.4. Individual Minerals
3.2.5. Individual Vitamins/Vitamin-like Nutraceuticals
3.2.6. Multivitamins
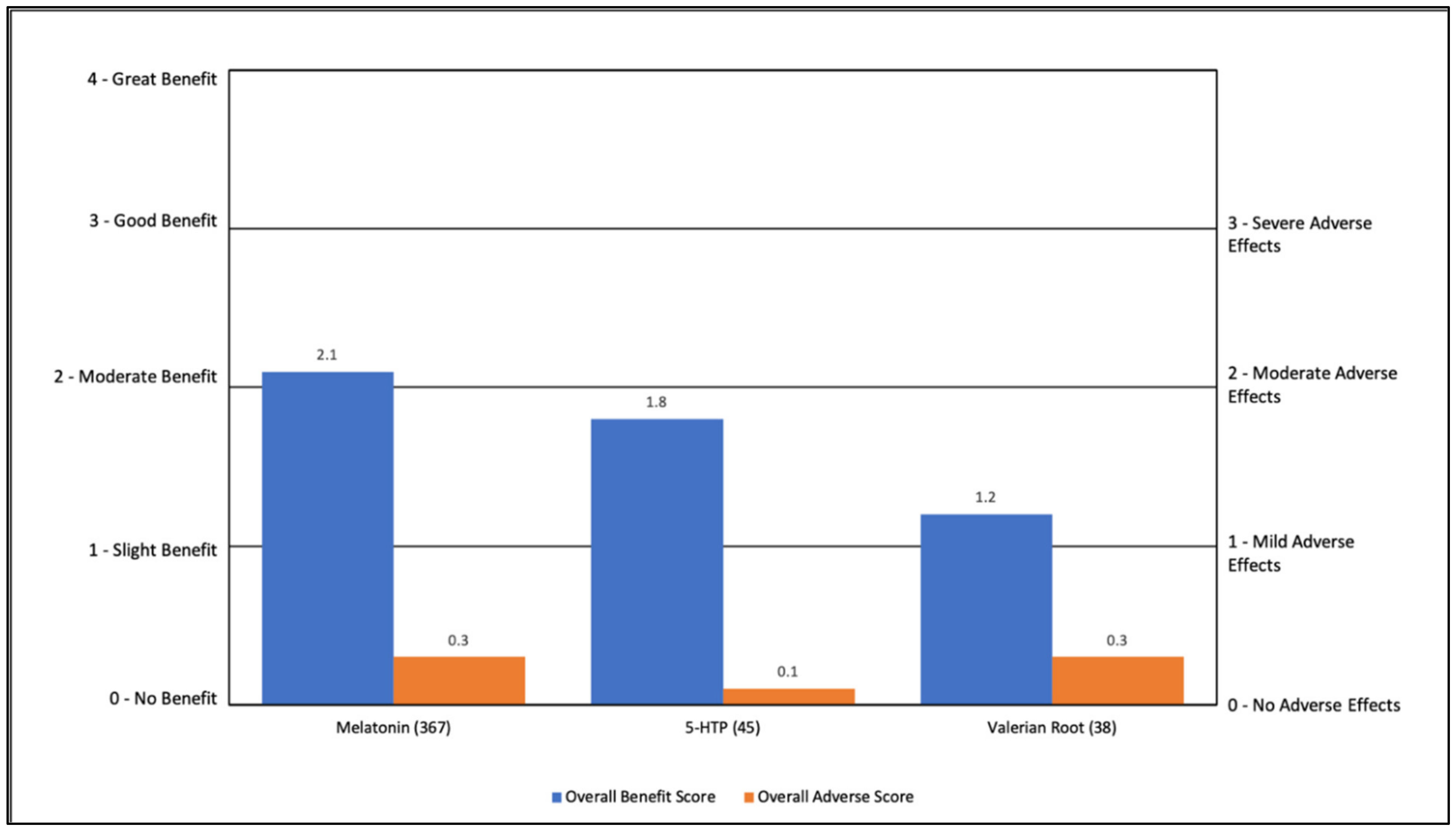
3.2.7. Sleep-Related Nutraceuticals
3.2.8. Other Miscellaneous Nutraceuticals
3.2.9. Average of All Nutraceuticals
3.2.10. Top Nutraceuticals by Symptom
3.2.11. Overall Effects of Nutraceuticals
3.3. Analysis of the Effect on Specific Supplements on Change in Severity
3.3.1. Specific Nutraceutical Use
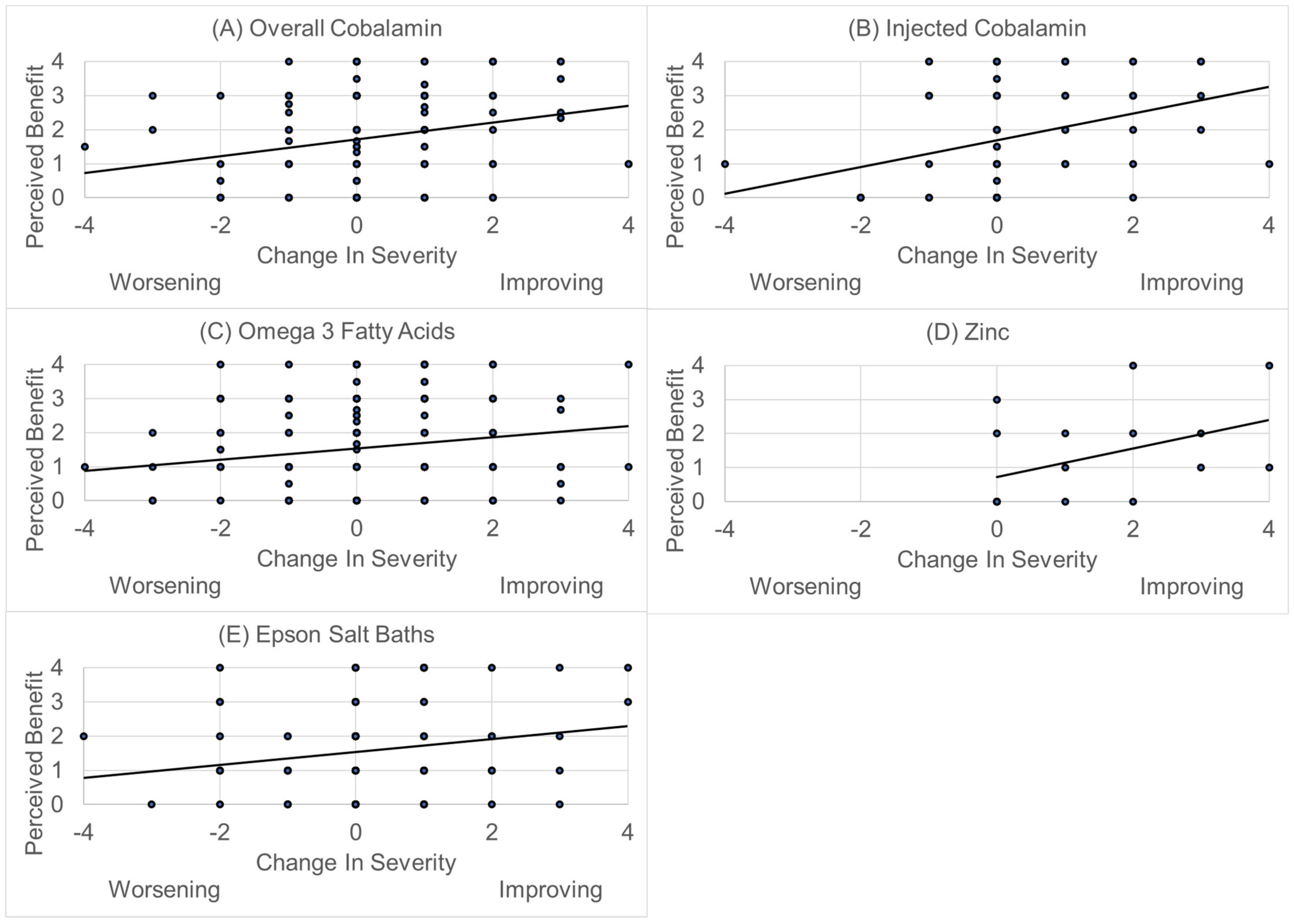
3.3.2. Perceived Benefit and Change in Autism Severity
4. Discussion
4.1. Strengths of This Study
4.2. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Dunn, K.; Rydzewska, E.; Fleming, M.; Cooper, S.A. Prevalence of mental health conditions, sensory impairments and physical disability in people with co-occurring intellectual disabilities and autism compared with other people: A cross-sectional total population study in Scotland. BMJ Open 2020, 10, e035280. [Google Scholar] [CrossRef]
- Viscidi, E.W.; Triche, E.W.; Pescosolido, M.F.; McLean, R.L.; Joseph, R.M.; Spence, S.J.; Morrow, E.M. Clinical characteristics of children with autism spectrum disorder and co-occurring epilepsy. PLoS ONE 2013, 8, e67797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holingue, C.; Newill, C.; Lee, L.C.; Pasricha, P.J.; Daniele Fallin, M. Gastrointestinal symptoms in autism spectrum disorder: A review of the literature on ascertainment and prevalence. Autism Res. 2018, 11, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef] [PubMed]
- James, S.J.; Cutler, P.; Melnyk, S.; Jernigan, S.; Janak, L.; Gaylor, D.W.; Neubrander, J.A. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 2004, 80, 1611–1617. [Google Scholar] [CrossRef] [Green Version]
