
The Effect of Gout on Thyroid Cancer Incidence: A Nested Case-Control Study Using a National Health Screening Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
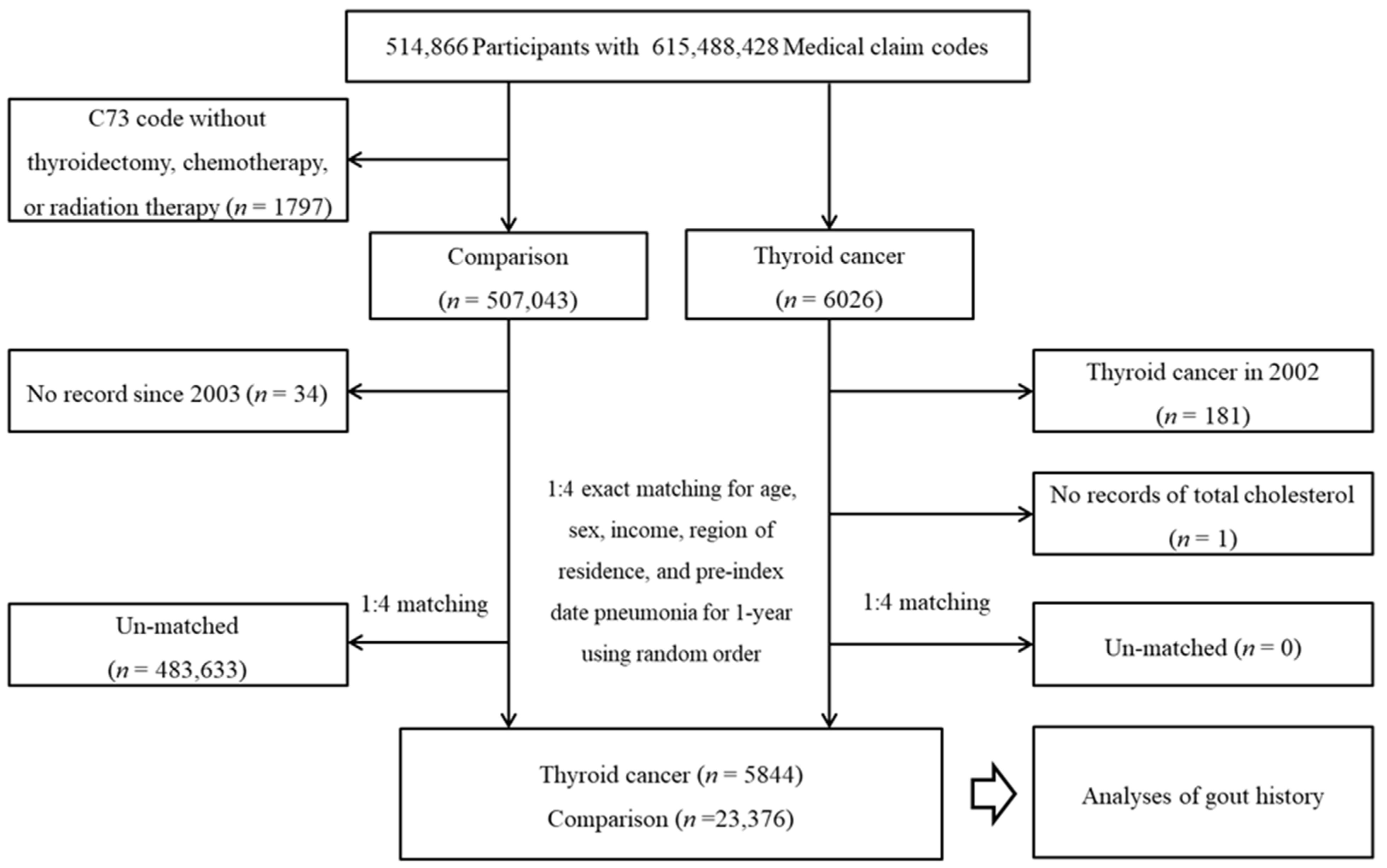
2.2. Participant Selection
2.3. Thyroid Cancer (Outcome)
2.4. Gout (Exposure)
2.5. Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wartofsky, L. Increasing world incidence of thyroid cancer: Increased detection or higher radiation exposure? Hormones 2010, 9, 103–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.S.; Kim, H.J.; Welch, H.G. Korea’s thyroid-cancer “epidemic”—Screening and overdiagnosis. N. Engl. J. Med. 2014, 371, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Myung, S.K.; Lee, C.W.; Lee, J.; Kim, J.; Kim, H.S. Risk Factors for Thyroid Cancer: A Hospital-Based Case-Control Study in Korean Adults. Cancer Res. Treat. 2017, 49, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Bogovic Crncic, T.; Ilic Tomas, M.; Girotto, N.; Grbac Ivankovic, S. Risk Factors for Thyroid Cancer: What Do We Know So Far? Acta Clin. Croat. 2020, 59 (Suppl. S1), 66–72. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Choi, M.; Kim, J.H.; Kim, J.; Han, K.; Kim, B.; Kim, D.H.; Park, Y.G. Metabolic Syndrome and the Risk of Thyroid Cancer: A Nationwide Population-Based Cohort Study. Thyroid 2020, 30, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Farkas, D.K.R.; Jorgensen, J.O.L.; Cronin-Fenton, D.; Sorensen, H.T. Benign Thyroid Diseases and Risk of Thyroid Cancer: A Nationwide Cohort Study. J. Clin. Endocrinol. Metab. 2018, 103, 2216–2224. [Google Scholar] [CrossRef]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef]
- Borghi, C.; Agabiti-Rosei, E.; Johnson, R.J.; Kielstein, J.T.; Lurbe, E.; Mancia, G.; Redon, J.; Stack, A.G.; Tsioufis, K.P. Hyperuricaemia and gout in cardiovascular, metabolic and kidney disease. Eur. J. Intern. Med. 2020, 80, 1–11. [Google Scholar] [CrossRef]
- Xu, J.; Wang, B.; Li, Q.; Yao, Q.; Jia, X.; Song, R.; Zhang, J.A. Risk of Thyroid Disorders in Patients with Gout and Hyperuricemia. Horm. Metab. Res. 2019, 51, 522–530. [Google Scholar] [CrossRef]
