
Easy Scheme Outlining the Various Morphological and Vascular Abnormalities of the Lymph Node Structure Associated with Recent COVID-19 Vaccination, Each with a Different Clinical/Diagnostic Management

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Short-term follow-up with US imaging, starting from the fourth week after the second dose and up to the twelfth week.
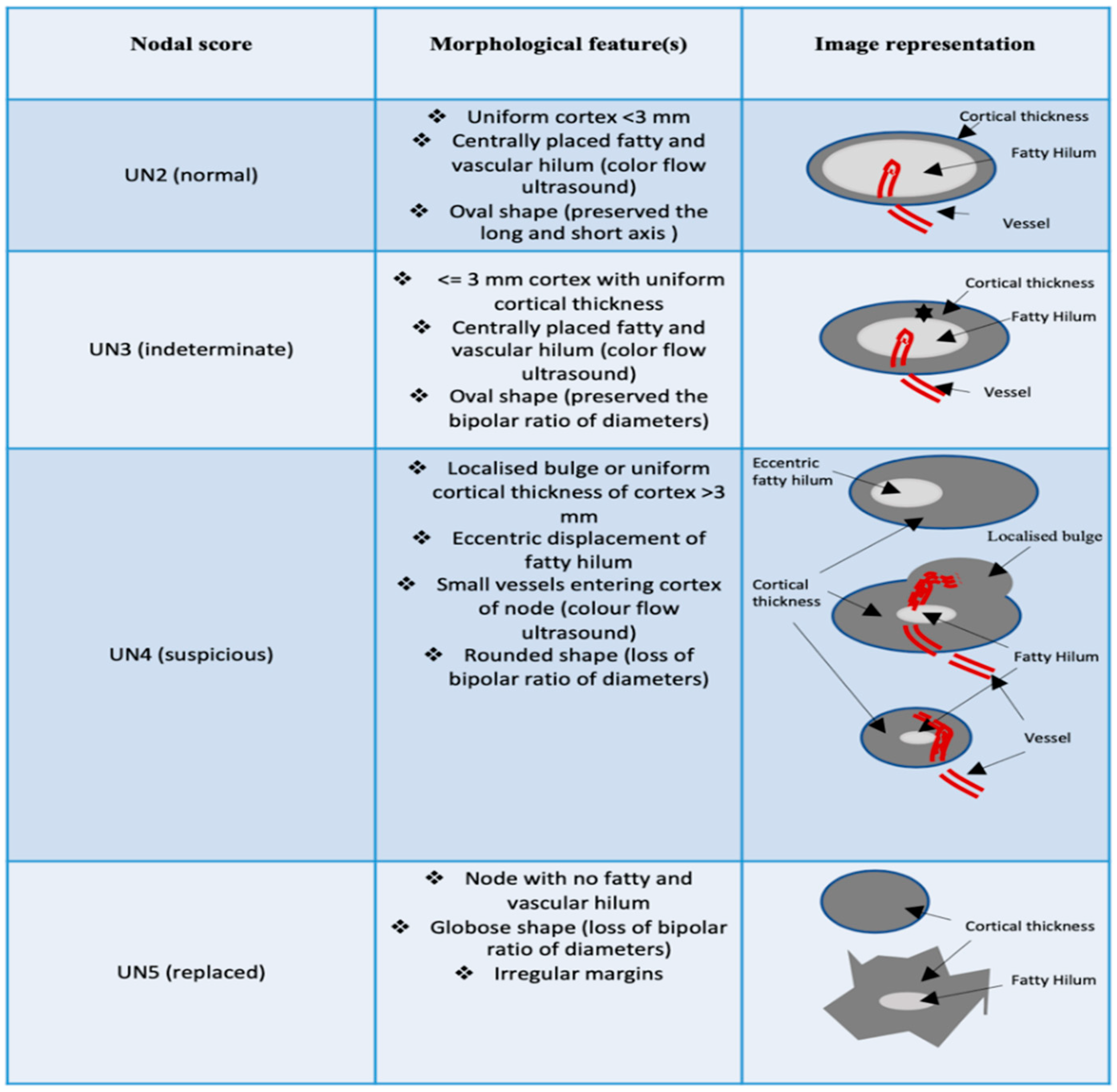
2. Ultrasound Method in Assessing Lymph Node Morphological Features
- ✓
- Morphology (oval vs. round shape/loss of bipolar ratio in diameter).
- ✓
- Thickening of the cortex (>3 mm).
