
Rhythm Control Better Prevents Dementia than Rate Control Strategies in Patients with Atrial Fibrillation—A Nationwide Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Database
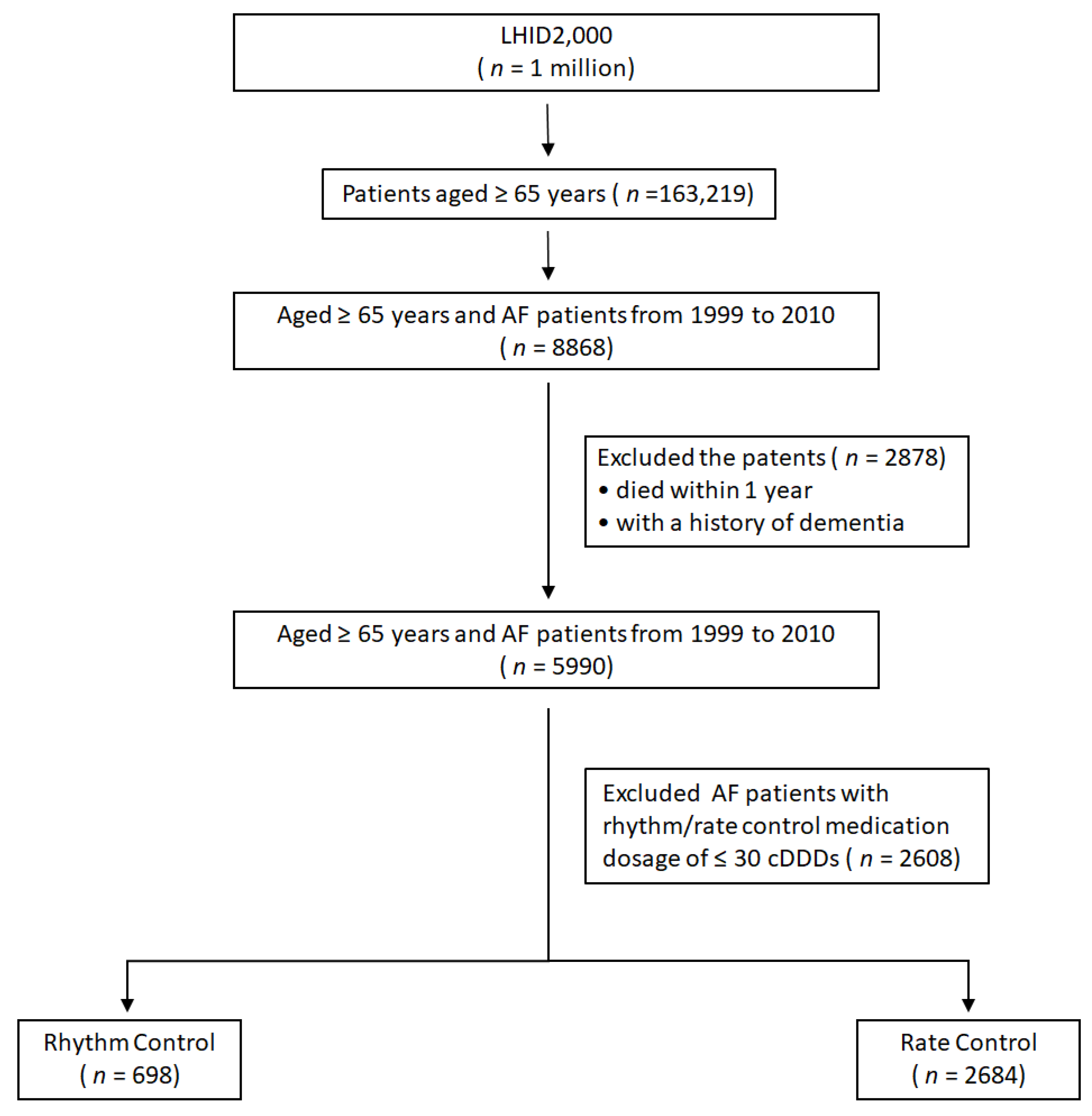
2.2. Study Population
2.3. Definitions of Rhythm Versus Rate Control Strategies
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. AF Control Strategies and Factors on Dementia Risk
3.3. Subgroup Strategy Analysis on Dementia Outcomes
3.4. Matched Cohort
4. Discussion
4.1. Risk Factors for Dementia in AF Patients
4.2. Rhythm Versus Rate Control on Dementia Risk
4.3. Aspirin Use on Dementia Risk in Patients with AF
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahathevan, R.; Brodtmann, A.; Donnan, G.A. Dementia, stroke, and vascular risk factors: A review. Int. J. Stroke 2012, 7, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Udompanich, S.; Lip, G.Y.; Apostolakis, S.; Lane, D.A. Atrial fibrillation as a risk factor for cognitive impairment: A semi-systematic review. QJM 2013, 106, 795–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopard, R.; Piazza, G.; Gale, S.A.; Campia, U.; Albertsen, I.E.; Kim, J.; Goldhaber, S.Z. Dementia and Atrial Fibrillation: Pathophysiological Mechanisms and Therapeutic Implications. Am. J. Med. 2018, 131, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.C.; Chen, Y.Y.; Chien, K.L.; Chung, F.P.; Lo, L.W.; Chang, S.L.; Chao, T.F.; Hu, Y.F.; Lin, C.Y.; Tuan, T.C.; et al. Catheter ablation of atrial fibrillation reduces the risk of dementia and hospitalization during a very long-term follow-up. Int. J. Cardiol. 2020, 304, 75–81. [Google Scholar] [CrossRef]
- Bunch, T.J.; Crandall, B.G.; Weiss, J.P.; May, H.T.; Bair, T.L.; Osborn, J.S.; Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Lappe, D.L.; et al. Patients treated with catheter ablation for atrial fibrillation have long-term rates of death, stroke, and dementia similar to patients without atrial fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 839–845. [Google Scholar] [CrossRef]
