The Effects of Postprandial Resistance Exercise on Blood Glucose and Lipids in Prediabetic, Beta-Thalassemia Major Patients

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- BTM patients requiring regular blood transfusions.
- Confirmed prediabetes with patients fulfilling one if the three following criteria: (a) impaired fasting glucose (IFG) (fasting plasma glucose (FPG) of 6.1–6.9 mmol/L), or (b) impaired glucose tolerance (IGT) (plasma glucose of 7.8–11.0 mmol/L, 2 h following ingestion of 75 g of oral glucose load) or (c) a combination of the two, based on a 2 h oral glucose tolerance test [1].
- Age group of 25 to 55.
- Hypertension.
- Injuries.
- Any other serious complications of BTM that could contraindicate participation to exercise.
2.2. Experimental Design
2.3. Anthropometric and Physiological Characteristics
2.4. Blood Collection and Handling
2.5. Blood Analysis
2.6. Statistical Analysis
3. Results
3.1. Anthropometric and Physiological Characteristics
3.2. Metabolic Parameters
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation; World Health Organization: Geneva, Switzerland, 2006; pp. 1–50. [Google Scholar]
- Bansal, N. Prediabetes diagnosis and treatment: A review. World J. Diabetes 2015, 6, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Borror, A.; Zieff, G.; Battaglini, C.; Stoner, L. The Effects of Postprandial Exercise on Glucose Control in Individuals with Type 2 Diabetes: A Systematic Review. Sports Med. 2018, 48, 1479–1491. [Google Scholar] [CrossRef] [PubMed]
- Heden, T.D.; Winn, N.C.; Mari, A.; Booth, F.W.; Rector, R.S.; Thyfault, J.P.; Kanaley, J.A. Postdinner resistance exercise improves postprandial risk factors more effectively than predinner resistance exercise in patients with type 2 diabetes. J. Appl. Physiol. 2015, 118, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taher, A.T.; Saliba, A.N. Iron overload in thalassemia: Different organs at different rates. Hematology. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Cario, H.; Holl, R.W.; Debatin, K.M.; Kohne, E. Insulin sensitivity and beta-cell secretion in thalassaemia major with secondary haemochromatosis: Assessment by oral glucose tolerance test. Eur. J. Pediatr. 2003, 162, 139–146. [Google Scholar] [CrossRef]
- Halliwell, B.; Gutteridge, J.M.C. Role of free radicals and catalytic metal ions in human disease: An overview. Methods Enzymol. 1990, 186, 1–85. [Google Scholar]
- Tiedge, M.; Lortz, S.; Drinkgern, J.; Lenzen, S. Relation between antioxidant enzyme gene expression and antioxidative defense status of insulin-producing cells. Diabetes 1997, 46, 1733–1742. [Google Scholar] [CrossRef]
- Sohn, E.Y.; Kato, R.; Noetzli, L.J.; Gera, A.; Coates, T.; Harmatz, P.; Keens, T.G.; Wood, J.C. Exercise performance in thalassemia major: Correlation with cardiac iron burden. Am. J. Hematol. 2013, 88, 193–197. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. US National Institutes of Health. Available online: http://www.clinicaltrials.gov (accessed on 14 January 2020).