- ✓
- Color Doppler evaluation (centrally placed vascular hilum vs. small vessels entering cortex of node or no/aberrant vascular hilum).
- ✓
- Adipose hilum (centrally vs. eccentric displacement fatty hilum or hilum absence).
- ✓
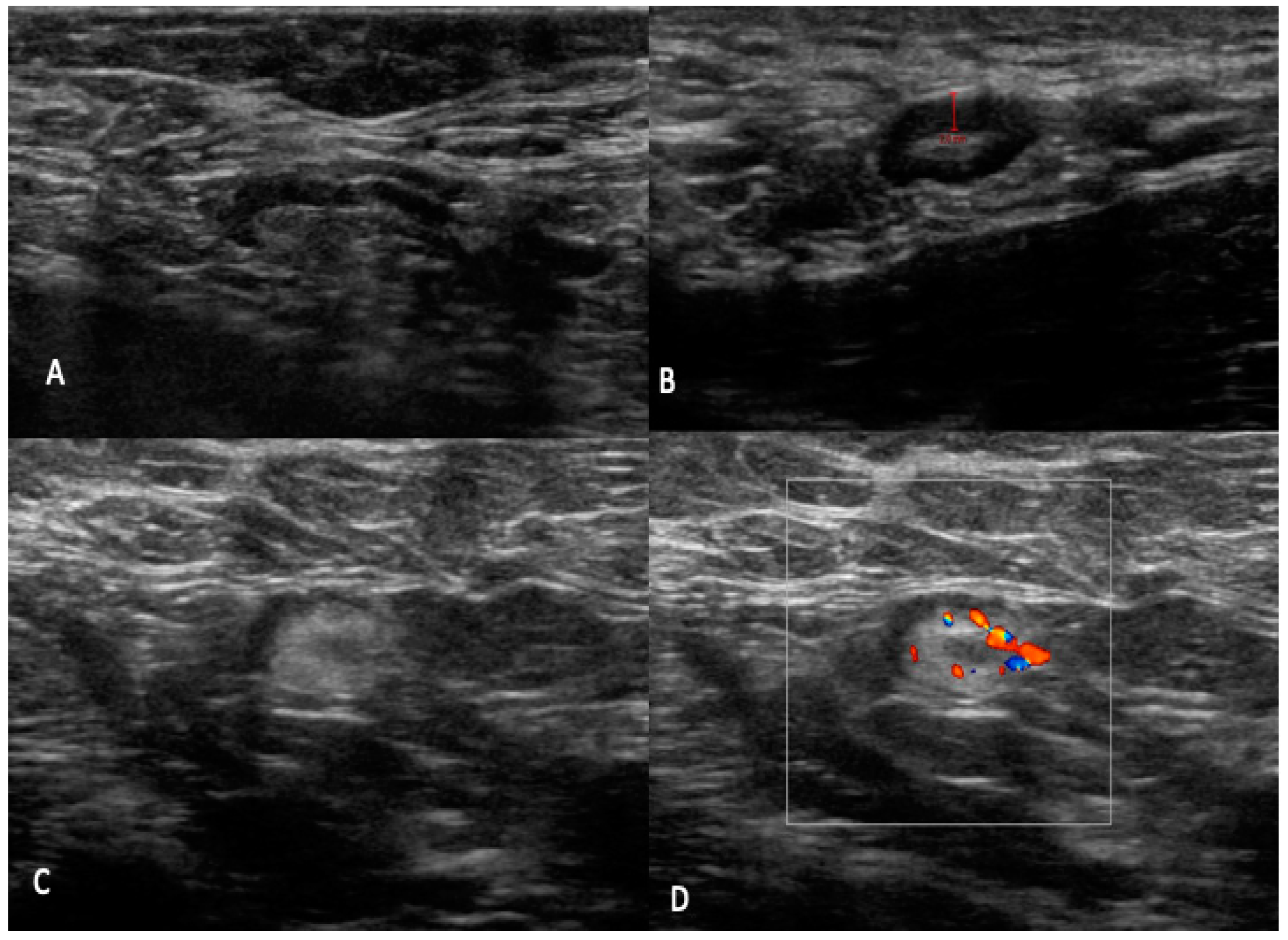
- UN 2: Uniform cortex < 3 mm, centrally placed fatty and vascular hilum (color flow ultrasound), oval shape (preserved the long and short axis) (Figure 2).