- James, S.J.; Melnyk, S.; Jernigan, S.; Cleves, M.A.; Halsted, C.H.; Wong, D.H.; Cutler, P.; Bock, K.; Boris, M.; Bradstreet, J.J.; et al. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2006, 141, 947–956. [Google Scholar] [CrossRef] [Green Version]
- Rossignol, D.A.; Frye, R.E. Melatonin in autism spectrum disorders: A systematic review and meta-analysis. Dev. Med. Child. Neurol. 2011, 53, 783–792. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. Mitochondrial dysfunction in autism spectrum disorders: A systematic review and meta-analysis. Mol. Psychiatry 2012, 17, 290–314. [Google Scholar] [CrossRef] [Green Version]
- Rose, S.; Niyazov, D.M.; Rossignol, D.A.; Goldenthal, M.; Kahler, S.G.; Frye, R.E. Clinical and Molecular Characteristics of Mitochondrial Dysfunction in Autism Spectrum Disorder. Mol. Diagn. Ther. 2018, 22, 571–593. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Shi, X.J.; Liu, H.; Mao, X.; Gui, L.N.; Wang, H.; Cheng, Y. Oxidative stress marker aberrations in children with autism spectrum disorder: A systematic review and meta-analysis of 87 studies (N = 9109). Transl. Psychiatry 2021, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, A.; Neri, M.; Cesario, A.; Adams, J.B.; Domenici, E.; Dalla Bernardina, B.; Bonassi, S. Oxidative stress-related biomarkers in autism: Systematic review and meta-analyses. Free. Radic. Biol. Med. 2012, 52, 2128–2141. [Google Scholar] [CrossRef]
- LeClerc, S.; Easley, D. Pharmacological therapies for autism spectrum disorder: A review. Pharm. Ther. 2015, 40, 389–397. [Google Scholar]
- Craig, F.; De Giacomo, A.; Operto, F.F.; Margari, M.; Trabacca, A.; Margari, L. Association between feeding/mealtime behavior problems and internalizing/externalizing problems in autism spectrum disorder (ASD), other neurodevelopmental disorders (NDDs) and typically developing children. Minerva Pediatr. 2019. [Google Scholar] [CrossRef]
