
Body Part Pain Affects Subjective and Objective Handball Performance in Japanese Male National Athletes—Results of Short-Term Practical Monitoring of Athletes’ Conditions

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participant Information
2.2. Data Collection
2.2.1. Schedule and Survey Procedure
2.2.2. Athletes’ Basic Information
2.2.3. Quantification of Degree of Body Part Pain and Subjective Handball Performance
2.2.4. Measurement of Heart Rate and Body Movement Vigorousness
2.3. Measurements
2.3.1. Heart Rate Data
2.3.2. Body Acceleration Data
2.4. Statistical Analysis
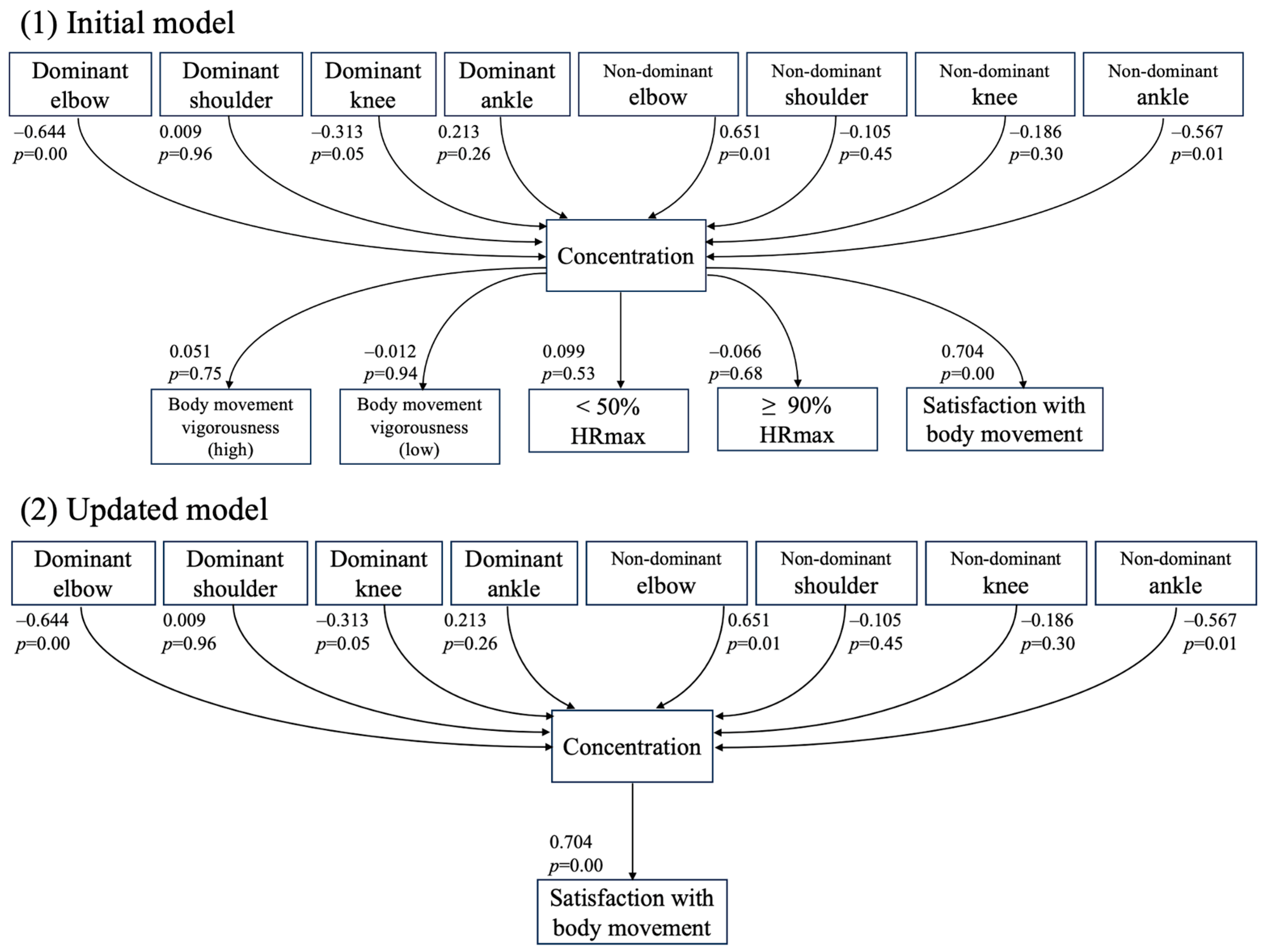
2.4.1. Path Analysis of the Hypothesis Model
2.4.2. Linear Mixed Modeling (LMM)
3. Results
3.1. VAS Scores for Body Part Pain
3.2. Path Analysis Using Subjective and Objective VAS Scores
3.3. Linear Mixed Modeling (LMM)
4. Discussion
4.1. Aim and Hypothesis
4.2. Summary of Pain Results
4.3. Pain in Dominant Elbow Reduced Subjective Performance
4.4. Lower Limb Joint Pain Did Not Affect Subjective Performance
4.5. Body Movement Vigorousness Was Not Affected by Body Pain
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Introduction of International Handball Federation in International Olympic Committee Website. Available online: https://olympics.com/ioc/international-handball-federation (accessed on 29 January 2024).
- Member of Federations, International Handball Federation. Available online: https://www.ihf.info/federations (accessed on 29 January 2024).
- Raya-González, J.; Clemente, F.M.; Beato, M.; Castillo, D. Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3925. [Google Scholar] [CrossRef] [PubMed]
- García-Sánchez, C.; Navarro, R.M.; Karcher, C.; de la Rubia, A. Physical Demands during Official Competitions in Elite Handball: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3353. [Google Scholar] [CrossRef] [PubMed]
- Møller, M.; Nielsen, R.O.; Attermann, J.; Wedderkopp, N.; Lind, M.; Sørensen, H.; Myklebust, G. Handball load and shoulder injury rate: A 31-week cohort study of 679 elite youth handball players. Br. J. Sport Med. 2017, 51, 231. [Google Scholar] [CrossRef] [PubMed]
- Barič, A.; Hlebš, S.; Novak, S.; Brumat, P. Epidemiology of injuries in female and male senior Slovenian handball leagues. J. Sports Med. Phys. Fit. 2021, 61, 1644–1652. [Google Scholar] [CrossRef] [PubMed]