- Georgakouli, K.; Manthou, E.; Fatouros, I.G.; Deli, C.K.; Spandidos, D.A.; Tsatsakis, A.M.; Kouretas, D.; Koutedakis, Y.; Theodorakis, Y.; Jamurtas, A.Z. Effects of acute exercise on liver function and blood redox status in heavy drinkers. Exp. Ther. Med. 2015, 10, 2015–2022. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Laughlin, M.H. Physical activity-induced remodeling of vasculature in skeletal muscle: Role in treatment of type 2 diabetes. J. Appl. Physiol. 2016, 120, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Dijk, J.W.; Manders, R.J.; Tummers, K.; Bonomi, A.G.; Stehouwer, C.D.; Hartgens, F.; van Loon, L.J. Both resistance- and endurance type exercise reduce the prevalence of hyperglycaemia in individuals with impaired glucose tolerance and in insulin-treated and non-insulin-treated type 2 diabetic patients. Diabetologia 2012, 55, 1273–1282. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports Medicine, American Diabetes Association. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Mauvais-Jarvis, F. Gender differences in glucose homeostasis and diabetes. Physiol. Behav. 2018, 187, 20–23. [Google Scholar] [CrossRef]
- van Genugten, R.E.; Utzschneider, K.M.; Tong, J.; Gerchman, F.; Zraika, S.; Udayasankar, J.; Boyko, E.J.; Fujimoto, W.Y.; Kahn, S.E. American Diabetes Association GENNID Study Group. Effects of sex and hormone replacement therapy use on the prevalence of isolated impaired fasting glucose and isolated impaired glucose tolerance in subjects with a family history of type 2 diabetes. Diabetes 2006, 55, 3529–3535. [Google Scholar] [CrossRef] [Green Version]
- Nordestgaard, B.; Benn, M.; Schnohr, P.; Tybjaerg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 2007, 289, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Blum, S.; Aviram, M.; Ben-Amotz, A.; Levy, Y. Effect of a Mediterranean meal on post-prandial carotenoids, paraoxonase activity and C-reactive protein levels. Ann. Nutr. Metab. 2006, 50, 20–24. [Google Scholar] [CrossRef]
- Jakulj, F.; Zernicke, K.; Bacon, S.L.; van Wielingen, L.E.; Key, B.L.; West, S.G.; Campbell, T.S. A high fat meal increases cardiovascular reactivity to psychological stress in healthy young adults. J. Nutr. 2007, 137, 935–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattar, N.; Gaw, A.; Scherbakova, O. Metabolic syndrome with and without creactive protein as a predictor of coronary heart disease and diabetes in the West of Scotland Coronary Prevention Study. Circulation 2003, 108, 414–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | ExT | CoT |