- Canals-Sans, J.; Esteban-Figuerola, P.; Morales-Hidalgo, P.; Arija, V. Do Children with Autism Spectrum Disorders Eat Differently and Less Adequately than Those with Subclinical ASD and Typical Development? EPINED Epidemiological Study. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sharp, W.G.; Berry, R.C.; McCracken, C.; Nuhu, N.N.; Marvel, E.; Saulnier, C.A.; Klin, A.; Jones, W.; Jaquess, D.L. Feeding problems and nutrient intake in children with autism spectrum disorders: A meta-analysis and comprehensive review of the literature. J. Autism Dev. Disord. 2013, 43, 2159–2173. [Google Scholar] [CrossRef]
- Page, S.D.; Souders, M.C.; Kral, T.V.E.; Chao, A.M.; Pinto-Martin, J. Correlates of Feeding Difficulties among Children with Autism Spectrum Disorder: A Systematic Review. J. Autism Dev. Disord. 2021, 1–20. [Google Scholar] [CrossRef]
- Adams, J.B.; Audhya, T.; Geis, E.; Gehn, E.; Fimbres, V.; Pollard, E.L.; Mitchell, J.; Ingram, J.; Hellmers, R.; Laake, D.; et al. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients 2018, 10, 369. [Google Scholar] [CrossRef] [Green Version]
- Owen-Smith, A.A.; Bent, S.; Lynch, F.L.; Coleman, K.J.; Yau, V.M.; Pearson, K.A.; Massolo, M.L.; Quinn, V.; Croen, L.A. Prevalence and Predictors of Complementary and Alternative Medicine Use in a Large Insured Sample of Children with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2015, 17, 40–51. [Google Scholar] [CrossRef] [Green Version]
- Frye, R.E.; Sreenivasula, S.; Adams, J.B. Traditional and non-traditional treatments for autism spectrum disorder with seizures: An on-line survey. BMC Pediatr. 2011, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- ARI. ARI Publ. 34: Parent Ratings of Behavorial Effects of Biomedical Interventions. Available online: https://www.autism.org/treatment-ratings-for-autism/ (accessed on 6 June 2021).
