
Role of Oral Microbiota Dysbiosis in the Development and Progression of Oral Lichen Planus
 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. OLP: Epidemiology and Clinical Variants
3. Etiopathogenesis of OLP
4. OLP Diagnosis, Treatment, and Malignant Potential
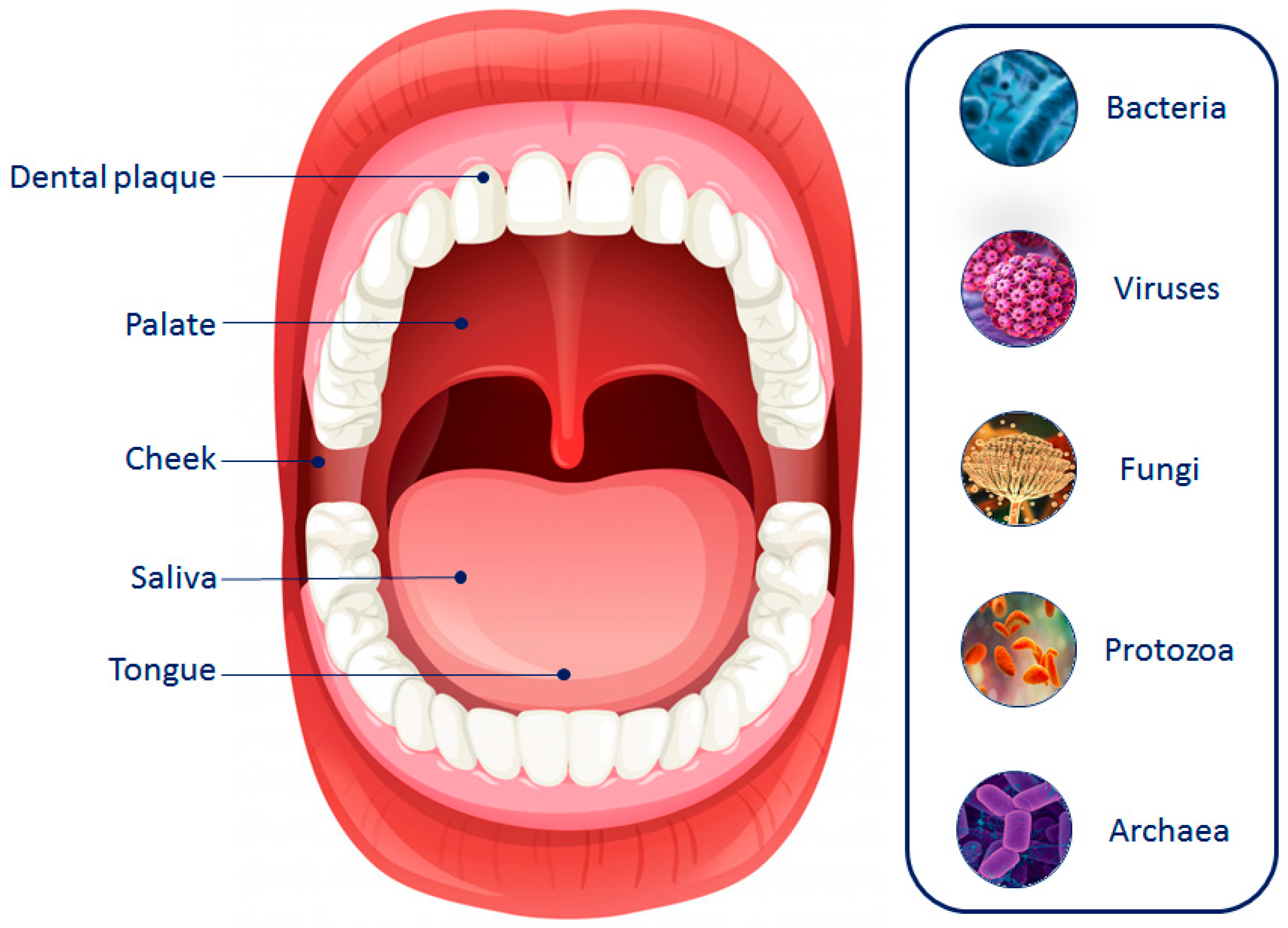
5. Oral Microbiota Composition and Location
6. Oral Microbiota and Oral Diseases
7. The Relationship between Oral Microbiota and OLP Development
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parashar, P. Oral lichen planus. Otolaryngol. Clin. N. Am. 2011, 44, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Piñas, L.; Alkhraisat, M.H. Histopathological features of oral lichen planus and its response to corticosteroid therapy: A retrospective study. Medicine 2019, 98, e18321. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, A.K.; Muthukrishnan, A. A Clinicohistopathological Characterization of Oral Lichen Planus: A Cross-Sectional Study. Cureus 2022, 14, e30568. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Lip, Oral, and Pharyngeal Cancer Collaborators; Cunha, A.R.D.; Compton, K.; Xu, R.; Mishra, R.; Drangsholt, M.T.; Antunes, J.L.F.; Kerr, A.R.; Acheson, A.R.; Lu, D.; et al. The Global, Regional, and National Burden of Adult Lip, Oral, and Pharyngeal Cancer in 204 Countries and Territories: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2023, 9, 1401–1416. [Google Scholar] [PubMed]
- Spirito, F.; Dioguardi, M.; Caponio, V.C.; Ambrosino, M.; Lo Muzio, E.; Lo Muzio, L. Oral lichen planus in children: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2024, 29, e152–e162. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.B.; Kumar, S.K.; Zain, R.B. Oral lichen planus and lichenoid reactions: Etiopathogenesis, diagnosis, management and malignant transformation. J. Oral Sci. 2007, 49, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Setterfield, J.F.; Neill, S.; Shirlaw, P.J.; Theron, J.; Vaughan, R.; Escudier, M.; Challacombe, S.J.; Black, M.M. The vulvovaginal gingival syndrome: A severe subgroup of lichen planus with characteristic clinical features and a novel association with the class II HLA DQB1*0201 allele. J. Am. Acad. Dermatol. 2006, 55, 98–113. [Google Scholar] [CrossRef] [PubMed]
- Quispel, R.; van Boxel, O.S.; Schipper, M.E.; Sigurdsson, V.; Canninga-van Dijk, M.R.; Kerckhoffs, A.; Smout, A.J.; Samsom, M.; Schwartz, M.P. High prevalence of esophageal involvement in lichen planus: A study using magnification chromoendoscopy. Endoscopy 2009, 41, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Gorouhi, F.; Davari, P.; Fazel, N. Cutaneous and mucosal lichen planus: A comprehensive review of clinical subtypes, risk factors, diagnosis, and prognosis. Sci. World J. 2014, 2014, 742826. [Google Scholar] [CrossRef]
- De Porras-Carrique, T.; Ramos-García, P.; Aguilar-Diosdado, M.; Warnakulasuriya, S.; González-Moles, M.Á. Autoimmune disorders in oral lichen planus: A systematic review and meta-analysis. Oral Dis. 2023, 29, 1382–1394. [Google Scholar] [CrossRef]
- Dissemond, J. Oral lichen planus: An overview. J. Dermatol. Treat. 2004, 15, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; Di Bisceglie, M.B.; Scivetti, M.; Lucchese, A.; Tecco, S.; Festa, F. Oral lichen planus: Update on etiopathogenesis, diagnosis and treatment. Immunopharmacol. Immunotoxicol. 2011, 33, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Offen, E.; Allison, J.R. What is the malignant transformation potential of oral lichen planus? Evid. Based Dent. 2022, 23, 36–37. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, L.M.; Cirillo, N.; McCullough, M.J. The immunopathogenesis of oral lichen planus-Is there a role for mucosal associated invariant T cells? J. Oral Pathol. Med. 2019, 48, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Wade, W.G. The oral microbiome in health and disease. Pharmacol. Res. 2013, 69, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Takeshita, T. The oral microbiome and human health. J. Oral Sci. 2017, 59, 201–206. [Google Scholar] [CrossRef]