- ✓
- UN 3: 3 mm cortex with uniform cortical thickness, centrally placed fatty and vascular hilum (color flow ultrasound), oval shape (preserved the bipolar ratio of diameters) (Figure 3).
- ✓
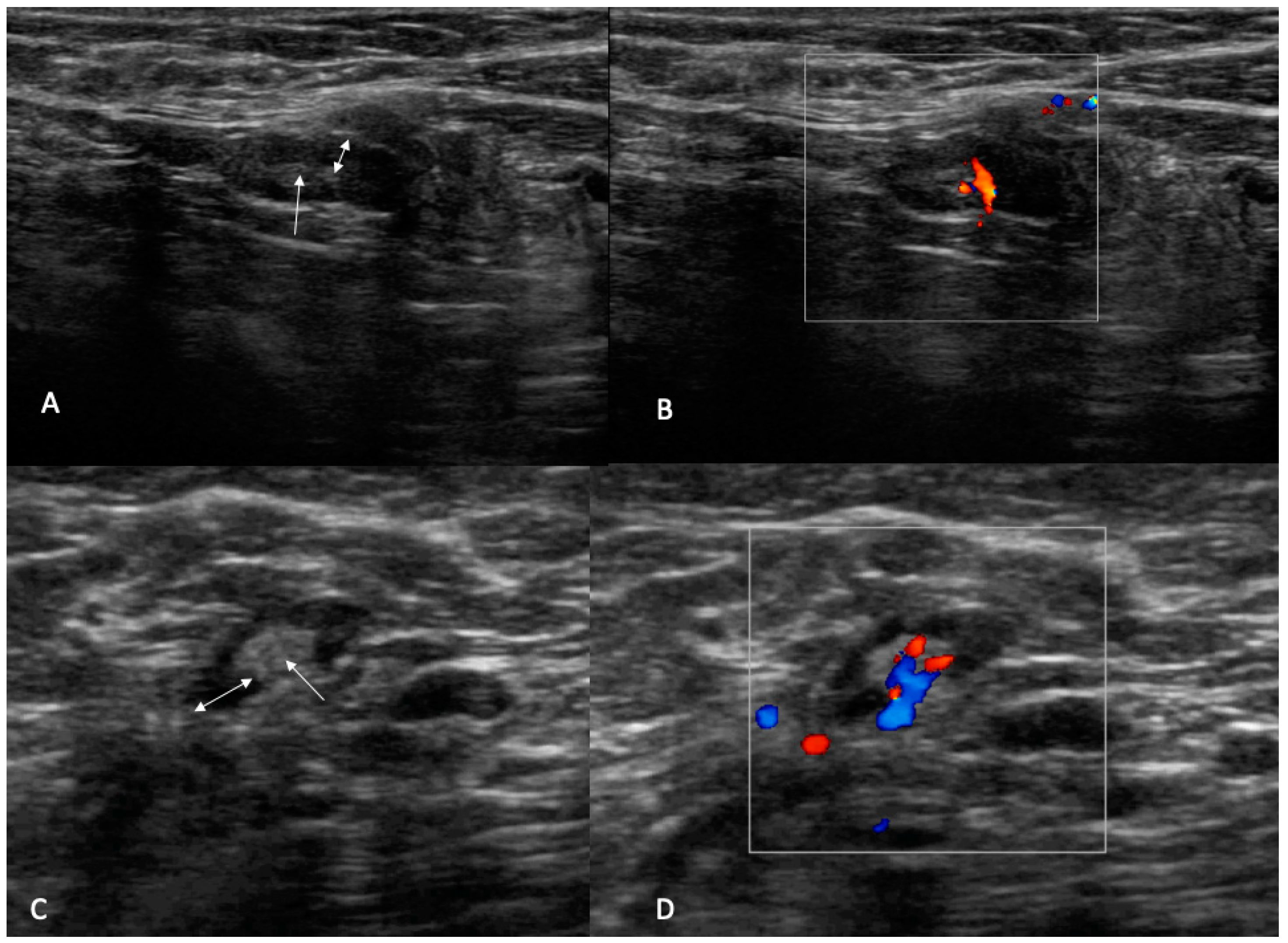
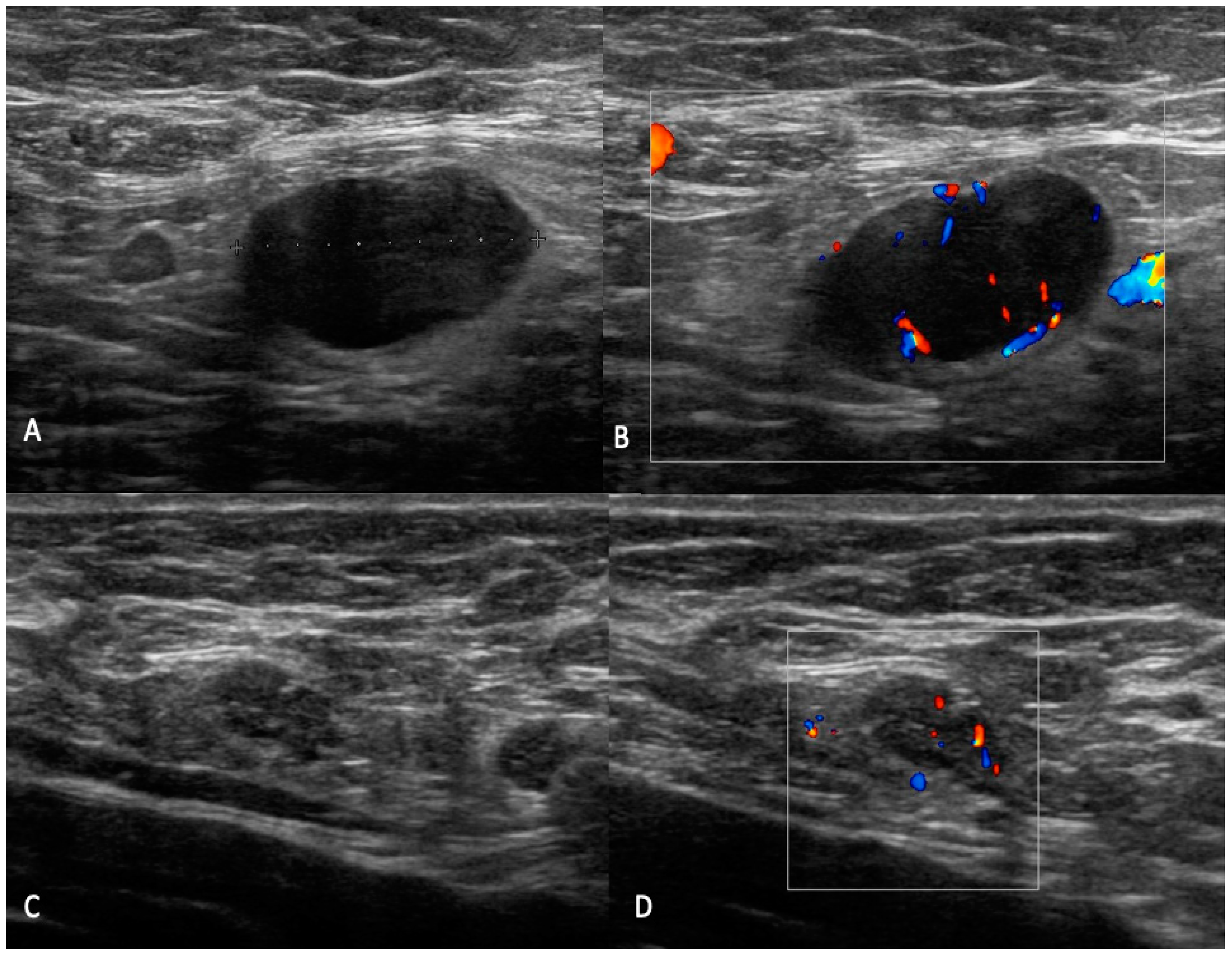
- UN 4: Localized bulge or uniform cortical thickness of cortex > 3 mm, eccentric displacement of fatty hilum, small vessels entering cortex of node (color flow ultrasound), rounded shape (loss of bipolar ratio of diameters) (Figure 4).