- Rossignol, D.A. Novel and emerging treatments for autism spectrum disorders: A systematic review. Ann. Clin. Psychiatry 2009, 21, 213–236. [Google Scholar] [PubMed]
- Frye, R.E.; Slattery, J.; Delhey, L.; Furgerson, B.; Strickland, T.; Tippett, M.; Sailey, A.; Wynne, R.; Rose, S.; Melnyk, S.; et al. Folinic acid improves verbal communication in children with autism and language impairment: A randomized double-blind placebo-controlled trial. Mol. Psychiatry 2018, 23, 247–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batebi, N.; Moghaddam, H.S.; Hasanzadeh, A.; Fakour, Y.; Mohammadi, M.R.; Akhondzadeh, S. Folinic Acid as Adjunctive Therapy in Treatment of Inappropriate Speech in Children with Autism: A Double-Blind and Placebo-Controlled Randomized Trial. Child. Psychiatry Hum. Dev. 2021, 52, 928–938. [Google Scholar] [CrossRef]
- Renard, E.; Leheup, B.; Gueant-Rodriguez, R.M.; Oussalah, A.; Quadros, E.V.; Gueant, J.L. Folinic acid improves the score of Autism in the EFFET placebo-controlled randomized trial. Biochimie 2020, 173, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Holloway, C. Pilot study of a moderate dose multivitamin/mineral supplement for children with autistic spectrum disorder. J. Altern. Complement. Med. 2004, 10, 1033–1039. [Google Scholar] [CrossRef]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S.; et al. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr. 2011, 11, 1–30. [Google Scholar] [CrossRef]
- Lee, T.M.; Lee, K.M.; Lee, C.Y.; Lee, H.C.; Tam, K.W.; Loh, E.W. Effectiveness of N-acetylcysteine in autism spectrum disorders: A meta-analysis of randomized controlled trials. Aust. N. Z. J. Psychiatry 2021, 55, 196–206. [Google Scholar] [CrossRef]
- McGuinness, G.; Kim, Y. Sulforaphane treatment for autism spectrum disorder: A systematic review. EXCLI J. 2020, 19, 892–903. [Google Scholar] [CrossRef]
- Coleman, D.M.; Adams, J.B.; Anderson, A.L.; Frye, R.E. Rating of the Effectiveness of 26 Psychiatric and Seizure Medications for Autism Spectrum Disorder: Results of a National Survey. J. Child. Adolesc. Psychopharmacol. 2019, 29, 107–123. [Google Scholar] [CrossRef] [Green Version]
- Fahmy, S.F.; El-hamamsy, M.H.; Zaki, O.K.; Badary, O.A. l-Carnitine supplementation improves the behavioral symptoms in autistic children. Res. Autism Spectr. Disord. 2013, 7, 159–166. [Google Scholar] [CrossRef]
- Geier, D.A.; Kern, J.K.; Davis, G.; King, P.G.; Adams, J.B.; Young, J.L.; Geier, M.R. A prospective double-blind, randomized clinical trial of levocarnitine to treat autism spectrum disorders. Med. Sci. Monit. 2011, 17, PI15. [Google Scholar] [CrossRef] [Green Version]
- Mousavinejad, E.; Ghaffari, M.A.; Riahi, F.; Hajmohammadi, M.; Tiznobeyk, Z.; Mousavinejad, M. Coenzyme Q10 supplementation reduces oxidative stress and decreases antioxidant enzyme activity in children with autism spectrum disorders. Psychiatry Res. 2018, 265, 62–69. [Google Scholar] [CrossRef]
- Munasinghe, S.A.; Oliff, C.; Finn, J.; Wray, J.A. Digestive enzyme supplementation for autism spectrum disorders: A double-blind randomized controlled trial. J. Autism Dev. Disord. 2010, 40, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Saad, K.; Eltayeb, A.A.; Mohamad, I.L.; Al-Atram, A.A.; Elserogy, Y.; Bjorklund, G.; El-Houfey, A.A.; Nicholson, B. A Randomized, Placebo-controlled Trial of Digestive Enzymes in Children with Autism Spectrum Disorders. Clin. Psychopharmacol. Neurosci. 2015, 13, 188–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendren, R.L.; James, S.J.; Widjaja, F.; Lawton, B.; Rosenblatt, A.; Bent, S. Randomized, Placebo-Controlled Trial of Methyl B12 for Children with Autism. J. Child. Adolesc. Psychopharmacol. 2016, 26, 774–783. [Google Scholar] [CrossRef]
- Gringras, P.; Nir, T.; Breddy, J.; Frydman-Marom, A.; Findling, R.L. Efficacy and Safety of Pediatric Prolonged-Release Melatonin for Insomnia in Children with Autism Spectrum Disorder. J. Am. Acad Child. Adolesc. Psychiatry 2017, 56, 948–957.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gringras, P.; Gamble, C.; Jones, A.P.; Wiggs, L.; Williamson, P.R.; Sutcliffe, A.; Montgomery, P.; Whitehouse, W.P.; Choonara, I.; Allport, T.; et al. Melatonin for sleep problems in children with neurodevelopmental disorders: Randomised double masked placebo controlled trial. BMJ 2012, 345, e6664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortesi, F.; Giannotti, F.; Sebastiani, T.; Panunzi, S.; Valente, D. Controlled-release melatonin, singly and combined with cognitive behavioural therapy, for persistent insomnia in children with autism spectrum disorders: A randomized placebo-controlled trial. J. Sleep Res. 2012, 21, 700–709. [Google Scholar] [CrossRef]