- Asai, K.; Nakase, J.; Shimozaki, K.; Toyooka, K.; Kitaoka, K.; Tsuchiya, H. Incidence of injury in young handball players during national competition: A 6-year survey. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2019, 25, 677–681. [Google Scholar] [CrossRef]
- Seil, R.; Rupp, S.; Tempelhof, S.; Kohn, D. Sports Injuries in Team Handball. Am. J. Sports Med. 1998, 26, 681–687. [Google Scholar] [CrossRef]
- Rafnsson, E.T.; Valdimarsson, Ö.; Sveinsson, T.; Árnason, Á. Injury Pattern in Icelandic Elite Male Handball Players. Clin. J. Sport Med. 2017; ahead of print. [Google Scholar] [CrossRef]
- Mónaco, M.; Rincón, J.A.G.; Ronsano, B.J.M.; Whiteley, R.; Sanz-Lopez, F.; Rodas, G. Injury incidence and injury patterns by category, player position, and maturation in elite male handball elite players. Biol. Sport 2019, 36, 67–74. [Google Scholar] [CrossRef]
- Arora, M.; Shetty, S.H.; Dhillon, M.S. The shoulder in cricket: What’s causing all the painful shoulders? J. Arthrosc. Jt. Surg. 2015, 2, 57–61. [Google Scholar] [CrossRef]
- Kauther, M.D.; Wedemeyer, C.; Wegner, A.; Kauther, K.M.; von Knoch, M. Breakdance Injuries and Overuse Syndromes in Amateurs and Professionals. Am. J. Sports Med. 2009, 37, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Geneviève, J.-P.; Jenny, G. Playing through the Pain: A University-Based Study of Sports Injury. Adv. Phys. Educ. 2016, 6, 178–194. [Google Scholar]
- Malcom, N.L. “Shaking It Off” and “Toughing It Out”. J. Contemp. Ethnogr. 2006, 35, 495–525. [Google Scholar] [CrossRef]
- Chirosa-Ríos, L.J.; Chirosa-Ríos, I.J.; Martínez-Marín, I.; Román-Montoya, Y.; Vera-Vera, J.F. The Role of the Specific Strength Test in Handball Performance: Exploring Differences across Competitive Levels and Age Groups. Sensors 2023, 23, 5178. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.M.; Naughton, J.P.; Haskell, W.L. Physical activity and the prevention of coronary heart disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef] [PubMed]
- Marutani, Y.; Konda, S.; Ogasawara, I.; Yamasaki, K.; Yokoyama, T.; Maeshima, E.; Nakata, K. Gaussian mixture modeling of acceleration-derived signal for monitoring external physical load of tennis player. Front. Physiol. 2023, 14, 1161182. [Google Scholar] [CrossRef]