- ✓
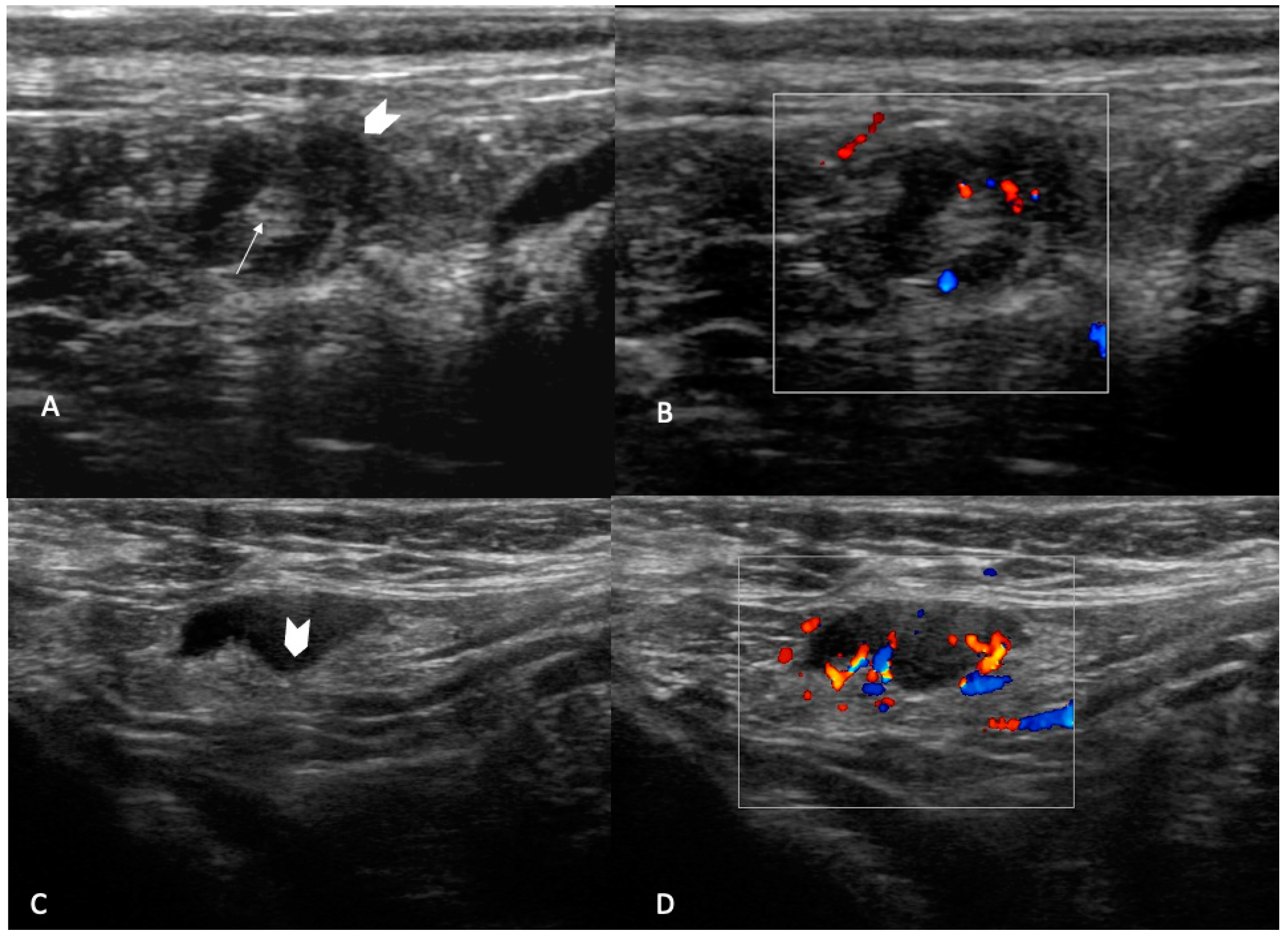
- UN 5: Node with no fatty and vascular hilum or aberrant vascular patterns, globular shape (loss of bipolar ratio of diameters), irregular margins (Figure 5).