- Garstang, J.; Wallis, M. Randomized controlled trial of melatonin for children with autistic spectrum disorders and sleep problems. Child. Care Health Dev. 2006, 32, 585–589. [Google Scholar] [CrossRef]
- Wright, B.; Sims, D.; Smart, S.; Alwazeer, A.; Alderson-Day, B.; Allgar, V.; Whitton, C.; Tomlinson, H.; Bennett, S.; Jardine, J.; et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: A randomised controlled crossover trial. J. Autism Dev. Disord. 2011, 41, 175–184. [Google Scholar] [CrossRef]
- Hardan, A.Y.; Fung, L.K.; Libove, R.A.; Obukhanych, T.V.; Nair, S.; Herzenberg, L.A.; Frazier, T.W.; Tirouvanziam, R. A randomized controlled pilot trial of oral N-acetylcysteine in children with autism. Biol. Psychiatry 2012, 71, 956–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanizadeh, A.; Moghimi-Sarani, E. A randomized double blind placebo controlled clinical trial of N-Acetylcysteine added to risperidone for treating autistic disorders. BMC Psychiatry 2013, 13, 196. [Google Scholar] [CrossRef] [Green Version]
- Nikoo, M.; Radnia, H.; Farokhnia, M.; Mohammadi, M.R.; Akhondzadeh, S. N-acetylcysteine as an adjunctive therapy to risperidone for treatment of irritability in autism: A randomized, double-blind, placebo-controlled clinical trial of efficacy and safety. Clin. Neuropharmacol. 2015, 38, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Amminger, G.P.; Berger, G.E.; Schafer, M.R.; Klier, C.; Friedrich, M.H.; Feucht, M. Omega-3 fatty acids supplementation in children with autism: A double-blind randomized, placebo-controlled pilot study. Biol. Psychiatry 2007, 61, 551–553. [Google Scholar] [CrossRef] [PubMed]
- Parellada, M.; Llorente, C.; Calvo, R.; Gutierrez, S.; Lazaro, L.; Graell, M.; Guisasola, M.; Dorado, M.L.; Boada, L.; Romo, J.; et al. Randomized trial of omega-3 for autism spectrum disorders: Effect on cell membrane composition and behavior. Eur. Neuropsychopharmacol. 2017, 27, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Dolske, M.C.; Spollen, J.; McKay, S.; Lancashire, E.; Tolbert, L. A preliminary trial of ascorbic acid as supplemental therapy for autism. Prog. Neuropsychopharmacol. Biol. Psychiatry 1993, 17, 765–774. [Google Scholar] [CrossRef]
- Li, B.; Xu, Y.; Zhang, X.; Zhang, L.; Wu, Y.; Wang, X.; Zhu, C. The effect of vitamin D supplementation in treatment of children with autism spectrum disorder: A systematic review and meta-analysis of randomized controlled trials. Nutr. Neurosci. 2020, 1–11. [Google Scholar] [CrossRef]
- Song, L.; Luo, X.; Jiang, Q.; Chen, Z.; Zhou, L.; Wang, D.; Chen, A. Vitamin D Supplementation is Beneficial for Children with Autism Spectrum Disorder: A Meta-analysis. Clin. Psychopharmacol. Neurosci. 2020, 18, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.B.; George, F.; Audhya, T. Abnormally high plasma levels of vitamin B6 in children with autism not taking supplements compared to controls not taking supplements. J. Altern. Complement. Med. 2006, 12, 59–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiffer, S.I.; Norton, J.; Nelson, L.; Shott, S. Efficacy of vitamin B6 and magnesium in the treatment of autism: A methodology review and summary of outcomes. J. Autism Dev. Disord. 1995, 25, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Ezugha, H.; Goldenthal, M.; Valencia, I.; Anderson, C.E.; Legido, A.; Marks, H. 5q14.3 deletion manifesting as mitochondrial disease and autism: Case report. J. Child. Neurol. 2010, 25, 1232–1235. [Google Scholar] [CrossRef] [PubMed]
- Guevara-Campos, J.; Gonzalez-Guevara, L.; Guevara-Gonzalez, J.; Cauli, O. First Case Report of Primary Carnitine Deficiency Manifested as Intellectual Disability and Autism Spectrum Disorder. Brain Sci. 2019, 9, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benke, P.J.; Duchowny, M.; McKnight, D. Biotin and Acetazolamide for Treatment of an Unusual Child with Autism Plus Lack of Nail and Hair Growth. Pediatr. Neurol. 2018, 79, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Zou, M.; Zhao, D.; Xia, W.; Wu, L. Efficacy of Folic Acid Supplementation in Autistic Children Participating in Structured Teaching: An Open-Label Trial. Nutrients 2016, 8, 337. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.S.; Sze, S.L.; Han, Y.M.Y. An intranasal herbal medicine improves executive functions and activates the underlying neural network in children with autism. Res. Autism Spectr. Disord. 2014, 8, 681–691. [Google Scholar] [CrossRef] [Green Version]