- Lankveld, T.A.R.; Vernooy, K.; Crijns, H.; Linz, D. How to make catheter ablation available world-wide? Int. J. Cardiol. Heart Vasc. 2019, 24, 100411. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Chung, M.K.; Shemanski, L.; Sherman, D.G.; Greene, H.L.; Hogan, D.B.; Kellen, J.C.; Kim, S.G.; Martin, L.W.; Rosenberg, Y.; Wyse, D.G.; et al. Functional status in rate- versus rhythm-control strategies for atrial fibrillation: Results of the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Functional Status Substudy. J. Am. Coll. Cardiol. 2005, 46, 1891–1899. [Google Scholar] [CrossRef] [Green Version]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef]
- Weng, C.-J.; Li, C.-H.; Liao, Y.-C.; Lin, C.-C.; Lin, J.-C.; Chang, S.-L.; Lo, C.-P.; Huang, K.-C.; Huang, J.-L.; Lin, C.-H. Rhythm control better prevents stroke and mortality than rate control strategies in patients with atrial fibrillation-A nationwide cohort study. Int. J. Cardiol. 2018, 270, 154–159. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Liao, Y.C.; Li, C.H.; Lin, J.C.; Weng, C.J.; Lin, C.C.; Lo, C.P.; Huang, K.C.; Huang, J.L. Lin CH. Hypoglycaemic episodes increase the risk of ventricular arrhythmia and sudden cardiac arrest in patients with type 2 diabetes—A nationwide cohort study. Diabetes/Metab. Res. Rev. 2020, 36, e3226. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-H.; Lee, Y.-C.; Tsai, C.-T.; Chang, S.-N.; Chung, Y.-H.; Lin, M.-S.; Lin, J.-W.; Lai, M.-S. Continuation of statin therapy and a decreased risk of atrial fibrillation/flutter in patients with and without chronic kidney disease. Atherosclerosis 2014, 232, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, V.; Cutler, M.J.; Day, J.D.; Bunch, T.J. Atrial fibrillation and dementia. Trends Cardiovasc. Med. 2015, 25, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Saglietto, A.; Matta, M.; Gaita, F.; Jacobs, V.; Bunch, T.J.; Anselmino, M. Stroke-independent contribution of atrial fibrillation to dementia: A meta-analysis. Arch. Dis. Child. 2019, 6, e000984. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Ganguli, M. Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wändell, P.; Carlsson, A.C.; Sundquist, J.; Sundquist, K. The association between relevant comorbidities and dementia in patients with atrial fibrillation. Geroscience 2018, 40, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Bellomo, A.; De Benedetto, G.; Fossati, C.; D’Ottavio, E.; Formosa, V.; Gianturco, V.; Iori, A.; Marigliano, B.; Lo Iacono, C.; Troisi, G.; et al. Atrial fibrillation (AF) and cognitive impairment in the elderly: A case-control study. Arch. Gerontol. Geriatr. 