
Evaluation of a 3D Printed Silicone Oral Cavity Cancer Model for Surgical Simulations

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Construction of a Silicone Tongue Model
2.2. Construction of an Organic Tongue Model
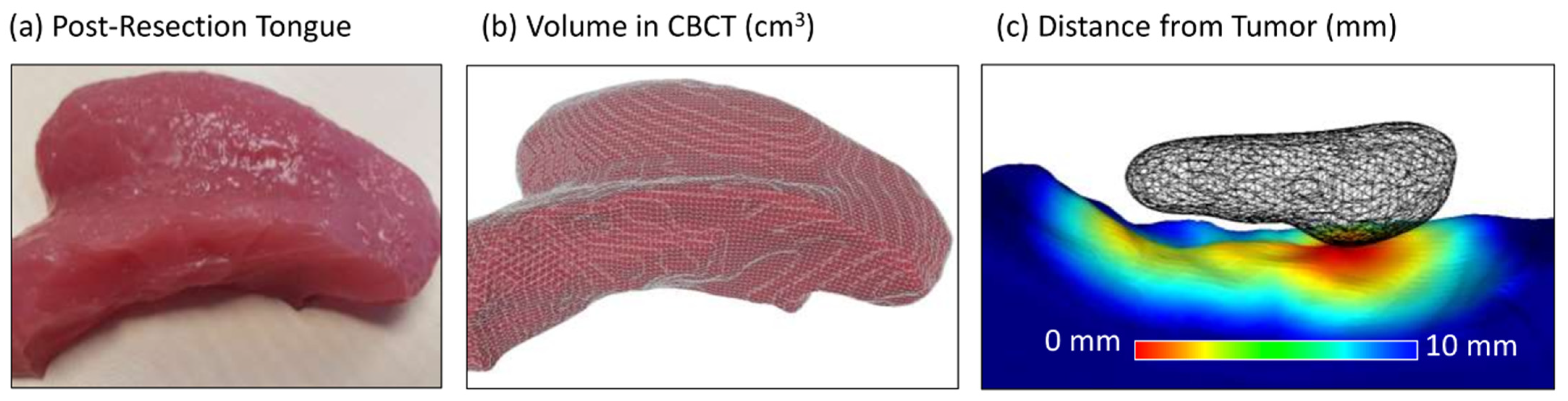
2.3. Evaluation of Training Model
2.4. Statistical Analysis
3. Results
Validity of Models for Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Wang, C.P.; Ko, J.Y.; Yang, T.L.; Lou, P.J. The impact of pathologic close margin on the survival of patients with early stage oral squamous cell carcinoma. Oral Oncol. 2012, 48, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Loree, T.R.; Strong, E.W. Significance of positive margins in oral cavity squamous carcinoma. Am. J. Surg. 1990, 160, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.; Hinther, A.; Matthews, T.W.; Nakoneshny, S.C.; Hart, R.; Dort, J.C.; Chandarana, S.P. The impact of close surgical margins on recurrence in oral squamous cell carcinoma. J. Otolaryngol. Head Neck Surg. 2021, 50, 9. [Google Scholar] [CrossRef] [PubMed]
- Luryi, A.L.; Chen, M.M.; Mehra, S.; Roman, S.A.; Sosa, J.A.; Judson, B.L. Positive surgical margins in early stage oral cavity cancer: An analysis of 20,602 cases. Otolaryngol. Head Neck Surg. 2014, 151, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Smits, R.W.; Koljenovic, S.; Hardillo, J.A.; Ten Hove, I.; Meeuwis, C.A.; Sewnaik, A.; Dronkers, E.A.; Bakker Schut, T.C.; Langeveld, T.P.; Molenaar, J.; et al. Resection margins in oral cancer surgery: Room for improvement. Head Neck 2016, 38 (Suppl. 1), E2197–E2203. [Google Scholar] [CrossRef]
- Camelo-Nunes, J.M.; Hiratsuka, J.; Yoshida, M.M.; Beltrani-Filho, C.A.; Oliveira, L.S.; Nagae, A.C. Ox tongue: An alternative model for surgical training. Plast. Reconstr. Surg. 2005, 116, 352–354. [Google Scholar] [CrossRef]
- Dawe, S.R.; Pena, G.N.; Windsor, J.A.; Broeders, J.A.; Cregan, P.C.; Hewett, P.J.; Maddern, G.J. Systematic review of skills transfer after surgical simulation-based training. Br. J. Surg. 2014, 101, 1063–1076. [Google Scholar] [CrossRef]
- Higgins, M.; Madan, C.; Patel, R. Development and decay of procedural skills in surgery: A systematic review of the effectiveness of simulation-based medical education interventions. Surgeon 2021, 19, e67–e77. [Google Scholar] [CrossRef]
- Chen, S.W.; Zhang, Q.; Guo, Z.M.; Chen, W.K.; Liu, W.W.; Chen, Y.F.; Li, Q.L.; Liu, X.K.; Li, H.; Ou-Yang, D.; et al. Trends in clinical features and survival of oral cavity cancer: Fifty years of experience with 3362 consecutive cases from a single institution. Cancer Manag. Res. 2018, 10, 4523–4535. [Google Scholar] [CrossRef]
- Justesen, M.M.; Stampe, H.; Jakobsen, K.K.; Andersen, A.O.; Jensen, J.M.; Nielsen, K.J.; Gothelf, A.B.; Wessel, I.; Christensen, A.; Gronhoj, C.; et al. Impact of tumor subsite on survival outcomes in oral squamous cell carcinoma: A retrospective cohort study from 2000 to 2019. Oral Oncol. 2024, 149, 106684. [Google Scholar] [CrossRef] [PubMed]
- Sternheim, A.; Kashigar, A.; Daly, M.; Chan, H.; Qiu, J.; Weersink, R.; Jaffray, D.; Irish, J.C.; Ferguson, P.C.; Wunder, J.S. Cone-Beam Computed Tomography-Guided Navigation in Complex Osteotomies Improves Accuracy at All Competence Levels: A Study Assessing Accuracy and Reproducibility of Joint-Sparing Bone Cuts. J. Bone Jt. Surg. Am. 2018, 100, e67. [Google Scholar] [CrossRef] [PubMed]