- Kern, J.K.; Geier, D.A.; Adams, J.B.; Garver, C.R.; Audhya, T.; Geier, M.R. A clinical trial of glutathione supplementation in autism spectrum disorders. Med. Sci. Monit. 2011, 17, CR677–CR682. [Google Scholar] [CrossRef]
- Dosman, C.F.; Brian, J.A.; Drmic, I.E.; Senthilselvan, A.; Harford, M.M.; Smith, R.W.; Sharieff, W.; Zlotkin, S.H.; Moldofsky, H.; Roberts, S.W. Children with autism: Effect of iron supplementation on sleep and ferritin. Pediatr. Neurol. 2007, 36, 152–158. [Google Scholar] [CrossRef]
- Guo, M.; Zhu, J.; Yang, T.; Lai, X.; Liu, X.; Liu, J.; Chen, J.; Li, T. Vitamin A improves the symptoms of autism spectrum disorders and decreases 5-hydroxytryptamine (5-HT): A pilot study. Brain Res. Bull. 2018, 137, 35–40. [Google Scholar] [CrossRef]
- Meguid, N.A.; Bjorklund, G.; Gebril, O.H.; Dosa, M.D.; Anwar, M.; Elsaeid, A.; Gaber, A.; Chirumbolo, S. The role of zinc supplementation on the metallothionein system in children with autism spectrum disorder. Acta Neurol. Belg. 2019, 119, 577–583. [Google Scholar] [CrossRef]
- Russo, A.J. Increased Copper in Individuals with Autism Normalizes Post Zinc Therapy More Efficiently in Individuals with Concurrent GI Disease. Nutr. Metab. Insights 2011, 4, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, M. Oxidative stress, metabolic and mitochondrial abnormalities associated with autism spectrum disorder. Prog. Mol. Biol. Transl. Sci. 2020, 173, 331–354. [Google Scholar] [CrossRef]
- Delhey, L.M.; Nur Kilinc, E.; Yin, L.; Slattery, J.C.; Tippett, M.L.; Rose, S.; Bennuri, S.C.; Kahler, S.G.; Damle, S.; Legido, A.; et al. The Effect of Mitochondrial Supplements on Mitochondrial Activity in Children with Autism Spectrum Disorder. J. Clin. Med. 2017, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossignol, D.A.; Frye, R.E. Psychotropic Medications for Sleep Disorders in Autism Spectrum Disorders. In Handbook of Autism and Pervasive Developmental Disorder; Matson, J.L., Sturmey, P., Eds.; Spring Publishing: Berlin/Heidelberg, Germany, 2020; in press. [Google Scholar]
- Frye, R.E.; Sequeira, J.M.; Quadros, E.V.; James, S.J.; Rossignol, D.A. Cerebral folate receptor autoantibodies in autism spectrum disorder. Mol. Psychiatry 2013, 18, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Ramaekers, V.T.; Blau, N.; Sequeira, J.M.; Nassogne, M.C.; Quadros, E.V. Folate receptor autoimmunity and cerebral folate deficiency in low-functioning autism with neurological deficits. Neuropediatrics 2007, 38, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Bjorklund, G.; Tinkov, A.A.; Hosnedlova, B.; Kizek, R.; Ajsuvakova, O.P.; Chirumbolo, S.; Skalnaya, M.G.; Peana, M.; Dadar, M.; El-Ansary, A.; et al. The role of glutathione redox imbalance in autism spectrum disorder: A review. Free Radic. Biol. Med. 2020, 160, 149–162. [Google Scholar] [CrossRef]
- Howsmon, D.P.; Vargason, T.; Rubin, R.A.; Delhey, L.; Tippett, M.; Rose, S.; Bennuri, S.C.; Slattery, J.C.; Melnyk, S.; James, S.J.; et al. Multivariate techniques enable a biochemical classification of children with autism spectrum disorder versus typically-developing peers: A comparison and validation study. Bioeng. Transl. Med. 2018, 3, 156–165. [Google Scholar] [CrossRef]
- Frye, R.E.; Melnyk, S.; Fuchs, G.; Reid, T.; Jernigan, S.; Pavliv, O.; Hubanks, A.; Gaylor, D.W.; Walters, L.; James, S.J. Effectiveness of methylcobalamin and folinic Acid treatment on adaptive behavior in children with autistic disorder is related to glutathione redox status. Autism Res. Treat. 2013, 2013, 609705. [Google Scholar] [CrossRef]
- James, S.J.; Melnyk, S.; Fuchs, G.; Reid, T.; Jernigan, S.; Pavliv, O.; Hubanks, A.; Gaylor, D.W. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am. J. Clin. Nutr. 2009, 89, 425–430. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Benefited Symptom Options | Adverse Symptom Options |
|---|---|
| General benefit, no one particular symptom | General worsening, no one specific symptom |
| Aggression/Agitation | Aggression/Agitation |
| Anxiety | Anxiety |
| Attention | Bedwetting/Bladder Control |
| Cognition (ability to think) | Behavior problems |
| Constipation | Decreased cognition (difficulty thinking/remembering) |
| Depression | Depression |
| Diarrhea | Dizziness/Unsteadiness |
| Eczema/Skin problem | Dry mouth |