- Zhang, G.; Yousif, M. The Optimization Model of College Students’ Physical Exercise Motivation and Self-control Ability Based on the Mathematical Model of Probability Theory. Appl. Math. Nonlinear Sci. 2023, 8, 1045–1056. [Google Scholar] [CrossRef]
- Zhang, X.; Feng, S.; Peng, R.; Li, H. Using Structural Equation Modeling to Examine Pathways between Physical Activity and Sleep Quality among Chinese TikTok Users. Int. J. Environ. Res. Public Health 2022, 19, 5142. [Google Scholar] [CrossRef]
- Bere, T.; Alonso, J.-M.; Wangensteen, A.; Bakken, A.; Eirale, C.; Dijkstra, H.P.; Ahmed, H.; Bahr, R.; Popovic, N. Injury and illness surveillance during the 24th Men’s Handball World Championship 2015 in Qatar. Br. J. Sports Med. 2015, 49, 1151. [Google Scholar] [CrossRef]
- Popovic, N.; Lemaire, R. Hyperextension trauma to the elbow: Radiological and ultrasonographic evaluation in handball goalkeepers. Br. J. Sports Med. 2002, 36, 452. [Google Scholar] [CrossRef]
- Tyrdal, S.; Bahr, R. High prevalence of elbow problems among goalkeepers in European team handball—‘Handball goalie’s elbow’. Scand. J. Med. Sci. Sports 1996, 6, 297–302. [Google Scholar] [CrossRef]
- Akgun, U.; Karahan, M.; Tiryaki, C.; Erol, B.; Engebretsen, L. Direction of the load on the elbow of the ball blocking handball goalie. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Fritz, B.; Parkar, A.P.; Cerezal, L.; Storgaard, M.; Boesen, M.; Åström, G.; Fritz, J. Sports Imaging of Team Handball Injuries. Semin. Musculoskelet. Radiol. 2020, 24, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, T.; Hagiwara, Y.; Momma, H.; Tsuchiya, M.; Kuroki, K.; Kanazawa, K.; Yabe, Y.; Yoshida, S.; Koide, M.; Itaya, N.; et al. Coexistence of Trunk or Lower Extremity Pain with Elbow and/or Shoulder Pain among Young Overhead Athletes: A Cross-Sectional Study. Tohoku J. Exp. Med. 2017, 243, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Age (y.o.) | Height (cm) | Weight (kg) | Position | Experience (Years) | Dominant Arm/Leg |
|---|---|---|---|---|---|---|
| 1 | 26 | 190 | 83.9 [0.4] | GK | 13 | R/R |
| 2 | 22 | 190 | 89.8 [0.6] | RW, RB | 14 | L/R |
| 3 | 22 | 182 | 82.6 [0.2] | RW | 15 | L/R |
| 4 | 28 | 178 | 80.1 [0.5] | LW | 18 | R/L |
| 5 | 22 | 186 | 93.6 [0.6] | LB, CB | 8 | R/L |
| 6 | 32 | 183 | 97.4 [0.4] | RB, RW | 20 | L/R |
| 7 | 27 | 190 | 85.6 [0.4] | GK | 12 | R/L |