- Li, X.; Liu, Y.; Yang, X.; Li, C.; Song, Z. The Oral Microbiota: Community Composition, Influencing Factors, Pathogenesis, and Interventions. Front. Microbiol. 2022, 13, 895537. [Google Scholar] [CrossRef]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The human oral microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Leys, E.J.; Bryk, J.M.; Martinez, F.J.; Moeschberger, M.L.; Griffen, A.L. Changes in periodontal health status are associated with bacterial community shifts as assessed by quantitative 16S cloning and sequencing. J. Clin. Microbiol. 2006, 44, 3665–3673. [Google Scholar] [CrossRef]
- Farrell, J.J.; Zhang, L.; Zhou, H.; Chia, D.; Elashoff, D.; Akin, D.; Paster, B.J.; Joshipura, K.; Wong, D.T. Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 2012, 61, 582–588. [Google Scholar] [CrossRef]
- Zarco, M.F.; Vess, T.J.; Ginsburg, G.S. The oral microbiome in health and disease and the potential impact on personalized dental medicine. Oral Dis. 2012, 18, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Casarin, R.C.; Barbagallo, A.; Meulman, T.; Santos, V.R.; Sallum, E.A.; Nociti, F.H.; Duarte, P.M.; Casati, M.Z.; Gonçalves, R.B. Subgingival biodiversity in subjects with uncontrolled type-2 diabetes and chronic periodontitis. J. Periodontal Res. 2013, 48, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Faller, L.L.; Klitgord, N.; Mazumdar, V.; Ghodsi, M.; Sommer, D.D.; Gibbons, T.R.; Treangen, T.J.; Chang, Y.C.; Li, S.; et al. Deep sequencing of the oral microbiome reveals signatures of periodontal disease. PLoS ONE 2012, 7, e37919. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.; Suneja, B.; Walsh, L.J. Ecological Approaches to Dental Caries Prevention: Paradigm Shift or Shibboleth? Caries Res. 2018, 52, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A.; Shay, K. Oral health disparities in older adults: Oral bacteria, inflammation, and aspiration pneumonia. Dent. Clin. North. Am. 2014, 58, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Chhibber-Goel, J.; Singhal, V.; Bhowmik, D.; Vivek, R.; Parakh, N.; Bhargava, B.; Sharma, A. Linkages between oral commensal bacteria and atherosclerotic plaques in coronary artery disease patients. NPJ Biofilms Microbiomes 2016, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Li, S.; Ma, Z.; Liang, S.; Shan, T.; Zhang, M.; Zhu, X.; Zhang, P.; Liu, G.; Zhou, F.; et al. Presence of Porphyromonas gingivalis in esophagus and its association with the clinicopathological characteristics and survival in patients with esophageal cancer. Infect. Agent. Cancer 2016, 11, 3. [Google Scholar] [CrossRef]
- Fan, X.; Alekseyenko, A.V.; Wu, J.; Peters, B.A.; Jacobs, E.J.; Gapstur, S.M.; Purdue, M.P.; Abnet, C.C.; Stolzenberg-Solomon, R.; Miller, G.; et al. Human oral microbiome and prospective risk for pancreatic cancer: A population-based nested case-control study. Gut 2018, 67, 120–127. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Warnakulasuriya, S.; González-Ruiz, I.; González-Ruiz, L.; Ayén, Á.; Lenouvel, D.; Ruiz-Ávila, I.; Ramos-García, P. Worldwide prevalence of oral lichen planus: A systematic review and meta-analysis. Oral Dis. 2021, 27, 813–828. [Google Scholar] [CrossRef]
- Li, C.; Tang, X.; Zheng, X.; Ge, S.; Wen, H.; Lin, X.; Chen, Z.; Lu, L. Global Prevalence and Incidence Estimates of Oral Lichen Planus: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 172–181. [Google Scholar] [CrossRef]
- Cox, T.; Woodhead, J.; Nelson, B.L. Reticular Oral Lichen Planus. Head. Neck Pathol. 2020, 14, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Au, J.; Patel, D.; Campbell, J.H. Oral lichen planus. Oral Maxillofac. Surg. Clin. N. Am. 2013, 25, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Eisen, D.; Carrozzo, M.; Bagan Sebastian, J.V.; Thongprasom, K. Number V Oral lichen planus: Clinical features and management. Oral Dis. 2005, 11, 338–349. [Google Scholar] [CrossRef]
- Scully, C.; Carrozzo, M. Oral mucosal disease: Lichen planus. Br. J. Oral Maxillofac. Surg. 2008, 46, 15–21. [Google Scholar] [CrossRef]