| Health (fewer illnesses and/or less severe illnesses) | Fatigue/Drowsiness |
| Hyperactivity | Gastrointestinal problems |
| Irritability | Headache/Migraine |
| Language/Communication | Hyperactivity |
| Lethargy (easily tired) | Irritability |
| OCD | Liver/Kidney problem |
| Reflux/Vomiting | Loss of appetite |
| Seizures | Nausea |
| Self-Injury | Rash |
| Sensory Sensitivity | Seizures |
| Sleep (falling asleep) | Self-injury |
| Sleep (staying asleep) | Sleep Problems |
| Social Interaction and Understanding | Stimming/Perseveration/Desire for Sameness |
| Stimming/Perseveration/Desire for Sameness | Tics/Abnormal movements |
| Tics/Abnormal movements | Weight gain |
| Weight loss |
| N | % | |
|---|---|---|
| Survey Completed By | ||
| Primary Caregiver of an Individual with Autism | 1094 | 85% |
| Adult with High-Functioning Autism 18 years or older who does not have a guardianship | 89 | 7% |
| Adult with Autism with their Mother/Father/Childhood Guardian | 39 | 3% |
| Grandparent of an Individual with Autism 1 | 58 | 5% |
| Other | 6 | 0% |
| Age of Participant | ||
| Child (under 13 years old) | 692 | 54% |
| Teenager (13–17 years old) | 274 | 21% |
| Young Adult (18–30 years old) | 202 | 16% |
| Adult (over 30 years old) | 116 | 9% |
| Gender of Participant | ||
| Male | 973 | 76% |
| Female | 305 | 24% |
| Other | 5 | 0% |
| Current Medical Diagnosis | ||
| Autism | 548 | 43% |
| Asperger’s Syndrome | 186 | 14% |
| Autism Spectrum Disorder | 289 | 22% |
| High-Functioning Autism | 148 | 12% |
| Pervasive Developmental Disorder—Not Otherwise Specified (PDD-NOS) | 76 | 6% |
| No current diagnosis, but he/she was on the autism spectrum previously | 18 | 1% |
| Other | 21 | 2% |
| Developmental History | ||
| Abnormal development from early infancy, with no major regression or plateau in development | 410 | 32% |
| Normal development, followed by a plateau in development that lasted for several months or longer | 284 | 22% |
| Normal development, followed by major regression | 278 | 22% |
| Normal development, followed by a major regression and a plateau lasting several months or longer | 168 | 13% |
| Other | 127 | 10% |
| Number of Rounds of Antibiotics during the first three years of life | ||
| Average | 9.3 | |
| Median | 3.0 | |
| None | 148 | 14% |
| 1 Round | 183 | 17% |
| 2 Rounds | 138 | 13% |
| 3 Rounds | 163 | 15% |
| 4 Rounds | 67 | 6% |
| 5 Rounds | 63 | 6% |
| 6–7 Rounds | 79 | 7% |
| 8–10 Rounds | 90 | 8% |
| 11–15 Rounds | 35 | 3% |
| 16–20 Rounds | 22 | 2% |
| 21+ Rounds | 84 | 8% |
| Severity of autism-related symptoms at age 3 | ||
| No autistic symptoms | 50 | 4% |
| Nearly normal, with only very mild symptoms | 227 | 18% |
| Mild autism | 290 | 23% |
| Moderate autism | 474 | 38% |
| Severe autism | 222 | 18% |
| Severity of autism-related symptoms currently | ||
| No autistic symptoms | 14 | 1% |
| Nearly normal, with only very mild symptoms | 200 | 16% |
| Mild autism | 390 | 31% |
| Moderate autism | 475 | 38% |
| Severe autism | 186 | 15% |
| Symptoms | Nutraceuticals (Overall Net Benefit Rating) |
|---|---|
| General benefit, no one particular symptom | Fruit/Vegetable Powder Concentrate (1.49), Potassium (1.30), Omega 6 (1.18), Vitamin C (1.05), Vitamin D (1.00), CoQ10 (1.00), High Dose Folinic Acid (1.00), Chromium (0.97), Vitamin E (0.95), Iodine (0.95), General Glutathione (0.92), Moderate Dose Folinic acid (0.92), High Dose Multivitamin (0.91), Folic Acid (0.89), Vitamin B1 (0.85), Vitamin A (not as cod liver oil) (0.85), High Dose Multivitamin for Children/Adults with ASD (0.83), Vitamin B2 (0.81), Vitamin B3 (0.78), Blend of Amino Acids (0.77), Calcium (0.76), Vitamin A (as cod liver oil) (0.75), Zinc (0.74), Generic Child/Adult Multivitamin (0.75), Omega 3 (0.74), Selenium (0.74), Vitamin B5 (0.72), Iron (0.69), Milk Thistle (0.66), Magnesium (0.66), Krill Oil (0.66), Vitamin K (0.65), PSP (0.64), Oral Vitamin B12 (0.64), Evening Primrose Oil (0.63), Oral Glutathione (0.62), Lithium (0.60), Biotin (0.60), Cod Liver Oil (0.55), Flax Seed Oil (0.52), Medium Dose Vitamin B6 (0.52), Oral NAC (0.51), Fish Oil (0.49), Carnitine (0.49), Injected Vitamin B12 (0.48), Taurine (0.47), 5-HTP (0.46), Transdermal Glutathione (0.44), Epsom Salt (0.34), DMG (0.30), GABA (0.25) |
| Sleep (falling asleep) | Melatonin (1.33), 5-HTP (0.61), Tryptophan (0.45), Valerian Root (0.44), Magnesium (0.21) |