3. Differential Diagnosis and Management of Atypical Lymph Nodes
- ✓
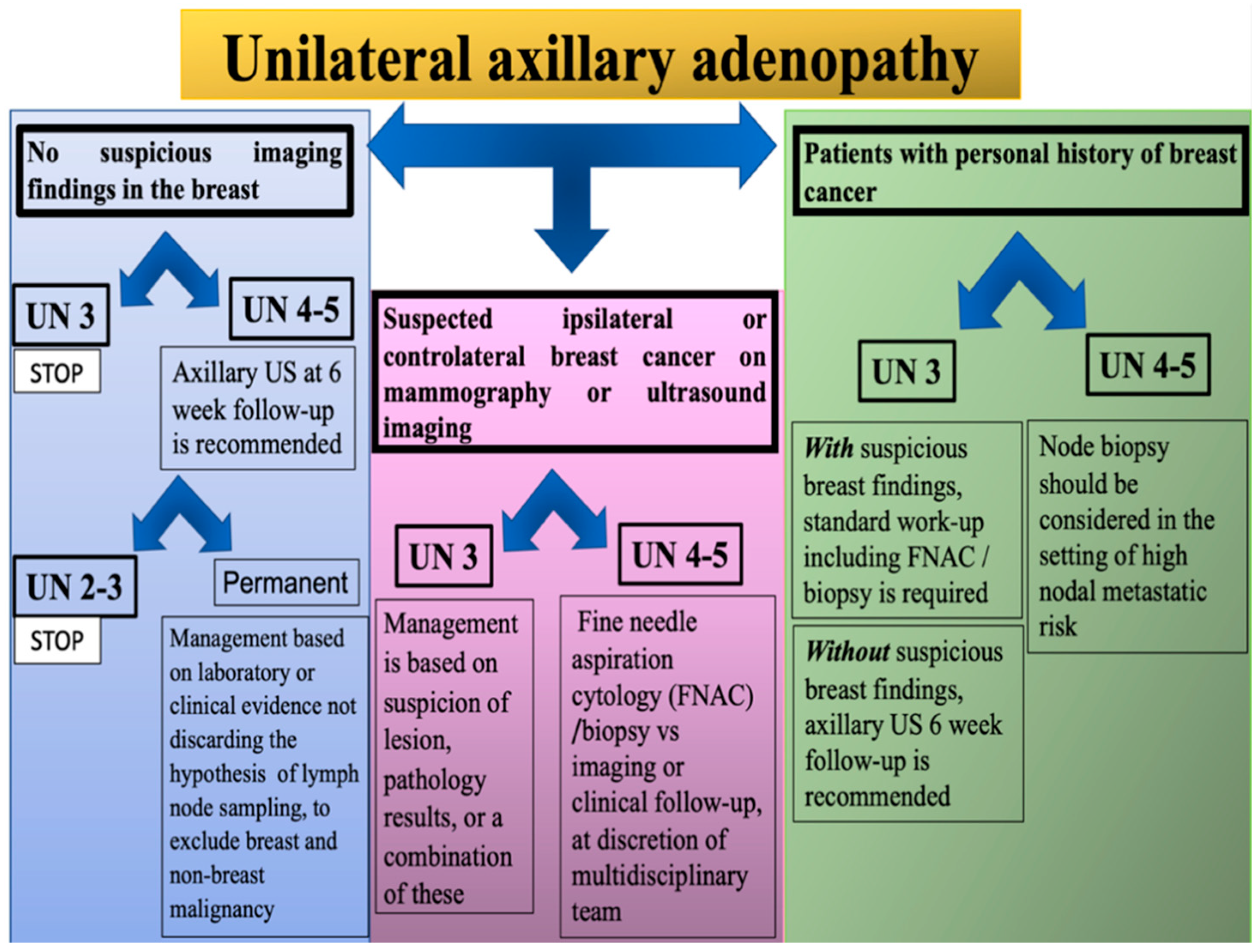
- UN 3 score: Benign. No further imaging is indicated at this time.
- ✓
- UN 4 or 5 score: US 6-week follow-up is recommended. If the lymph node has a lower score at the control, no further imaging is indicated at this time. If the score UN 4/5 remains, management is at the discretion of the attending procedural radiologist and/or surgeon based on laboratory or clinical evidence.
- ✓
- UN 3 score: The management is at the discretion of the attending procedural radiologist based on suspicion of lesion, pathology results, or a combination of these.
- ✓
- UN 4/5 score: Collegial management must be taken (surgeon and/or medical or radiation oncologist in consultation with radiologist), evaluating the choice between fine needle aspiration cytology (FNAC)/biopsy vs. imaging or clinical follow-up.
- ✓
- UN 3 score:
- Unsuspicious breast finding requires short-interval follow-up imaging with ultrasonography (with at least a 6-week delay).
- Suspicious breast finding requires standard work-up, including FNAC/biopsy.