- Bruderer, S.G.; Meier, C.R.; Jick, S.S.; Bodmer, M. The association between thyroid disorders and incident gout: Population-based case-control study. Clin. Epidemiol. 2017, 9, 205–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.-J.; Do, C.-H.; Song, J.-S.; Lee, E.-J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.S.; Kim, K.S.; Kim, S.K.; Cho, Y.W.; Choi, H.G. Screening Leads to Overestimated Associations of Thyroid Dysfunction and Thyroiditis with Thyroid Cancer Risk. Cancers 2021, 13, 5385. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Min, C.; Yoo, D.M.; Chang, J.; Lee, H.J.; Park, B.; Choi, H.G. Hearing Impairment Increases Economic Inequality. Clin. Exp. Otorhinolaryngol. 2021, 14, 278–286. [Google Scholar] [CrossRef]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef]
- See, L.C.; Kuo, C.F.; Yu, K.H.; Luo, S.F.; Chou, I.J.; Ko, Y.S.; Chiou, M.-J.; Liu, J.-R. Hyperthyroid and hypothyroid status was strongly associated with gout and weakly associated with hyperuricaemia. PLoS ONE 2014, 9, e114579. [Google Scholar] [CrossRef]
- Mariani, L.H.; Berns, J.S. The renal manifestations of thyroid disease. J. Am. Soc. Nephrol. 2012, 23, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Blackburn, B.E.; Ganz, P.A.; Rowe, K.; Snyder, J.; Wan, Y.; Deshmukh, V.; Newman, M.; Fraser, A.; Smith, K.; et al. Risk Factors for Cardiovascular Disease Among Thyroid Cancer Survivors: Findings from the Utah Cancer Survivors Study. J. Clin. Endocrinol. Metab. 2018, 103, 2468–2477. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Slettebo Daltveit, D.; Ekbom, A.; Engeland, A.; Gissler, M.; Glimelius, I.; Grotmol, T.; Lagerros, Y.T.; Madanat-Harjuoja, L.; Männistö, T.; et al. Maternal health, in-utero, and perinatal exposures and risk of thyroid cancer in offspring: A Nordic population-based nested case-control study. Lancet Diabetes Endocrinol. 2021, 9, 94–105. [Google Scholar] [CrossRef]
- Vaccarella, S.; Dal Maso, L. Challenges in investigating risk factors for thyroid cancer. Lancet Diabetes Endocrinol. 2021, 9, 57–59. [Google Scholar] [CrossRef]
- Lamartina, L.; Grani, G.; Durante, C.; Filetti, S.; Cooper, D.S. Screening for differentiated thyroid cancer in selected populations. Lancet Diabetes Endocrinol. 2020, 8, 81–88. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| Thyroid Cancer (N = 5844) | Comparison (N = 23,376) | Standardized Difference | |