| Cognition | High Dose Folinic Acid (0.63), Omega 6 (0.53), Cod Liver Oil (0.43), Omega 3 (0.43), Injected Vitamin B12 (0.42), Oral Vitamin B12 (0.40), Fish Oil (0.39), High Dose Multivitamin for Children/Adults with ASD (0.35), CoQ10 (0.26), High Dose Multivitamin (0.23), Lithium (0.22), Krill Oil (0.21), Moderate Dose Folinic Acid (0.20) |
| Sleep (staying asleep) | Melatonin (0.63), 5-HTP (0.46), Tryptophan (0.32), Valerian Root (0.24) |
| Aggression/Agitation | Epsom Salt (0.54), Lithium (0.22), Magnesium (0.20) |
| Attention | High Dose Folinic Acid (0.54), Omega 6 (0.50), Epsom Salt (0.41), High Dose Multivitamin for Children/Adults with ASD (0.32), Cod Liver Oil (0.30), Omega 3 (0.29), Evening Primrose Oil (0.28), PSP (0.26), Oral Vitamin B12 (0.26), Fish Oil (0.21) |
| Language/Communication | High Dose Folinic Acid (0.45), Injected Vitamin B12 (0.45), Moderate Dose Folinic Acid (0.33), Omega 6 (0.32), General Glutathione (0.32), Oral Vitamin B12 (0.30), Cod Liver Oil (0.25), Omega 3 (0.25), Epsom Salt (0.24), High Dose Multivitamin (0.23), High Dose Multivitamin for Children/Adults with ASD (0.22), Fish Oil (0.21), TMG (0.20) |
| Constipation | Fruit/Vegetable Powder Concentrate (0.53), Magnesium (0.48), Vitamin C (0.22) |
| Health (fewer illnesses and/or less severe illnesses) | Fruit/Vegetable Powder Concentrate (0.53), Vitamin C (0.51), High Dose Multivitamin (0.45), Vitamin D (0.34), Potassium (0.33), Zinc (0.31), High Dose Multivitamin for Children/Adults with ASD (0.29), Vitamin E (0.23) |
| Anxiety | Lithium (0.37), Magnesium (0.33), PSP (0.32), GABA (0.27), Tryptophan (0.26), High Dose Multivitamin for Children/Adults with ASD (0.22) |
| Social Interaction and Understanding | High Dose Folinic Acid (0.36), General Glutathione (0.26), Moderate Dose Folinic Acid (0.26), High Dose Multivitamin for Children/Adults with ASD (0.26), Injected Vitamin B12 (0.26), High Dose Multivitamin (0.23), Oral Vitamin B12 (0.22) |
| Irritability | High Dose Folinic Acid (0.27), Magnesium (0.26), Epsom Salt (0.23), High Dose Multivitamin for Children/Adults with ASD (0.22) |
| Sensory Sensitivity | High Dose Multivitamin for Children/Adults with ASD (0.22), Lithium (0.15), Injected Vitamin B12 (0.12) |
| Lethargy (easily tired) | Carnitine (0.21), Chromium (0.19), Injected Vitamin B12 (0.15) |
| Depression | Epsom Salt (0.18), Tryptophan (0.13), Vitamin D (0.11) |
| Hyperactivity | High Dose Folinic Acid (0.18), High Dose Multivitamin for Children/Adults with ASD (0.13), Magnesium (0.12) |
| Stimming/Perseveration/Desire for Sameness | Evening Primrose Oil (0.14), High Dose Multivitamin for Children/Adults with ASD (0.13), Tryptophan (0.13) |
| OCD | PSP (0.13), Vitamin B3 (0.10), High Dose Folinic Acid (0.09) |
| Tics/involuntary movements | Tryptophan (0.13), Potassium (0.08), High Dose Multivitamin (0.08) |
| Eczema/Skin problems | Biotin (0.12), Vitamin E (0.08), Vitamin D (0.07) |
| Diarrhea | Fruit/Vegetable Powder Concentrate (0.11), Glutamine (0.08), High Dose Multivitamin for Children/Adults with ASD (0.06) |
| Seizures | High Dose Folinic Acid (0.09), Moderate Dose Folinic Acid (0.07), Oral Vitamin B12 (0.01) |
| Self-Injurious behaviors | High Dose Folinic Acid (0.09), Oral Glutathione (0.07), High Dose Multivitamin for Children/Adults with ASD (0.06) |
| Reflux/Vomiting | Epsom Salt (0.06), Milk Thistle (0.05), Vitamin E (0.04) |
| Percentage of Responses | |
|---|---|
| Much Better (3) | 27% |
| Somewhat Better (2) | 26% |
| Slightly Better (1) | 24% |
| No Effect (0) | 23% |
| Mildly Worse (−1) | 0% |
| Somewhat Worse (−2) | 0% |
| Much Worse (−3) | 0% |
| Average | 1.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adams, J.B.; Bhargava, A.; Coleman, D.M.; Frye, R.E.; Rossignol, D.A. Ratings of the Effectiveness of Nutraceuticals for Autism Spectrum Disorders: Results of a National Survey. J. Pers. Med. 2021, 11, 878. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090878
Adams JB, Bhargava A, Coleman DM, Frye RE, Rossignol DA. Ratings of the Effectiveness of Nutraceuticals for Autism Spectrum Disorders: Results of a National Survey. Journal of Personalized Medicine. 2021; 11(9):878. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090878
Chicago/Turabian StyleAdams, James B., Anisha Bhargava, Devon M. Coleman, Richard E. Frye, and Daniel A. Rossignol. 2021. "Ratings of the Effectiveness of Nutraceuticals for Autism Spectrum Disorders: Results of a National Survey" Journal of Personalized Medicine 11, no. 9: 878. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11090878