- Canto, A.M.; Müller, H.; Freitas, R.R.; Santos, P.S. Oral lichen planus (OLP): Clinical and complementary diagnosis. An. Bras. Dermatol. 2010, 85, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Carrozzo, M.; Gandolfo, S.; Carbone, M.; Colombatto, P.; Broccoletti, R.; Garzino-Demo, P.; Ghisetti, V. Hepatitis C virus infection in Italian patients with oral lichen planus: A prospective case-control study. J. Oral Pathol. Med. 1996, 25, 527–533. [Google Scholar] [CrossRef]
- Netto, J.N.S.; Pires, F.R.; Costa, K.H.A.; Fischer, R.G. Clinical features of oral lichen planus and oral lichenoid lesions: An oral pathologist’s perspective. Braz. Dent. J. 2022, 33, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Rotaru, D.; Chisnoiu, R.; Picos, A.M.; Picos, A.; Chisnoiu, A. Treatment trends in oral lichen planus and oral lichenoid lesions (Review). Exp. Ther. Med. 2020, 20, 198. [Google Scholar] [CrossRef]
- Tenório, J.R.; de Camargo, A.R.; Lemos, C.; Ortega, K.L. Oral lichen planus and HCV infection. Autops. Case Rep. 2020, 10, e2020210. [Google Scholar] [CrossRef]
- Manomaivat, T.; Pongsiriwet, S.; Kuansuwan, C.; Thosaporn, W.; Tachasuttirut, K.; Iamaroon, A. Association between hepatitis C infection in Thai patients with oral lichen planus: A case-control study. J. Investig. Clin. Dent. 2018, 9, e12316. [Google Scholar] [CrossRef]
- Shang, Q.; Peng, J.; Zhou, Y.; Chen, Q.; Xu, H. Association of Human Papillomavirus with Oral Lichen Planus and Oral Leukoplakia: A Meta-analysis. J. Evid. Based Dent. Pract. 2020, 20, 101485. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Di Stasio, D.; Romano, A.; Fiori, F.; De Felice, G.P.; Lajolo, C.; Serpico, R.; Cecchetti, F.; Petruzzi, M. Correlation between Oral Lichen Planus and Viral Infections Other Than HCV: A Systematic Review. J. Clin. Med. 2022, 11, 5487. [Google Scholar] [CrossRef] [PubMed]
- Shariati, M.; Mokhtari, M.; Masoudifar, A. Association between oral lichen planus and Epstein-Barr virus in Iranian patients. J. Res. Med. Sci. 2018, 23, 24. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, B.; Sengüven, B.; Demir, C. Prevalence of herpes simplex, Epstein Barr and human papilloma viruses in oral lichen planus. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e170–e174. [Google Scholar] [CrossRef]
- Al-Hashimi, I.; Schifter, M.; Lockhart, P.B.; Wray, D.; Brennan, M.; Migliorati, C.A.; Axéll, T.; Bruce, A.J.; Carpenter, W.; Eisenberg, E.; et al. Oral lichen planus and oral lichenoid lesions: Diagnostic and therapeutic considerations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, S25.e1–S25.12. [Google Scholar] [CrossRef]
- Klaisiri, A.; Iamaroon, A.; Neff, A.; Pitak-Arnnop, P. Oral lichenoid lesion related to dental amalgam: A case report. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Carrozzo, M.; Uboldi de Capei, M.; Dametto, E.; Fasano, M.E.; Arduino, P.; Broccoletti, R.; Vezza, D.; Rendine, S.; Curtoni, E.S.; Gandolfo, S. Tumor necrosis factor-alpha and interferon-gamma polymorphisms contribute to susceptibility to oral lichen planus. J. Investig. Dermatol. 2004, 122, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Manczyk, B.; Gołda, J.; Biniak, A.; Reszelewska, K.; Mazur, B.; Zając, K.; Bińczak, P.; Chomyszyn-Gajewska, M.; Oruba, Z. Evaluation of depression, anxiety and stress levels in patients with oral lichen planus. J. Oral Sci. 2019, 61, 391–397. [Google Scholar] [CrossRef]
- Zucoloto, M.L.; Shibakura, M.E.W.; Pavanin, J.V.; Garcia, F.T.; da Silva Santos, P.S.; Maciel, A.P.; de Barros Gallo, C.; Souza, N.V.; Innocentini, L.M.A.R.; Humberto, J.S.M.; et al. Severity of oral lichen planus and oral lichenoid lesions is associated with anxiety. Clin. Oral Investig. 2019, 23, 4441–4448. [Google Scholar] [CrossRef]
- Sugerman, P.B.; Savage, N.W.; Walsh, L.J.; Zhao, Z.Z.; Zhou, X.J.; Khan, A.; Seymour, G.J.; Bigby, M. The pathogenesis of oral lichen planus. Crit. Rev. Oral Biol. Med. 2002, 13, 350–365. [Google Scholar] [CrossRef]