| 8 | 26 | 183 | 87.3 [0.6] | LB | 18 | R/L |
| 9 | 22 | 190 | 84.2 [0.4] | LB | 11 | R/L |
| 10 | 25 | 190 | 99.8 [0.6] | PV | 12 | R/L |
| 11 | 22 | 186 | 91.6 [0.5] | RB, CB, LB | 9 | R/L |
| 12 | 29 | 182 | 83.4 [0.3] | CB | 22 | R/L |
| 13 | 31 | 182 | 86.1 [0.7] | GK | 20 | R/L |
| 14 | 33 | 190 | 97.7 [0.0] | LB | 20 | R/L |
| Dominant Knee | Dominant Achilles tendon | Dominant Ankle | Dominant Elbow | Dominant Shoulder | |||||||||||||||||||
| No. | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | |||
| 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4.3 | 0 | |||
| 4 | 7.2 | 8 | 2.5 | 4.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 5 | 2.7 | 3.6 | 2.8 | 1.8 | 0 | 0 | 0 | 0 | 6.4 | 3.6 | 3 | 1.8 | 0 | 0 | 0 | 0 | 2.9 | 4 | 0 | 1.5 | |||
| 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5.9 | 6.6 | 6 | 7.1 | 0 | 0 | 0 | 0 | |||
| 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5.7 | 8.5 | 5.8 | 5.9 | 0 | 0 | 0 | 0 | 5 | 6.2 | 4.1 | 4.2 | Pain VAS score | ||
| 9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6.2 | 0 | 0 | 3.1 | 3.7 | 0 | 0 | range in color | ||
| 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5.7 | 6.5 | 6.2 | 0 | 0 | 0 | 0 | [8, 10] | ||
| 11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 3.5 | 4.8 | 2.8 | [6, 8) | ||
| 12 | 8.3 | 9.1 | 10 | 7.8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | [4, 6) | ||
| 13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1.9 | 2.8 | 3.2 | 1.8 | [2, 4) | ||
| 14 | - | 0 | 0 | 0 | - | 0 | 0 | 0 | - | 3 | 0 | 0 | - | 0 | 0 | 0 | - | 0 | 0 | 0 | (0, 2) | ||
| Non-dominant Knee | Non-dominant Achilles tendon | Non-dominant Ankle | Non-dominant Elbow | Non-dominant Shoulder | |||||||||||||||||||
| No. | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | D1 | D2 | D3 | D4 | |||
| 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1.6 | |||
| 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3.9 | 7.2 | 4.7 | 5.3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5.7 | 3.7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 10 | 0 | 0 | 6.4 | 0 | 0 | 0 | 0 | 0 | 6.7 | 5.8 | 0 | 6.6 | 6.3 | 5.7 | 6.5 | 6.2 | 0 | 0 | 0 | 0 | |||
| 11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 12 | 0 | 0 | 0 | 0 | 1.6 | 1.1 | 0 | 4.6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| 14 | - | 0 | 0 | 0 | - | 0 | 0 | 0 | - | 0 | 0 | 0 | - | 0 | 0 | 0 | - | 0 | 2.7 | 2.9 | |||