| Age (years old, n, %) | 0.00 | ||
| 40–44 | 127 (2.2) | 508 (2.2) | |
| 45–49 | 837 (14.3) | 3348 (14.3) | |
| 50–54 | 1593 (27.3) | 6372 (27.3) | |
| 55–59 | 1344 (23.0) | 5376 (23.0) | |
| 60–64 | 896 (15.3) | 3584 (15.3) | |
| 65–69 | 592 (10.1) | 2368 (10.1) | |
| 70–74 | 325 (5.6) | 1300 (5.6) | |
| 75–79 | 102 (1.8) | 408 (1.8) | |
| 80–84 | 27 (0.5) | 108 (0.5) | |
| ≥85 | 1 (0.0) | 4 (0.0) | |
| Sex (n, %) | 0.00 | ||
| Male | 1234 (21.1) | 4936 (21.1) | |
| Female | 4610 (78.9) | 18,440 (78.9) | |
| Income (n, %) | 0.00 | ||
| 1 (lowest) | 732 (12.5) | 2928 (12.5) | |
| 2 | 683 (11.7) | 2732 (11.7) | |
| 3 | 901 (15.4) | 3604 (15.4) | |
| 4 | 1195 (20.5) | 4780 (20.5) | |
| 5 (highest) | 2333 (39.9) | 9332 (39.9) | |
| Region of residence (n, %) | 0.00 | ||
| Urban | 2802 (48.0) | 11,208 (48.0) | |
| Rural | 3042 (52.1) | 12,168 (52.1) | |
| Total cholesterol level (mg/dL, mean, SD) | 198.7 (38.0) | 201.5 (37.7) | 0.08 |
| SBP (mmHg, mean, SD) | 124.4 (15.9) | 123.5 (16.1) | 0.05 |
| DBP (mmHg, mean, SD) | 77.5 (10.5) | 76.7 (10.5) | 0.08 |
| Fasting blood glucose level (mg/dL, mean, SD) | 97.2 (23.1) | 98.2 (26.1) | 0.04 |
| Obesity * (n, %) | 0.11 | ||
| Underweight | 79 (1.4) | 453 (1.9) | |
| Normal | 1936 (33.1) | 8772 (37.5) | |
| Overweight | 1654 (28.3) | 6370 (27.3) | |
| Obese I | 1936 (33.1) | 6998 (29.9) | |
| Obese II | 239 (4.1) | 783 (3.4) | |
| Smoking status (n, %) | 0.08 | ||
| Non-smoker | 5113 (87.5) | 20,053 (85.8) | |
| Past smoker | 392 (6.7) | 1474 (6.3) | |
| Current smoker | 339 (5.8) | 1849 (7.9) | |
| Alcohol consumption (n, %) | 0.01 | ||
| <1 time a week | 4576 (78.3) | 18,171 (77.7) | |
| ≥1 time a week | 1268 (21.7) | 5205 (22.3) | |
| CCI score † (score, n, %) | 0.41 | ||
| 0 | 3528 (60.4) | 18,201 (77.9) | |
| 1 | 941 (16.1) | 2840 (12.2) | |
| ≥2 | 1375 (23.5) | 2335 (10.0) | |
| Gout (n, %) | 116 (2.0) | 354 (1.5) | 0.04 |
| Characteristics | Thyroid Cancer | Comparison | OR (95% CIs) for Thyroid Cancer | |||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | (Exposure/Total, %) | Crude † | p-Value | Adjusted † ‡ | p-Value | |
| Total participants (n = 29,220) | 116/5844 (2.0) | 354/23,376 (1.5) | 1.32 (1.07–1.64) | 0.010 * | 1.24 (0.99–1.54) | 0.062 |