- Lavanya, N.; Jayanthi, P.; Rao, U.K.; Ranganathan, K. Oral lichen planus: An update on pathogenesis and treatment. J. Oral Maxillofac. Pathol. 2011, 15, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Payeras, M.R.; Cherubini, K.; Figueiredo, M.A.; Salum, F.G. Oral lichen planus: Focus on etiopathogenesis. Arch. Oral Biol. 2013, 58, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Guan, X.; Luo, Z.; Liu, Y.; Ren, Q.; Zhao, X. The association and potentially destructive role of Th9/IL-9 is synergistic with Th17 cells by elevating MMP9 production in local lesions of oral lichen planus. J. Oral Pathol. Med. 2018, 47, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Hazzaa, H.H.; El Shiekh, M.A.M.; Abdelgawad, N.; Gouda, O.M.; Kamal, N.M. Correlation of VEGF and MMP-2 levels in oral lichen planus: An in vivo immunohistochemical study. J. Oral Biol. Craniofacial Res. 2020, 10, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.Z.; Sugerman, P.B.; Zhou, X.J.; Walsh, L.J.; Savage, N.W. Mast cell degranulation and the role of T cell RANTES in oral lichen planus. Oral Dis. 2001, 7, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Kramer, I.R.; Lucas, R.B.; Pindborg, J.J.; Sobin, L.H. Definition of leukoplakia and related lesions: An aid to studies on oral precancer. Oral Surg. Oral Med. Oral Pathol. 1978, 46, 518–539. [Google Scholar] [PubMed]
- van der Meij, E.H.; van der Waal, I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications. J. Oral Pathol. Med. 2003, 32, 507–512. [Google Scholar] [CrossRef]
- Idrees, M.; Farah, C.S.; Khurram, S.A.; Firth, N.; Soluk-Tekkesin, M.; Kujan, O. Observer agreement in the diagnosis of oral lichen planus using the proposed criteria of the American Academy of Oral and Maxillofacial Pathology. J. Oral Pathol. Med. 2021, 50, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Gattuso, G.; Crimi, S.; Lavoro, A.; Rizzo, R.; Musumarra, G.; Gallo, S.; Facciponte, F.; Paratore, S.; Russo, A.; Bordonaro, R.; et al. Liquid Biopsy and Circulating Biomarkers for the Diagnosis of Precancerous and Cancerous Oral Lesions. Noncoding RNA 2022, 8, 60. [Google Scholar] [CrossRef]
- Crimi, S.; Falzone, L.; Gattuso, G.; Grillo, C.M.; Candido, S.; Bianchi, A.; Libra, M. Droplet Digital PCR Analysis of Liquid Biopsy Samples Unveils the Diagnostic Role of hsa-miR-133a-3p and hsa-miR-375-3p in Oral Cancer. Biology 2020, 9, 379. [Google Scholar] [CrossRef]
- Kim, T.J.; Kim, Y.G.; Jung, W.; Jang, S.; Ko, H.G.; Park, C.H.; Byun, J.S.; Kim, D.Y. Non-Coding RNAs as Potential Targets for Diagnosis and Treatment of Oral Lichen Planus: A Narrative Review. Biomolecules 2023, 13, 1646. [Google Scholar] [CrossRef] [PubMed]
- Córdova, P.; Rubio, A.; Echeverría, P. Oral lichen planus: A look from diagnosis to treatment. J. Oral Res. 2014, 3, 62–67. [Google Scholar] [CrossRef]
- Gissi, D.B.; Tarsitano, A.; Gabusi, A.; Rossi, R.; Attardo, G.; Lenzi, J.; Marchetti, C.; Montebugnoli, L.; Foschini, M.P.; Morandi, L. 13-gene DNA Methylation Analysis from Oral Brushing: A Promising Non Invasive Tool in the Follow-up of Oral Cancer Patients. J. Clin. Med. 2019, 8, 2107. [Google Scholar] [CrossRef] [PubMed]
- Byun, J.S.; Hong, S.H.; Choi, J.K.; Jung, J.K.; Lee, H.J. Diagnostic profiling of salivary exosomal microRNAs in oral lichen planus patients. Oral Dis. 2015, 21, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Zhong, E.F.; Chang, A.; Stucky, A.; Chen, X.; Mundluru, T.; Khalifeh, M.; Sedghizadeh, P.P. Genomic Analysis of Oral Lichen Planus and Related Oral Microbiome Pathogens. Pathogens 2020, 9, 952. [Google Scholar] [CrossRef] [PubMed]
- Bankvall, M.; Carda-Diéguez, M.; Mira, A.; Karlsson, A.; Hasséus, B.; Karlsson, R.; Robledo-Sierra, J. Metataxonomic and metaproteomic profiling of the oral microbiome in oral lichen planus—A pilot study. J. Oral Microbiol. 2022, 15, 2161726. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, K.; Sivaramakrishnan, G. Interventions for oral lichen planus: A systematic review and network meta-analysis of randomized clinical trials. Aust. Dent. J. 2021, 66, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Lajevardi, V.; Ghodsi, S.Z.; Hallaji, Z.; Shafiei, Z.; Aghazadeh, N.; Akbari, Z. Treatment of erosive oral lichen planus with methotrexate. J. Dtsch. Dermatol. Ges. 2016, 14, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Mansourian, A.; Momen-Heravi, F.; Saheb-Jamee, M.; Esfehani, M.; Khalilzadeh, O.; Momen-Beitollahi, J. Comparison of aloe vera mouthwash with triamcinolone acetonide 0.1% on oral lichen planus: A randomized double-blinded clinical trial. Am. J. Med. Sci. 2011, 342, 447–451. [Google Scholar] [CrossRef]