| Concentration | Satisfaction with Body Movement | |||||||
|---|---|---|---|---|---|---|---|---|
| No. | Day 1 | Day 2 | Day 3 | Day 4 | Day 1 | Day 2 | Day 3 | Day 4 |
| 1 | 3.5 | 7.5 | 3.5 | 3.8 | 2.9 | 7.5 | 3.5 | 3.9 |
| 2 | 7.4 | 3.5 | 3.9 | 3.5 | 7.5 | 2.8 | 3.1 | 2.2 |
| 3 | 6.7 | 7.3 | 5.7 | 6.7 | 7.3 | 7.3 | 6.4 | 6.8 |
| 4 | 7.6 | 7.7 | 7.7 | 6.9 | 7.6 | 7.8 | 7.8 | 6.7 |
| 5 | 7.5 | 6.0 | 7.5 | 7.9 | 5.6 | 5.3 | 4.9 | 5.2 |
| 6 | 4.2 | 6.7 | 4.3 | 2.6 | 5.6 | 6.5 | 5.4 | 4.1 |
| 7 | 3.8 | 3.5 | 2.5 | 2.6 | 4.0 | 3.8 | 2.6 | 2.5 |
| 8 | 5.5 | 6.0 | 6.1 | 5.6 | 5.5 | 5.3 | 5.7 | 4.8 |
| 9 | 6.1 | 2.8 | 5.5 | 4.6 | 6.1 | 3.5 | 3.9 | 5.6 |
| 10 | 6.8 | 6.4 | 6.1 | 5.7 | 6.9 | 6.3 | 6.1 | 5.5 |
| 11 | 7.6 | 7.5 | 10.0 | 8.0 | 5.6 | 5.2 | 10.0 | 7.8 |
| 12 | 3.3 | 7.4 | 2.0 | 5.4 | 5.0 | 5.4 | 2.9 | 2.6 |
| 13 | 4.3 | 6.5 | 7.5 | 7.5 | 2.2 | 5.6 | 6.3 | 6.3 |
| 14 | - | 0.0 | 5.0 | 6.8 | - | 2.9 | 2.0 | 5.3 |
| Body Movement Vigorousness (High) Unit: G | Body Movement Vigorousness (Low) Unit: G | <50% HRmax Unit: % | >90% HRmax Unit: % | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Day 1 | Day 2 | Day 3 | Day 4 | Day 1 | Day 2 | Day 3 | Day 4 | Day 1 | Day 2 | Day 3 | Day 4 | Day 1 | Day 2 | Day 3 | Day 4 |
| 1 | 1.1 | 1.1 | 1.2 | 1.0 | 0.3 | 0.3 | 0.4 | 0.3 | 5.4 | 1.1 | 11.9 | 17.4 | 0.5 | 5.6 | 1.6 | 0.0 |
| 2 | 1.2 | 1.2 | 1.1 | 1.1 | 0.4 | 0.3 | 0.4 | 0.3 | 0.0 | 0.3 | 11.8 | 9.1 | 14.4 | 4.3 | 0.1 | 0.0 |
| 3 | 1.3 | 1.3 | 1.2 | 1.2 | 0.4 | 0.4 | 0.3 | 0.3 | 10.1 | 3.4 | 28.9 | 23.3 | 0.0 | 0.0 | 0.0 | 0.0 |
| 4 | 1.3 | 1.1 | 1.4 | 1.3 | 0.4 | 0.4 | 0.4 | 0.3 | 3.4 | 0.6 | 1.4 | 11.5 | 32.4 | 26.9 | 12.0 | 0.6 |
| 5 | 1.2 | N.A. | 1.1 | 1.0 | 0.3 | N.A. | 0.3 | 0.3 | 6.3 | N.A. | 3.3 | 12.3 | 24.0 | N.A. | 23.3 | 0.0 |
| 6 | 1.3 | 1.1 | 1.2 | 1.2 | 0.3 | 0.3 | 0.3 | 0.3 | 7.4 | 3.0 | 33.3 | 12.8 | 6.6 | 4.5 | 0.1 | 0.0 |
| 7 | N.A. | N.A. | 1.0 | 1.1 | N.A. | N.A. | 0.3 | 0.3 | N.A. | N.A. | 7.5 | 9.7 | N.A. | N.A. | 4.5 | 9.4 |
| 8 | 1.1 | 1.1 | 1.2 | N.A. | 0.3 | 0.3 | 0.3 | N.A. | 5.8 | 1.3 | 10.4 | N.A. | 5.0 | 12.4 | 13.0 | N.A. |
| 9 | 1.1 | 1.2 | 1.3 | 1.1 | 0.3 | 0.3 | 0.3 | 0.3 | 5.9 | 0.9 | 3.8 | 11.3 | 1.1 | 1.6 | 4.2 | 0.0 |
| 10 | 1.3 | 1.1 | 1.1 | 1.2 | 0.3 | 0.3 | 0.3 | 0.3 | 5.3 | 3.0 | 6.8 | 14.3 | 4.2 | 3.0 | 1.1 | 0.0 |