| Age | ||||||
| Age < 60 years old (n = 19,505) | 67/3901 (1.7) | 187/15,604 (1.2) | 1.45 (1.09–1.92) | 0.011 * | 1.36 (1.01–1.82) | 0.041 * |
| Age 60 years old (n = 9715) | 49/1943 (2.5) | 167/7772 (2.2) | 1.18 (0.85–1.64) | 0.314 | 1.11 (0.79–1.56) | 0.532 |
| Sex | ||||||
| Males (n = 6170) | 61/1234 (4.9) | 201/4936 (4.1) | 1.23 (0.91–1.65) | 0.174 | 1.15 (0.85–1.56) | 0.377 |
| Females (n = 23,050) | 55/4610 (1.2) | 153/18,440 (0.8) | 1.44 (1.06–1.97) | 0.020 * | 1.36 (0.99–1.87) | 0.062 |
| Income | ||||||
| Low income (n = 11,580) | 48/2316 (2.1) | 126/9264 (1.4) | 1.54 (1.10–2.17) | 0.012 * | 1.39 (0.98–1.98) | 0.067 |
| High income (n = 17,640) | 68/3528 (1.9) | 228/14,112 (1.6) | 1.20 (0.91–1.58) | 0.194 | 1.14 (0.86–1.52) | 0.375 |
| Region of residence | ||||||
| Urban (n = 14,010) | 47/2802 (1.7) | 155/11,208 (1.4) | 1.22 (0.88–1.70) | 0.240 | 1.12 (0.79–1.59) | 0.522 |
| Rural (n = 15,210) | 69/3042 (2.3) | 199/12,168 (1.6) | 1.41 (1.06–1.86) | 0.017 * | 1.32 (0.99–1.76) | 0.059 |
| Characteristics | Thyroid Cancer | Comparison | OR (95% CIs) for Thyroid Cancer | |||
|---|---|---|---|---|---|---|
| (Exposure/ Total, %) | (Exposure/Total, %) | Crude | p-Value | Adjusted † | p-Value | |
| Obesity | ||||||
| Underweight (n = 532) | 2/79 (2.5) | 2/453 (0.4) | 5.86 (0.81–42.25) | 0.079 | 6.70 (0.80–56.09) | 0.079 |
| Normal weight (n = 10,708) | 32/1936 (1.7) | 83/8772 (1.0) | 1.76 (1.17–2.65) | 0.007 * | 1.73 (1.13–2.66) | 0.013 * |
| Overweight (n = 8024) | 26/1654 (1.6) | 100/6370 (1.6) | 1.00 (0.65–1.55) | 1.000 | 1.03 (0.66–1.61) | 0.891 |
| Obese (n = 9956) | 56/2175 (2.6) | 169/7781 (2.2) | 1.19 (0.88–1.62) | 0.264 | 1.08 (0.79–1.49) | 0.621 |
| Smoking status | ||||||
| Non-smoker (n = 25,166) | 84/5113 (1.6) | 249/20,053 (1.2) | 1.33 (1.04–1.71) | 0.025 * | 1.20 (0.93–1.56) | 0.170 |
| Past or current smoker (n = 4054) | 32/731 (4.4) | 105/3323 (3.2) | 1.40 (0.94–2.10) | 0.100 | 1.38 (0.91–2.10) | 0.132 |
| Alcohol consumption | ||||||
| <1 time a week (n = 22,747) | 75/4576 (1.6) | 222/18171 (1.2) | 1.35 (1.04–1.75) | 0.027 * | 1.23 (0.93–1.62) | 0.144 |
| ≥1 time a week (n = 6473) | 41/1268 (3.2) | 132/5205 (2.5) | 1.28 (0.90–1.83) | 0.168 | 1.22 (0.84–1.78) | 0.290 |
| Total cholesterol (mg/dL) | ||||||