- Salgado, D.S.; Jeremias, F.; Capela, M.V.; Onofre, M.A.; Massucato, E.M.; Orrico, S.R. Plaque control improves the painful symptoms of oral lichen planus gingival lesions. A short-term study. J. Oral Pathol. Med. 2013, 42, 728–732. [Google Scholar] [CrossRef]
- Yang, H.; Wu, Y.; Ma, H.; Jiang, L.; Zeng, X.; Dan, H.; Zhou, Y.; Chen, Q. Possible alternative therapies for oral lichen planus cases refractory to steroid therapies. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Amanat, D.; Ebrahimi, H.; Zahedani, M.Z.; Zeini, N.; Pourshahidi, S.; Ranjbar, Z. Comparing the effects of cryotherapy with nitrous oxide gas versus topical corticosteroids in the treatment of oral lichen planus. Indian. J. Dent. Res. 2014, 25, 711–716. [Google Scholar] [PubMed]
- Kassem, R.; Yarom, N.; Scope, A.; Babaev, M.; Trau, H.; Pavlotzky, F. Treatment of erosive oral lichen planus with local ultraviolet B phototherapy. J. Am. Acad. Dermatol. 2012, 66, 761–766. [Google Scholar] [CrossRef]
- Mirza, S.; Rehman, N.; Alrahlah, A.; Alamri, W.R.; Vohra, F. Efficacy of photodynamic therapy or low-level laser therapy against steroid therapy in the treatment of erosive-atrophic oral lichen planus. Photodiagn. Photodyn. Ther. 2018, 21, 404–408. [Google Scholar] [CrossRef]
- van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef]
- Eisen, D. The clinical features, malignant potential, and systemic associations of oral lichen planus: A study of 723 patients. J. Am. Acad. Dermatol. 2002, 46, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Gandolfo, S.; Richiardi, L.; Carrozzo, M.; Broccoletti, R.; Carbone, M.; Pagano, M.; Vestita, C.; Rosso, S.; Merletti, F. Risk of oral squamous cell carcinoma in 402 patients with oral lichen planus: A follow-up study in an Italian population. Oral Oncol. 2004, 40, 77–83. [Google Scholar] [CrossRef]
- Laniosz, V.; Torgerson, R.R.; Ramos-Rodriguez, A.J.; Ma, J.E.; Mara, K.C.; Weaver, A.L.; Bruce, A.J. Incidence of squamous cell carcinoma in oral lichen planus: A 25-year population-based study. Int. J. Dermatol. 2019, 58, 296–301. [Google Scholar] [CrossRef]
- Falzone, L.; Bordonaro, R.; Libra, M. SnapShot: Cancer Chemotherapy. Cell 2023, 186, 1816–1816.e1. [Google Scholar] [CrossRef]
- Hartner, L. Chemotherapy for Oral Cancer. Dent. Clin. N. Am. 2018, 62, 87–97. [Google Scholar] [CrossRef]
- Lang, K.; Baur, M.; Held, T.; Shafie, R.E.; Moratin, J.; Freudlsperger, C.; Zaoui, K.; Bougatf, N.; Hoffmann, J.; Plinkert, P.K.; et al. Definitive radiotherapy for squamous cell carcinoma of the oral cavity: A single-institution experience. Radiol. Oncol. 2021, 55, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Sagheb, K.; Blatt, S.; Rahimi-Nedjat, R.K.; Lingawi, A.; Schiegnitz, E.; Kumar, V.V.; Walter, C.; Sagheb, K. Oral Squamous Cell Carcinomas Developing from Oral Lichen Planus: A 5-21 year Retrospective Study. J. Maxillofac. Oral Surg. 2022, 21, 1088–1095. [Google Scholar] [CrossRef]
- Bermejo-Fenoll, A.; Sánchez-Siles, M.; López-Jornet, P.; Camacho-Alonso, F.; Salazar-Sánchez, N. A retrospective clinicopathological study of 550 patients with oral lichen planus in south-eastern Spain. J. Oral Pathol. Med. 2010, 39, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, X.; Li, H.; Ni, C.; Du, Z.; Yan, F. Human oral microbiota and its modulation for oral health. Biomed. Pharmacother. 2018, 99, 883–893. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Li, Y.; Cao, Y.; Xue, J.; Zhou, X. The oral microbiome diversity and its relation to human diseases. Folia Microbiol. 2015, 60, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Maia, B.; Caldas, I.M.; Pereira, M.L.; Pérez-Mongiovi, D.; Araujo, R. The Oral Microbiome in Health and Its Implication in Oral and Systemic Diseases. Adv. Appl. Microbiol. 2016, 97, 171–210. [Google Scholar]