2012, 55, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Rokita, H.; Launer, L.J.; Gudnason, V.; Arnar, D.O. Atrial fibrillation is associated with decreased total cerebral blood flow and brain perfusion. Europace 2018, 20, 1252–1258. [Google Scholar] [CrossRef]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Gardarsdottir, V.A.; Forsberg, L.; Gudnason, V.; Arnar, D.O. Improved brain perfusion after electrical cardioversion of atrial fibrillation. Europace 2020, 22, 530–537. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Canova, D.; Roatta, S.; Gianotto, N.; Piccotti, A.; Franzin, S.; Gaita, F.; De Ferrari, G.M.; Ridolfi, L.; et al. Increased beat-to-beat variability of cerebral microcirculatory perfusion during atrial fibrillation: A near-infrared spectroscopy study. Europace 2021, 23, 1219–1226. [Google Scholar] [CrossRef]
- Niu, H.; Álvarez-Álvarez, I.; Guillén-Grima, F.; Aguinaga-Ontoso, I. Prevalence and incidence of Alzheimer’s disease in Europe: A meta-analysis. Neurología 2017, 32, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Maggi, S.; Thompson, T.; Schofield, P.; Muller, C.; Tseng, P.T.; Lin, P.Y.; Carvalho, A.F.; Solmi, M. Low-dose aspirin use and cognitive function in older age: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2017, 65, 1763–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boos, C.J. Infection and atrial fibrillation: Inflammation begets AF. Eur. Heart J. 2020, 41, 1120–1122. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.N.; Chao, T.F.; Liu, C.J.; Wang, K.L.; Chen, S.J.; Tuan, T.C.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; et al. Risk and prediction of dementia in patients with atrial fibrillation—A nationwide population-based cohort study. Int. J. Cardiol. 2015, 199, 25–30. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Rhythm Control | Rate Control | p-Value |
|---|---|---|---|
| N = 698 | N = 2684 | ||
| Age, mean (SD) | 75.1 (6.2) | 75.9 (6.7) | 0.003 * |
| ≥75 (%) | 362 (51.9) | 1489 (55.5) | 0.09 |
| Male (%) | 398 (57.0) | 1425 (53.1) | 0.06 |
| Co-morbidity (%) | |||
| Hypertension | 563 (80.7) | 2303 (85.8) | 0.0008 |
| Diabetes | 216 (30.9) | 879 (32.7) | 0.36 |
| Heart failure | 214 (30.7) | 1186 (44.2) | <0.0001 |
| Stroke | 271 (38.8) | 1095 (40.8) | 0.34 |
| VHD | 165 (23.6) | 663 (24.7) | 0.56 |
| CAD | 478 (68.5) | 1925 (71.7) | 0.09 |
| COPD | 403 (57.7) | 1581 (58.9) | 0.58 |