- Cignoni, P.; Callieri, M.; Corsini, M.; Dellepiane, M.; Ganovelli, F.; Ranzuglia, G. MeshLab: An Open-Source Mesh Processing Tool. In Proceedings of the Sixth Eurographics Italian Chapter Conference, Salerno, Italy, 2–4 July 2008; Vsardcau, E., Ed.; Eurographics Association for Computer Graphics: Eindhoven, The Netherlands, 2008; pp. 129–136. [Google Scholar]
- Bilimoria, K.Y.; Phillips, J.D.; Rock, C.E.; Hayman, A.; Prystowsky, J.B.; Bentrem, D.J. Effect of surgeon training, specialization, and experience on outcomes for cancer surgery: A systematic review of the literature. Ann. Surg. Oncol. 2009, 16, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Bolster, L.; Rourke, L. The Effect of Restricting Residents’ Duty Hours on Patient Safety, Resident Well-Being, and Resident Education: An Updated Systematic Review. J. Grad. Med. Educ. 2015, 7, 349–363. [Google Scholar] [CrossRef]
- Awan, M.; Zagales, I.; McKenney, M.; Kinslow, K.; Elkbuli, A. ACGME 2011 Duty Hours Restrictions and Their Effects on Surgical Residency Training and Patients Outcomes: A Systematic Review. J. Surg. Educ. 2021, 78, e35–e46. [Google Scholar] [CrossRef]
- Coverdill, J.E.; Alseidi, A.; Borgstrom, D.C.; Dent, D.L.; Dumire, R.; Fryer, J.; Hartranft, T.H.; Holsten, S.B.; Nelson, M.T.; Shabahang, M.M.; et al. Assessing the 16 hour intern shift limit: Results of a multi-center, mixed-methods study of residents and faculty in general surgery. Am. J. Surg. 2018, 215, 326–330. [Google Scholar] [CrossRef]
- Patel, V.; Galloway, T.J.; Liu, J.C. The impact of positive margin on survival in oral cavity squamous cell carcinoma. Oral Oncol. 2021, 122, 105499. [Google Scholar] [CrossRef] [PubMed]
- Kalidindi, S.; Kirk, M.; Griffith, E. In-Situ Simulation Enhances Emergency Preparedness in Pediatric Care Practices. Cureus 2018, 10, e3389. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.R.; Soerensen, J.L.; Grantcharov, T.P.; Dalsgaard, T.; Schouenborg, L.; Ottosen, C.; Schroeder, T.V.; Ottesen, B.S. Effect of virtual reality training on laparoscopic surgery: Randomised controlled trial. BMJ 2009, 338, b1802. [Google Scholar] [CrossRef]
- Monachino, A.; Caraher, C.; Ginsberg, J.; Bailey, C.; White, E. Medical Emergencies in the Primary Care Setting: An Evidence Based Practice Approach Using Simulation to Improve Readiness. J. Pediatr. Nurs. 2019, 49, 72–78. [Google Scholar] [CrossRef]
- Compton, E.C.; Agrawal, S.K.; Ladak, H.M.; Chan, S.; Hoy, M.; Nakoneshny, S.C.; Siegel, L.; Dort, J.C.; Lui, J.T. Assessment of a virtual reality temporal bone surgical simulator: A national face and content validity study. J. Otolaryngol. Head Neck Surg. 2020, 49, 17. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.P.; Li, C.Z.; Chen, G.Q.; Song, G.D.; Zhang, Y.Z. Three-Dimensional Printed Skull Base Simulation for Transnasal Endoscopic Surgical Training. World Neurosurg. 2018, 111, e773–e782. [Google Scholar] [CrossRef]