| 11 | 1.2 | 1.1 | 1.2 | 1.2 | 0.3 | 0.3 | 0.3 | 0.3 | 13.6 | 20.8 | 15.4 | 34.4 | 0.5 | 0.7 | 0.0 | 0.0 |
| 12 | 1.2 | 1.1 | 1.3 | 1.1 | 0.3 | 0.3 | 0.3 | 0.3 | 7.2 | 1.3 | 3.6 | 7.1 | 21.1 | 23.3 | 16.7 | 0.9 |
| 13 | 1.4 | 1.2 | 1.3 | 1.3 | 0.4 | 0.3 | 0.3 | 0.3 | 2.4 | 0.0 | 10.8 | 9.1 | 8.7 | 8.3 | 2.3 | 6.5 |
| 14 | - | N.A. | 1.2 | 1.2 | - | N.A. | 0.3 | 0.3 | - | N.A. | 5.1 | 15.9 | - | N.A. | 1.7 | 0.0 |
| Estimate | Standard Error | Degree of Freedom | t-Value | p-Value | |
|---|---|---|---|---|---|
| Intercept | 6.757 | 0.640 | 12.207 | 10.547 | <0.01 * |
| D Shoulder | −0.042 | 0.179 | 28.854 | −0.236 | 0.82 |
| Nd Shoulder | 0.108 | 0.435 | 24.926 | 0.248 | 0.80 |
| D Elbow | −0.358 | 0.142 | 22.842 | −2.520 | 0.02 * |
| Nd Elbow | 0.324 | 0.323 | 10.830 | 1.003 | 0.34 |
| D Knee | −0.156 | 0.134 | 13.824 | −1.166 | 0.26 |
| Nd Knee | −0.076 | 0.323 | 32.983 | −0.236 | 0.81 |
| D Ankle | 0.044 | 0.212 | 12.185 | 0.207 | 0.84 |
| Nd Ankle | −0.169 | 0.209 | 23.113 | −0.810 | 0.43 |
| Nd Achilles Tendon | 0.183 | 0.348 | 31.939 | 0.528 | 0.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogasawara, I.; Shindo, D.; Fujiwara, K.; Suzuki, H.; Ueno, Y.; Kato, H.; Takada, M.; Adachi, Y.; Todoroki, M.; Iwasaki, S.; et al. Body Part Pain Affects Subjective and Objective Handball Performance in Japanese Male National Athletes—Results of Short-Term Practical Monitoring of Athletes’ Conditions. Sports 2024, 12, 65. https://0-doi-org.brum.beds.ac.uk/10.3390/sports12030065
Ogasawara I, Shindo D, Fujiwara K, Suzuki H, Ueno Y, Kato H, Takada M, Adachi Y, Todoroki M, Iwasaki S, et al. Body Part Pain Affects Subjective and Objective Handball Performance in Japanese Male National Athletes—Results of Short-Term Practical Monitoring of Athletes’ Conditions. Sports. 2024; 12(3):65. https://0-doi-org.brum.beds.ac.uk/10.3390/sports12030065
Chicago/Turabian StyleOgasawara, Issei, Daichi Shindo, Kazuki Fujiwara, Haruka Suzuki, Yuki Ueno, Hiroyuki Kato, Michihiro Takada, Yusuke Adachi, Manabu Todoroki, Susumu Iwasaki, and et al. 2024. "Body Part Pain Affects Subjective and Objective Handball Performance in Japanese Male National Athletes—Results of Short-Term Practical Monitoring of Athletes’ Conditions" Sports 12, no. 3: 65. https://0-doi-org.brum.beds.ac.uk/10.3390/sports12030065