| Depression | 49 (7.0) | 173 (6.4) | 0.59 |
| ** Propensity score | 0.22 (0.05) | 0.20 (0.05) | <0.001 |
| Medications (%) | |||
| ACEIs/ARBs | 427 (61.2) | 1812 (67.5) | 0.0016 |
| Alpha blockers | 147 (21.1) | 518 (19.3) | 0.3 |
| Diuretics | 379 (54.3) | 1831 (68.2) | <0.0001 |
| Aspirin | 479 (68.6) | 1953 (72.8) | 0.03 |
| Clopidogrel | 116 (16.6) | 332 (12.4) | 0.0032 |
| Warfarin | 108 (15.5) | 526 (19.6) | 0.01 |
| Statins | 131 (18.8) | 394 (14.7) | 0.0079 |
| Fibrates | 28 (4.01) | 117 (4.36) | 0.69 |
| Catheter ablation for AF (%) | 7 (0.26) | 4 (0.57) | 0.197 |
| Electrical cardioversion (%) | 9 (1.3) | 20 (0.7) | 0.165 |
| Maze procedure (%) | 0 (0%) | 1 (0%) | - |
| Medications | Rhythm Control N = 698 | Rate Control N = 2684 | p-Value |
|---|---|---|---|
| Rate control (%) | |||
| β-Blocker | 299 (42.8) | 1700 (63.3) | <0.0001 |
| Diltiazem | 145 (20.8) | 1060 (39.5) | <0.0001 |
| Verapamil | 62 (8.9) | 405 (15.1) | <0.0001 |
| Digoxin | 182 (26.1) | 1860 (69.3) | <0.0001 |
| Rhythm control (%) | |||
| Quinidine | 4 (0.57) | ||
| Flecainide | 4 (0.57) | ||
| Propafenone | 255 (36.5) | ||
| Amiodarone | 540 (77.4) | ||
| Sotalol | 6 (0.86) |
| Variable | Event | PYs | Event Rate | Crude HR (95% CI) | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| AF control strategy | ||||||
| Rate control | 347 | 12,936 | 26.8 | ref | ref | |
| Rhythm control | 67 | 3501 | 19.1 | 0.71 (0.55–0.92) | 0.75 (0.58–0.97) | 0.031 |
| Age | ||||||
| <75 | 155 | 9024 | 17.2 | ref | ref | |
| ≥75 | 259 | 7412 | 34.9 | 2.14 (1.75–2.62) | 1.72 (1.23–2.42) | 0.002 |
| Sex | ||||||
| Female | 227 | 7459 | 30.4 | ref | ref | |
| Male | 187 | 8977 | 20.8 | 0.68 (0.56–0.83) | 0.91 (0.58–1.42) | 0.667 |
| Hypertension | ||||||
| No | 53 | 2744 | 19.3 | ref | ref | |
| Yes | 361 | 13,693 | 26.4 | 1.38 (1.03–1.84) | 0.51 (0.13–2.03) | 0.339 |
| Diabetes | ||||||
| No | 280 | 11,423 | 24.5 | ref | ref | |
| Yes | 134 | 5014 | 26.7 | 1.10 (0.90–1.36) | 0.96 (0.78–1.19) | 0.706 |
| Heart failure | ||||||
| No | 251 | 10,423 | 24.1 | ref | ref | |
| Yes | 163 | 6014 | 27.1 | 1.15 (0.94–1.40) | 0.29 (0.03–2.5) | 0.262 |
| Stroke | ||||||
| No | 218 | 10,446 | 20.9 | ref | ref | |
| Yes | 196 | 5990 | 32.7 | 1.59 (1.31–1.93) | 1.25 (0.95–1.66) | 0.116 |
| VHD | ||||||
| No | 315 | 12,694 | 24.8 | ref | ref | |
| Yes | 99 | 3742 | 26.5 | 1.07 (0.86–1.35) | 1.23 (0.79–1.91) | 0.354 |