- ✓
- UN 4/5 score: Node biopsy should be considered in the setting of high nodal metastatic risk and immediate histopathologic confirmation is necessary for timely patient management.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Spiteri, G.; Fielding, J.; Diercke, M.; Campese, C.; Enouf, V.; Gaymard, A.; Bella, A.; Sognamiglio, P.; Moros, M.J.S.; Riutort, A.N.; et al. First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Eurosurveillance 2020, 25, 2000178. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Buzatto, I.P.C.; dos Reis, F.J.C.; de Andrade, J.M.; Rodrigues, T.C.G.F.; Borba, J.M.C.; Netto, A.H.; Polydoro, M.S.; Tiezzi, D.G. Axillary ultrasound and fine-needle aspiration cytology to predict clinically relevant nodal burden in breast cancer patients. World J. Surg. Oncol. 2021, 19, 1–8. [Google Scholar] [CrossRef]
- Mansel, R.E.; Fallowfield, L.; Kissin, M.; Goyal, A.; Newcombe, R.G.; Dixon, J.M.; Yiangou, C.; Horgan, K.; Bundred, N.; Monypenny, I.; et al. Randomized Multicenter Trial of Sentinel Node Biopsy Versus Standard Axillary Treatment in Operable Breast Cancer: The ALMANAC Trial. JNCI J. Natl. Cancer Inst. 2006, 98, 599–609. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology; BI-RADS Committee. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013; Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads (accessed on 25 June 2022).
- Seely, J.M.; Barry, M.H. The Canadian Society of Breast Imaging Recommendations for the Management of Axillary Adenopathy in Patients with Recent COVID-19 Vaccination—Update. Can. Assoc. Radiol. J. 2021, 72, 601–602. [Google Scholar] [CrossRef] [PubMed]
- Garreffa, E.; Hamad, A.; O’Sullivan, C.C.; Hazim, A.Z.; York, J.; Puri, S.; Turnbull, A.; Robertson, J.F.; Goetz, M.P. Regional lymphadenopathy following COVID-19 vaccination: Literature review and considerations for patient management in breast cancer care. Eur. J. Cancer 2021, 159, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.A.; Maimone, S.; Gococo-Benore, D.A.; Li, Z.; Advani, P.P.; Chumsri, S. Incidence of Axillary Adenopathy in Breast Imaging After COVID-19 Vaccination. JAMA Oncol. 2021, 7, 1395. [Google Scholar] [CrossRef]
- Grimm, L.; Destounis, S.; Dogan, B.; Nicholson, B.; Dontchos, B.; Sonnenblick, E.; Milch, H.; Pushkin, J.; Benson, J.; Dodelzon, K.; et al. SBI Recommendations for the Management of Axillary Adenopathy in Patients with Recent COVID-19 Vaccination. Available online: https://www.sbi-online.org/Portals/0/Position%20Statements/2021/SBI-recommendations-for-managing-axillary-adenopathy-post-COVID-vaccination.pdf (accessed on 9 March 2021).
- Schiaffino, S.; Pinker, K.; Magni, V.; Cozzi, A.; Athanasiou, A.; Baltzer, P.A.T.; Herrero, J.C.; Clauser, P.; Fallenberg, E.M.; Forrai, G.; et al. Axillary lymphadenopathy at the time of COVID-19 vaccination: Ten recommendations from the European Society of Breast Imaging (EUSOBI). Insights Imaging 2021, 12, 1–7. [Google Scholar] [CrossRef]
- Duke, H.; Posch, L.; Green, L. Axillary adenopathy following COVID-19 vaccination: A single institution case series. Clin. Imaging 2021, 80, 111–116. [Google Scholar] [CrossRef]
- Cui, X.W.; Hocke, M.; Jenssen, C.; Ignee, A.; Klein, S.; Schreiber-Dietrich, D.; Dietrich, C.F. Conventional ultrasound for lymph node evaluation, update 2013. Z. Gastroenterol. 2014, 52, 212–221. [Google Scholar] [CrossRef]
- Net, J.M.; Mirpuri, T.M.; Plaza, M.J.; Escobar, C.A.; Whittington, E.E.; Collado-Mesa, F.; Yepes, M.M. Resident and Fellow Education Feature: US Evaluation of Axillary Lymph Nodes. RadioGraphics 2014, 34, 1817–1818. [Google Scholar] [CrossRef] [PubMed]
- Cocco, G.; Boccatonda, A.; D’Ardes, D.; Galletti, S.; Schiavone, C. Mantle cell lymphoma: From ultrasound examination to histological diagnosis. J. Ultrasound 2018, 21, 339–342. [Google Scholar] [CrossRef]