- D’Ambrosio, F.; Santella, B.; Di Palo, M.P.; Giordano, F.; Lo Giudice, R. Characterization of the Oral Microbiome in Wearers of Fixed and Removable Implant or Non-Implant-Supported Prostheses in Healthy and Pathological Oral Conditions: A Narrative Review. Microorganisms 2023, 11, 1041. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.W.; Hsieh, C.H.; Lin, M.R.; Huang, Y.C. Clinical features of gingivostomatitis due to primary infection of herpes simplex virus in children. BMC Infect. Dis. 2020, 20, 782. [Google Scholar] [CrossRef]
- Piña, A.R.; Fonseca, F.P.; Pontes, F.S.; Pontes, H.A.; Pires, F.R.; Mosqueda-Taylor, A.; Aguirre-Urizar, J.M.; de Almeida, O.P. Benign epithelial oral lesions—Association with human papillomavirus. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e290–e295. [Google Scholar] [CrossRef]
- Peters, B.A.; Wu, J.; Hayes, R.B.; Ahn, J. The oral fungal mycobiome: Characteristics and relation to periodontitis in a pilot study. BMC Microbiol. 2017, 17, 157. [Google Scholar] [CrossRef]
- Verma, D.; Garg, P.K.; Dubey, A.K. Insights into the human oral microbiome. Arch. Microbiol. 2018, 200, 525–540. [Google Scholar] [CrossRef] [PubMed]
- Kazarina, A.; Kuzmicka, J.; Bortkevica, S.; Zayakin, P.; Kimsis, J.; Igumnova, V.; Sadovska, D.; Freimane, L.; Kivrane, A.; Namina, A.; et al. Oral microbiome variations related to ageing: Possible implications beyond oral health. Arch. Microbiol. 2023, 205, 116. [Google Scholar] [CrossRef] [PubMed]
- Arweiler, N.B.; Netuschil, L. The Oral Microbiota. Adv. Exp. Med. Biol. 2016, 902, 45–60. [Google Scholar] [PubMed]
- Belstrøm, D.; Holmstrup, P.; Bardow, A.; Kokaras, A.; Fiehn, N.E.; Paster, B.J. Temporal Stability of the Salivary Microbiota in Oral Health. PLoS ONE 2016, 11, e0147472. [Google Scholar] [CrossRef]
- Kim, Y.T.; Jeong, J.; Mun, S.; Yun, K.; Han, K.; Jeong, S.N. Comparison of the oral microbial composition between healthy individuals and periodontitis patients in different oral sampling sites using 16S metagenome profiling. J. Periodontal Implant. Sci. 2022, 52, 394–410. [Google Scholar] [CrossRef] [PubMed]
- Valm, A.M. The Structure of Dental Plaque Microbial Communities in the Transition from Health to Dental Caries and Periodontal Disease. J. Mol. Biol. 2019, 431, 2957–2969. [Google Scholar] [CrossRef] [PubMed]
- Riggio, M.P.; Lennon, A.; Rolph, H.J.; Hodge, P.J.; Donaldson, A.; Maxwell, A.J.; Bagg, J. Molecular identification of bacteria on the tongue dorsum of subjects with and without halitosis. Oral Dis. 2008, 14, 251–258. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; Materna, A.C.; Friedman, J.; Campos-Baptista, M.I.; Blackburn, M.C.; Perrotta, A.; Erdman, S.E.; Alm, E.J. Host lifestyle affects human microbiota on daily timescales. Genome Biol. 2014, 15, R89. [Google Scholar] [CrossRef] [PubMed]
- Belstrøm, D.; Holmstrup, P.; Nielsen, C.H.; Kirkby, N.; Twetman, S.; Heitmann, B.L.; Klepac-Ceraj, V.; Paster, B.J.; Fiehn, N.E. Bacterial profiles of saliva in relation to diet, lifestyle factors, and socioeconomic status. J. Oral Microbiol. 2014, 6, 23609. [Google Scholar] [CrossRef]
- Anukam, K.C.; Agbakoba, N.R. A comparative study of the oral microbiome compositions of healthy postmenopausal, premenopausal, and prepubertal Nigerian females, using 16s rrna metagenomics methods. Niger. J. Clin. Pract. 2017, 20, 1250–1258. [Google Scholar] [CrossRef]
- Galvão-Moreira, L.V.; de Andrade, C.M.; de Oliveira, J.F.F.; Bomfim, M.R.Q.; Figueiredo, P.M.S.; Branco-de-Almeida, L.S. Sex Differences in Salivary Parameters of Caries Susceptibility in Healthy Individuals. Oral Health Prev. Dent. 2018, 16, 71–77. [Google Scholar] [PubMed]