| CAD | ||||||
| No | 103 | 4742 | 21.7 | ref | ref | |
| Yes | 311 | 11,695 | 26.6 | 1.22 (0.98–1.53) | 0.99 (0.76–1.28) | 0.930 |
| COPD | ||||||
| No | 159 | 7059 | 22.5 | ref | ref | |
| Yes | 255 | 9378 | 27.2 | 1.21 (1.00–1.48) | 1.2 (0.94–1.54) | 0.142 |
| Depression | ||||||
| No | 372 | 15,473 | 24.0 | ref | ref | |
| Yes | 42 | 963 | 43.6 | 1.84 (1.34–2.53) | 2.22 (1.19–4.13) | 0.012 |
| Rate Control | Rhythm Control | Adjusted HR (95% CI) | p for Interaction | |||
|---|---|---|---|---|---|---|
| Variable | Event | Rate | Event | Rate | ||
| Age | 0.42 | |||||
| <75 | 131 | 18.7 | 24 | 12.0 | 0.65 (0.42–1.01) | |
| ≥75 | 216 | 36.5 | 43 | 28.7 | 0.79 (0.57–1.10) | |
| Sex | 0.18 | |||||
| Female | 197 | 33.0 | 30 | 20.0 | 0.63 (0.43–0.93) | |
| Male | 150 | 21.5 | 37 | 18.5 | 0.93 (0.65–1.34) | |
| Hypertension | 0.54 | |||||
| No | 40 | 20.0 | 13 | 17.5 | 0.91 (0.48–1.74) | |
| Yes | 307 | 28.1 | 54 | 19.6 | 0.74 (0.55–0.99) | |
| Diabetes | 0.11 | |||||
| No | 238 | 26.8 | 42 | 16.5 | 0.65 (0.47–0.90) | |
| Yes | 109 | 26.9 | 25 | 26.1 | 1.05 (0.68–1.63) | |
| Heart failure | 0.19 | |||||
| No | 199 | 25.3 | 52 | 20.3 | 0.90 (0.66–1.22) | |
| Yes | 148 | 29.2 | 15 | 15.9 | 0.54 (0.31–0.91) | |
| Stroke | 0.79 | |||||
| No | 183 | 22.3 | 35 | 15.5 | 0.76 (0.53–1.10) | |
| Yes | 164 | 34.6 | 32 | 25.7 | 0.80 (0.55–1.17) | |
| VHD | 0.66 | |||||
| No | 265 | 26.6 | 50 | 18.4 | 0.73 (0.54–0.99) | |
| Yes | 82 | 27.7 | 17 | 21.8 | 0.94 (0.55–1.60) | |
| CAD | 0.07 | |||||
| No | 78 | 21.6 | 25 | 22.3 | 1.12 (0.71–1.78) | |
| Yes | 269 | 28.9 | 42 | 17.7 | 0.65 (0.47–0.90) | |
| COPD | 0.76 | |||||
| No | 133 | 24.2 | 26 | 16.6 | 0.70 (0.46–1.07) | |
| Yes | 214 | 28.7 | 41 | 21.2 | 0.81 (0.58–1.14) | |
| Depression | 0.26 | |||||
| No | 314 | 25.8 | 58 | 17.6 | 0.73 (0.55–0.97) | |
| Yes | 33 | 43.2 | 9 | 45.2 | 1.27 (0.59–2.77) | |
| Aspirin | 0.03 | |||||
| No | 76 | 20.5 | 25 | 22.9 | 1.19 (0.75–1.87) | |
| Yes | 271 | 29.4 | 42 | 17.5 | 0.64 (0.46–0.89) | |
| Clopidogrel | 0.35 | |||||
| No | 318 | 27.3 | 62 | 20.5 | 0.80 (0.61–1.05) | |
| Yes | 29 | 22.7 | 5 | 10.6 | 0.63 (0.24–1.67) | |
| Warfarin | 0.89 | |||||
| No | 274 | 26.1 | 55 | 18.8 | 0.79 (0.59–1.06) | |
| Yes | 73 | 29.9 | 12 | 20.9 | 0.68 (0.36–1.25) | |
| ACEIs/ARBs | 0.19 | |||||
| No | 101 | 21.6 | 27 | 19.5 | 0.99 (0.64–1.52) | |