|---|---|---|
| BM (kg) | 66.0 ± 16.6 | 65.5 ± 16.2 |
| BMI (kg/m2) | 24.2 ± 5.4 (men: 25.7 ± 7.2; women: 22.6 ± 3.8) | 24.0 ± 5.2 (men: 25.6 ± 6.8; women: 22.4 ± 3.7) |
| %BF | 37.6 ± 5.1 (men: 25.7; women: 22.6) | 37.6 ± 5.1 (men: 25.7; women: 22.6) |
| WC (cm) | 93.5 ± 12.2 (men: 101.7 ± 9.1; women: 85.3 ± 9.5) | 93.0 ± 11.6 (men: 101.0 ± 7.9; women: 85.0 ± 9.0) |
| HC (cm) | 97.5 ± 8.2 (men: 100.3 ± 8.5; women: 94.7 ± 8.5) | 97.5 ± 8.2 (men: 100.3 ± 8.5; women: 94.7 ± 8.5) |
| WHR | 0.96 ± 0.07 (men: 1.01 ± 0.03; women: 0.90 ± 0.02) | 0.95 ± 0.06 (men: 1.00 ± 0.03; women: 0.90 ± 0.01) |
| RHR | 79.0 ± 8.6 | 77.5 ± 9.2 |
| SBP (mmHg) | 104.5 ± 9.7 | 103.7 ± 10.3 |
| DBP (mmHg) | 67.5 ± 7.6 | 67.5 ± 7.6 |
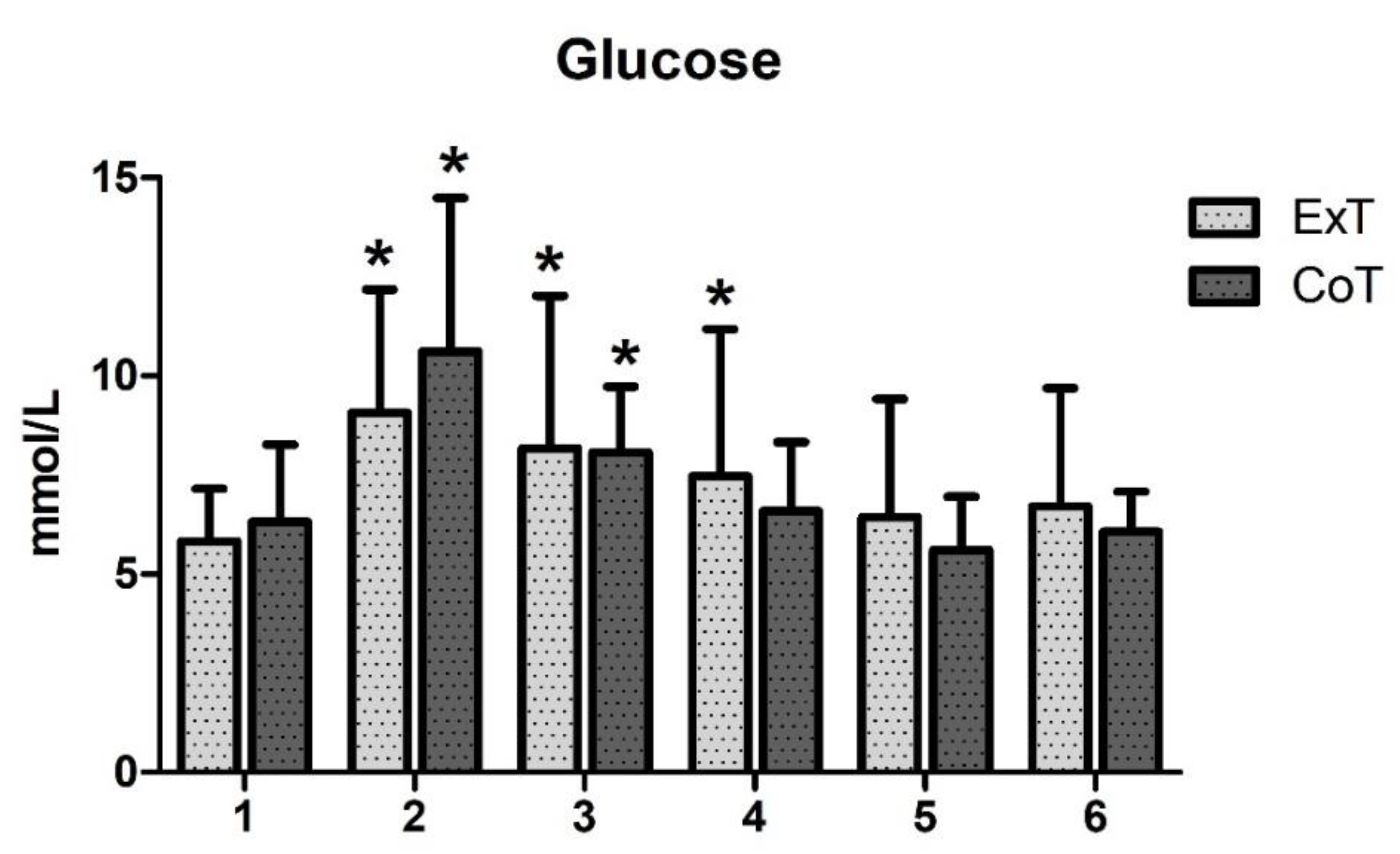
| Time point | ExT | CoT |
|---|---|---|
| 1 | 5.83 ± 1.33 | 6.32 ± 1.95 |
| 2 | 9.07 ± 3.11 * | 10.62 ± 3.87 * |
| 3 | 8.17 ± 3.85 * | 8.07 ± 1.66 * |
| 4 | 7.47 ± 3.71 * | 6.60 ± 1.73 |
| 5 | 6.43 ± 2.99 | 5.61 ± 1.35 |
| 6 | 6.71 ± 2.99 | 6.07 ± 1.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgakouli, K.; Stamperna, A.; Deli, C.K.; Syrou, N.; Draganidis, D.; Fatouros, I.G.; Jamurtas, A.Z. The Effects of Postprandial Resistance Exercise on Blood Glucose and Lipids in Prediabetic, Beta-Thalassemia Major Patients. Sports 2020, 8, 57. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8050057
Georgakouli K, Stamperna A, Deli CK, Syrou N, Draganidis D, Fatouros IG, Jamurtas AZ. The Effects of Postprandial Resistance Exercise on Blood Glucose and Lipids in Prediabetic, Beta-Thalassemia Major Patients. Sports. 2020; 8(5):57. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8050057
Chicago/Turabian StyleGeorgakouli, Kalliopi, Alexandra Stamperna, Chariklia K. Deli, Niki Syrou, Dimitrios Draganidis, Ioannis G. Fatouros, and Athanasios Z. Jamurtas. 2020. "The Effects of Postprandial Resistance Exercise on Blood Glucose and Lipids in Prediabetic, Beta-Thalassemia Major Patients" Sports 8, no. 5: 57. https://0-doi-org.brum.beds.ac.uk/10.3390/sports8050057