- Kato, I.; Vasquez, A.; Moyerbrailean, G.; Land, S.; Djuric, Z.; Sun, J.; Lin, H.S.; Ram, J.L. Nutritional Correlates of Human Oral Microbiome. J. Am. Coll. Nutr. 2017, 36, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Mason, M.R.; Preshaw, P.M.; Nagaraja, H.N.; Dabdoub, S.M.; Rahman, A.; Kumar, P.S. The subgingival microbiome of clinically healthy current and never smokers. ISME J. 2015, 9, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, T.M. Role of Oral Microbiota in Cancer Development. Microorganisms 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Lucchese, A.; Lajolo, C.; Rupe, C.; Di Stasio, D.; Romano, A.; Petruzzi, M.; Serpico, R. The Oral Microbiota Changes in Orthodontic Patients and Effects on Oral Health: An Overview. J. Clin. Med. 2021, 10, 780. [Google Scholar] [CrossRef] [PubMed]
- Tuominen, H.; Rautava, J. Oral Microbiota and Cancer Development. Pathobiology 2021, 88, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Struzycka, I. The oral microbiome in dental caries. Pol. J. Microbiol. 2014, 63, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Hiller, N.L.; Powell, E.; Kim, L.H.; Spirk, T.; Modesto, A.; Kreft, R. Profiling microorganisms in whole saliva of children with and without dental caries. Clin. Exp. Dent. Res. 2019, 5, 438–446. [Google Scholar] [CrossRef]
- Zhang, D.; Takeshita, T.; Furuta, M.; Kageyama, S.; Asakawa, M.; Nambu, K.; Yamashita, Y. Tongue Microbiota Composition and Dental Caries Experience in Primary School Children. mSphere 2021, 6, e01252-20. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Sanz-Martin, I.; Doolittle-Hall, J.; Teles, R.P.; Patel, M.; Belibasakis, G.N.; Hämmerle, C.H.F.; Jung, R.E.; Teles, F.R.F. Exploring the microbiome of healthy and diseased peri-implant sites using Illumina sequencing. J. Clin. Periodontol. 2017, 44, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Apatzidou, D.; Lappin, D.F.; Hamilton, G.; Papadopoulos, C.A.; Konstantinidis, A.; Riggio, M.P. Microbiome of peri-implantitis affected and healthy dental sites in patients with a history of chronic periodontitis. Arch. Oral Biol. 2017, 83, 145–152. [Google Scholar] [CrossRef]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental plaque-induced gingival conditions. J. Periodontol. 2018, 89, S17–S27. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Ouyang, X.Y.; Chu, Y.; Zhang, Q. Subgingival Microbiome of Gingivitis in Chinese Undergraduates. Chin. J. Dent. Res. 2017, 20, 145–152. [Google Scholar]
- Lundmark, A.; Hu, Y.O.O.; Huss, M.; Johannsen, G.; Andersson, A.F.; Yucel-Lindberg, T. Identification of Salivary Microbiota and Its Association with Host Inflammatory Mediators in Periodontitis. Front. Cell Infect. Microbiol. 2019, 9, 216. [Google Scholar] [CrossRef]
- Bewley, A.F.; Farwell, D.G. Oral leukoplakia and oral cavity squamous cell carcinoma. Clin. Dermatol. 2017, 35, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, S.O.; Greenberg, M.S. Recurrent aphthous stomatitis. Dent. Clin. N. Am. 2014, 58, 281–297. [Google Scholar] [CrossRef]
- Amer, A.; Galvin, S.; Healy, C.M.; Moran, G.P. The Microbiome of Potentially Malignant Oral Leukoplakia Exhibits Enrichment for Fusobacterium, Leptotrichia, Campylobacter, and Rothia Species. Front. Microbiol. 2017, 8, 2391. [Google Scholar] [CrossRef]
- Zhu, Z.; He, Z.; Xie, G.; Fan, Y.; Shao, T. Altered oral microbiota composition associated with recurrent aphthous stomatitis in young females. Medicine 2021, 100, e24742. [Google Scholar] [CrossRef]
- Zhao, H.; Chu, M.; Huang, Z.; Yang, X.; Ran, S.; Hu, B.; Zhang, C.; Liang, J. Variations in oral microbiota associated with oral cancer. Sci. Rep. 2017, 7, 11773. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, P.; Malik, S.; Laha, S.; Das, S.; Bunk, S.; Ray, J.G.; Chatterjee, R.; Saha, A. Dysbiosis of Oral Microbiota During Oral Squamous Cell Carcinoma Development. Front. Oncol. 2021, 11, 614448. [Google Scholar] [CrossRef]
- Baek, K.; Choi, Y. The microbiology of oral lichen planus: Is microbial infection the cause of oral lichen planus? Mol. Oral Microbiol. 2018, 33, 22–28. [Google Scholar] [CrossRef]
- Gao, L.; Xu, T.; Huang, G.; Jiang, S.; Gu, Y.; Chen, F. Oral microbiomes: More and more importance in oral cavity and whole body. Protein Cell 2018, 9, 488–500. [Google Scholar] [CrossRef]