| Yes | 246 | 29.8 | 40 | 18.9 | 0.67 (0.48–0.94) | |
| Alpha blockers | 0.08 | |||||
| No | 272 | 25.9 | 57 | 20.7 | 0.86 (0.64–1.14) | |
| Yes | 75 | 30.9 | 10 | 13.4 | 0.48 (0.25–0.93) | |
| Diuretics | 0.07 | |||||
| No | 103 | 21.2 | 37 | 20.4 | 1.14 (0.78–1.68) | |
| Yes | 244 | 30.3 | 30 | 17.7 | 0.56 (0.39–0.83) | |
| Statins | 0.79 | |||||
| No | 310 | 28.0 | 58 | 19.9 | 0.76 (0.58–1.01) | |
| Yes | 37 | 19.7 | 9 | 15.3 | 0.74 (0.35–1.58) | |
| Fibrates | 0.83 | |||||
| No | 334 | 27.1 | 65 | 19.2 | 0.76 (0.58–0.99) | |
| Yes | 13 | 20.9 | 2 | 17.4 | 1.03 (0.2–5.3) | |
| Variables | Rhythm Control N = 698 (%) | Rate Control N = 698 (%) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 75.1 (6.2) | 75.1 (6.3) | 0.983 |
| ≥75 | 362 (51.9) | 362 (51.9) | 1.000 |
| Male | 398 (57.0) | 398 (57.0) | 1.000 |
| Co-morbidity | |||
| Hypertension | 563 (80.7) | 595 (85.2) | 0.023 |
| Diabetes | 216 (30.9) | 227 (32.5) | 0.527 |
| Heart failure | 214 (30.7) | 289 (41.4) | <0.001 |
| Stroke | 271 (38.8) | 282 (40.4) | 0.547 |
| VHD | 165 (23.6) | 176 (25.2) | 0.493 |
| CAD | 478 (68.5) | 512 (73.4) | 0.045 |
| COPD | 403 (57.7) | 408 (58.5) | 0.786 |
| Depression | 49 (7.0) | 36 (5.2) | 0.146 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.-C.; Li, C.-H.; Chen, Y.-Y.; Weng, C.-J.; Chien, Y.-S.; Wu, S.-J.; Lo, C.-P.; Tien, H.-C.; Lin, C.-H.; Huang, J.-L.; et al. Rhythm Control Better Prevents Dementia than Rate Control Strategies in Patients with Atrial Fibrillation—A Nationwide Cohort Study. J. Pers. Med. 2022, 12, 572. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040572
Lin J-C, Li C-H, Chen Y-Y, Weng C-J, Chien Y-S, Wu S-J, Lo C-P, Tien H-C, Lin C-H, Huang J-L, et al. Rhythm Control Better Prevents Dementia than Rate Control Strategies in Patients with Atrial Fibrillation—A Nationwide Cohort Study. Journal of Personalized Medicine. 2022; 12(4):572. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040572
Chicago/Turabian StyleLin, Jiunn-Cherng, Cheng-Hung Li, Yun-Yu Chen, Chi-Jen Weng, Yu-Shan Chien, Shang-Ju Wu, Chu-Pin Lo, Hui-Chun Tien, Ching-Heng Lin, Jin-Long Huang, and et al. 2022. "Rhythm Control Better Prevents Dementia than Rate Control Strategies in Patients with Atrial Fibrillation—A Nationwide Cohort Study" Journal of Personalized Medicine 12, no. 4: 572. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040572