- Ainsworth, T.A.; Kobler, J.B.; Loan, G.J.; Burns, J.A. Simulation model for transcervical laryngeal injection providing real-time feedback. Ann. Otol. Rhinol. Laryngol. 2014, 123, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Broadbent, J.; Murphy, E.C.; Guy, B.; Baguley, K.E.; Young, J. A three-dimensional (3D) printed paediatric trachea for airway management training. Anaesth. Intensive Care 2020, 48, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, K.R.; Cote, V.; Tsui, Y.; Kudernatsch, S.; Peterson, D.R.; Valdez, T.A. Pediatric laryngeal simulator using 3D printed models: A novel technique. Laryngoscope 2017, 127, E132–E137. [Google Scholar] [CrossRef]
- Ock, J.; Gwon, E.; Kim, D.H.; Kim, S.H.; Kim, N. Patient-specific and hyper-realistic phantom for an intubation simulator with a replaceable difficult airway of a toddler using 3D printing. Sci. Rep. 2020, 10, 10631. [Google Scholar] [CrossRef] [PubMed]
- Rulliere, A.; Danion, J.; Fieux, M.; Tonnerre, D.; Faure, J.P.; Legre, M.; Favier, V.; Oriot, D.; Dufour, X.; Carsuzaa, F. SimLife(R): A New Dynamic Model for Head and Neck Surgical Oncology Simulation. Otolaryngol. Head Neck Surg. 2024, 170, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Razavi, C.R.; Tanavde, V.; Shaear, M.; Richmon, J.D.; Russell, J.O. Simulations and simulators in head and neck endocrine surgery. Ann. Thyroid. 2020, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Backhaus, J.; Lutz, R.; Nobis, C.P.; Zeichner, S.; Koenig, S.; Kesting, M.; Olmos, M. A novel approach to microsurgical teaching in head and neck surgery leveraging modern 3D technologies. Sci. Rep. 2023, 13, 20341. [Google Scholar] [CrossRef]
- LaRochelle, E.P.M.; Streeter, S.S.; Littler, E.A.; Ruiz, A.J. 3D-Printed Tumor Phantoms for Assessment of In Vivo Fluorescence Imaging Analysis Methods. Mol. Imaging Biol. 2023, 25, 212–220. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Face Validation | Mean Content Validation | |
|---|---|---|
| Silicone model | 4 | 4.4 |
| Porcine model | 3.6 | 4.1 |
| Closest Margin Recorded | Closest Margin Recorded | ||
|---|---|---|---|
| Resident 1 | 0 | Fellow/attending 1 | 3.2 |
| Resident 2 | 1.8 | Fellow/attending 2 | 1.3 |
| Resident 3 | 3.5 | Fellow/attending 3 | 3.9 |
| Resident 4 | 0.1 | Fellow/attending 4 | 4.5 |
| Fellow/attending 5 | 3.8 | ||
| Fellow/attending 6 | 1.4 | ||
| Median Distance of Closest Margin (mm) | Mean Distance of Closest Margin (mm) | ||
| Residents | 1 | 1.4 | |
| Fellow/attendings | 3.5 | 3 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eu, D.; Daly, M.J.; Taboni, S.; Sahovaler, A.; Gilbank, A.N.; Irish, J.C. Evaluation of a 3D Printed Silicone Oral Cavity Cancer Model for Surgical Simulations. J. Pers. Med. 2024, 14, 450. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050450
Eu D, Daly MJ, Taboni S, Sahovaler A, Gilbank AN, Irish JC. Evaluation of a 3D Printed Silicone Oral Cavity Cancer Model for Surgical Simulations. Journal of Personalized Medicine. 2024; 14(5):450. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050450
Chicago/Turabian StyleEu, Donovan, Michael J. Daly, Stefano Taboni, Axel Sahovaler, Ashley N. Gilbank, and Jonathan C. Irish. 2024. "Evaluation of a 3D Printed Silicone Oral Cavity Cancer Model for Surgical Simulations" Journal of Personalized Medicine 14, no. 5: 450. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050450