- Wang, K.; Lu, W.; Tu, Q.; Ge, Y.; He, J.; Zhou, Y.; Gou, Y.; Van Nostrand, J.D.; Qin, Y.; Li, J.; et al. Preliminary analysis of salivary microbiome and their potential roles in oral lichen planus. Sci. Rep. 2016, 6, 22943. [Google Scholar] [CrossRef]
- Choi, Y.S.; Kim, Y.; Yoon, H.J.; Baek, K.J.; Alam, J.; Park, H.K.; Choi, Y. The presence of bacteria within tissue provides insights into the pathogenesis of oral lichen planus. Sci. Rep. 2016, 6, 29186. [Google Scholar] [CrossRef]
- He, Y.; Gong, D.; Shi, C.; Shao, F.; Shi, J.; Fei, J. Dysbiosis of oral buccal mucosa microbiota in patients with oral lichen planus. Oral Dis. 2017, 23, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.F.M.S.; Cavalieri, D.; Do Nascimento, S.; Lourenço, T.G.B.; Ramos, D.V.R.; Pasqualin, D.D.C.; Martins, L.A.L.; Rocha, F.A.; Heller, D.; Marti, L. Cytokines Levels and Salivary Microbiome Play A Potential Role in Oral Lichen Planus Diagnosis. Sci. Rep. 2019, 9, 18137. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.Y.; Wang, Q.Q.; Li, M.; Cheng, Y.H.; Cheng, Y.L.; Zhou, Y.; Yang, X.; Zhang, F.; Ge, X.; Zhao, B.; et al. Dysbiosis of saliva microbiome in patients with oral lichen planus. BMC Microbiol. 2020, 20, 75. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, Z.; Tang, N.; Zhao, Y.; Xu, J.; Li, L.; Qian, L.; Zhang, J.; Fan, Y. Microbial Community Analysis of Saliva and Biopsies in Patients with Oral Lichen Planus. Front. Microbiol. 2020, 11, 629. [Google Scholar] [CrossRef]
- Min, Z.; Yang, L.; Hu, Y.; Huang, R. Oral microbiota dysbiosis accelerates the development and onset of mucositis and oral ulcers. Front. Microbiol. 2023, 14, 1061032. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Corrêa, J.D.; Silva, T.A. The Oral Microbiota Is Modified by Systemic Diseases. J. Dent. Res. 2019, 98, 148–156. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pattern | Localization | Clinical Manifestations | Ref. |
|---|---|---|---|
| Reticular | buccal mucosa; tongue; gingiva; palate; lips | Wickham striae surrounded by an erythematous area | [32] |
| Erosive | gingiva; tongue | Keratotic white striae and ulcerations covered by a fibrin plaque | [33] |
| Atrophic | gingiva; tongue dorsum | Red lesions and mucosal atrophy | [34] |
| Plaque-like | tongue; buccal mucosa | Whitish and raised lesions | [35] |
| Bullous | soft palate; lips | Ulcerated areas due to the rupture of bullae | [36] |
| Papular | soft palate; lips | White papules in combination with other patterns | [36] |
| Sample | Microbial Profile Variations | Ref. |
|---|---|---|
| Saliva | ↑: Solobacterium, Porphyromonas ↓: Campylobacter, Corynebacterium, Cellulosimicrobium, Haemophilus | [52] |
| Buccal mucosa | ↑: Leptotrichia, Acinetobacter ↓: Streptococcus, Escherichia | [123] |
| Buccal mucosa | ↑: Leptotrichia, Fusobacterium, Lautropia ↓: Streptococcus | [124] |
| Saliva | ↑: Firmicutes, Actinobacteria ↓: Proteobacteria | [125] |
| Saliva | ↑: Oribacterium, Abiotrophia, Neisseria, Haemophilus, Gemella, Lautropia ↓: Aggregatibacter | [126] |
| Saliva and tissue | ↑: Carnobacteriaceae, Flavobacteriaceae, Delftia, Caulobacteraceae, Sphingomonas, Veillonellaceae | [127] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavoro, A.; Cultrera, G.; Gattuso, G.; Lombardo, C.; Falzone, L.; Saverio, C.; Libra, M.; Salmeri, M. Role of Oral Microbiota Dysbiosis in the Development and Progression of Oral Lichen Planus. J. Pers. Med. 2024, 14, 386. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14040386
Lavoro A, Cultrera G, Gattuso G, Lombardo C, Falzone L, Saverio C, Libra M, Salmeri M. Role of Oral Microbiota Dysbiosis in the Development and Progression of Oral Lichen Planus. Journal of Personalized Medicine. 2024; 14(4):386. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14040386
Chicago/Turabian StyleLavoro, Alessandro, Giovanni Cultrera, Giuseppe Gattuso, Cinzia Lombardo, Luca Falzone, Candido Saverio, Massimo Libra, and Mario Salmeri. 2024. "Role of Oral Microbiota Dysbiosis in the Development and Progression of Oral Lichen Planus" Journal of Personalized Medicine 14, no. 4: 386. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14040386