| <200 (n = 14,984) | 67/3160 (2.1) | 197/11,824 (1.7) | 1.28 (0.97–1.69) | 0.085 | 1.28 (0.95–1.72) | 0.100 |
| ≥200 to < 240 (n = 10,041) | 34/1893 (1.8) | 105/8148 (1.3) | 1.40 (0.95–2.07) | 0.090 | 1.33 (0.89–1.99) | 0.161 |
| ≥240 (n = 4195) | 15/791 (1.9) | 52/3404 (1.5) | 1.25 (0.70–2.23) | 0.457 | 0.96 (0.52–1.78) | 0.898 |
| Blood pressure (mmHg) | ||||||
| SBP < 140 and DBP < 90 (n = 23,458) | 89/4655 (1.9) | 256/18,803 (1.4) | 1.41 (1.11–1.80) | 0.005 * | 1.37 (1.07–1.76) | 0.014 * |
| SBP ≥ 140 or DBP ≥ 90 (n = 5762) | 27/1189 (2.3) | 98/4573 (2.1) | 1.06 (0.69–1.63) | 0.784 | 0.92 (0.58–1.45) | 0.709 |
| Fasting blood glucose (mg/dL) | ||||||
| <100 (n = 19,981) | 75/4040 (1.9) | 216/15,941 (1.4) | 1.38 (1.06–1.80) | 0.018 * | 1.26 (0.95–1.66) | 0.106 |
| ≥100 (n = 9239) | 41/1804 (2.3) | 138/7435 (1.9) | 1.23 (0.86–1.75) | 0.250 | 1.18 (0.81–1.70) | 0.389 |
| CCI score | ||||||
| 0 (n = 21,729) | 68/3528 (1.9) | 233/18,201 (1.3) | 1.52 (1.16–1.99) | 0.003 * | 1.48 (1.12–1.95) | 0.005 * |
| 1 (n = 3781) | 19/941 (2.0) | 47/2840 (1.7) | 1.23 (0.72–2.10) | 0.460 | 1.19 (0.69–2.05) | 0.544 |
| ≥2 (n = 3710) | 29/1375 (2.1) | 74/2335 (3.2) | 0.66 (0.43–1.02) | 0.060 | 0.85 (0.53–1.36) | 0.504 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Yoo, D.M.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Bang, W.J.; Kim, S.K.; Choi, H.G. The Effect of Gout on Thyroid Cancer Incidence: A Nested Case-Control Study Using a National Health Screening Cohort. J. Pers. Med. 2022, 12, 887. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060887
Kim SY, Yoo DM, Kwon MJ, Kim JH, Kim J-H, Bang WJ, Kim SK, Choi HG. The Effect of Gout on Thyroid Cancer Incidence: A Nested Case-Control Study Using a National Health Screening Cohort. Journal of Personalized Medicine. 2022; 12(6):887. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060887
Chicago/Turabian StyleKim, So Young, Dae Myoung Yoo, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, Woo Jin Bang, Sung Kyun Kim, and Hyo Geun Choi. 2022. "The Effect of Gout on Thyroid Cancer Incidence: A Nested Case-Control Study Using a National Health Screening Cohort" Journal of Personalized Medicine 12, no. 6: 887. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12060887