- Yi, C.-B.; Ding, Z.-Y.; Deng, J.; Ye, X.-H.; Chen, L.; Zong, M.; Li, C.-Y. Combining the Ultrasound Features of Primary Tumor and Axillary Lymph Nodes Can Reduce False-Negative Rate during the Prediction of High Axillary Node Burden in BI-RADS Category 4 or 5 Breast Cancer Lesions. Ultrasound Med. Biol. 2020, 46, 1941–1948. [Google Scholar] [CrossRef] [PubMed]
- Bialek, E.; Jakubowski, W.; Szczepanik, A.; Maryniak, R.; Prochorec-Sobieszek, M.; Bilski, R.; Szopinski, K. Vascular patterns in superficial lymphomatous lymph nodes: A detailed sonographic analysis. J. Ultrasound 2007, 10, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Amonkar, S.; Oates, E.; McLean, L.; Nicholson, S. Pre-operative staging of the axilla in primary breast cancer. By redefining the abnormal appearing node can we reduce investigations without affecting overall treatment? Breast 2013, 22, 1114–1118. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Setola, S.; Galdiero, R.; Picone, C.; Izzo, F.; D’Aniello, R.; Miele, V.; Grassi, R.; Grassi, R.; et al. Lymphadenopathy after BNT162b2 COVID-19 Vaccine: Preliminary Ultrasound Findings. Biology 2021, 10, 214. [Google Scholar] [CrossRef]
- Locklin, J.N.; Woodard, G.A. Mammographic and sonographic findings in the breast and axillary tail following a COVID-19 vaccine. Clin. Imaging 2021, 80, 202–204. [Google Scholar] [CrossRef]
- Garver, K. Managing the Risk of Delayed Breast Cancer Screening Versus COVID-19 Vaccination Associated Axillary Lymphadenopathy. Acad. Radiol. 2021, 28, 1198–1199. [Google Scholar] [CrossRef]
- Lehman, C.D.; D’Alessandro, H.A.; Mendoza, D.P.; Succi, M.D.; Kambadakone, A.; Lamb, L.R. Unilateral Lymphadenopathy after COVID-19 Vaccination: A Practical Management Plan for Radiologists Across Specialties. J. Am. Coll. Radiol. 2021, 18, 843–852. [Google Scholar] [CrossRef]
- Mehta, N.; Sales, R.M.; Babagbemi, K.; Levy, A.D.; McGrath, A.L.; Drotman, M.; Dodelzon, K. Unilateral axillary Adenopathy in the setting of COVID-19 vaccine. Clin. Imaging 2021, 75, 12–15. [Google Scholar] [CrossRef]
- Özütemiz, C.; Krystosek, L.A.; Church, A.L.; Chauhan, A.; Ellermann, J.M.; Domingo-Musibay, E.; Steinberger, D. Lymphadenopathy in COVID-19 Vaccine Recipients: Diagnostic Dilemma in Oncologic Patients. Radiology 2021, 300, E296–E300. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liu, Y.; Wang, Y.; Zheng, X.; Han, J.; Li, Q.; Hu, Y.; Mao, R.; Zhou, J. Quantitative analysis of shear wave elastic heterogeneity for prediction of lymphovascular invasion in breast cancer. Br. J. Radiol. 2021, 94. [Google Scholar] [CrossRef] [PubMed]
- Cocco, G.; Pizzi, A.D.; Fabiani, S.; Cocco, N.; Boccatonda, A.; Frisone, A.; Scarano, A.; Schiavone, C. Lymphadenopathy after the Anti-COVID-19 Vaccine: Multiparametric Ultrasound Findings. Biology 2021, 10, 652. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiaschetti, V.; Ubaldi, N.; De Fazio, S.; Cossu, E. Easy Scheme Outlining the Various Morphological and Vascular Abnormalities of the Lymph Node Structure Associated with Recent COVID-19 Vaccination, Each with a Different Clinical/Diagnostic Management. J. Pers. Med. 2022, 12, 1371. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12091371
Fiaschetti V, Ubaldi N, De Fazio S, Cossu E. Easy Scheme Outlining the Various Morphological and Vascular Abnormalities of the Lymph Node Structure Associated with Recent COVID-19 Vaccination, Each with a Different Clinical/Diagnostic Management. Journal of Personalized Medicine. 2022; 12(9):1371. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12091371
Chicago/Turabian StyleFiaschetti, Valeria, Nicolò Ubaldi, Smeralda De Fazio, and Elsa Cossu. 2022. "Easy Scheme Outlining the Various Morphological and Vascular Abnormalities of the Lymph Node Structure Associated with Recent COVID-19 Vaccination, Each with a Different Clinical/Diagnostic Management" Journal of Personalized Medicine 12, no. 9: 1371. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12091371